Page 28 of 35
IM26.34-35 | Infection Communication and Prevention: Counselling, Contact Tracing, and Public Health Measures — SDL Guide
Learning Objectives
- Counsel patients and their families regarding the nature, transmission, isolation requirements, and public health implications of communicable infections
- Describe and apply principles of infection prevention and control — including standard precautions, transmission-based precautions, contact tracing, and outbreak management in community and healthcare settings
INSTRUCTIONS
This SDL uses the IM-skills arc, which focuses on procedural and communication competencies rather than disease knowledge. The six steps of this arc are: (1) indication and preparation, (2) gathering information, (3) performing the skill, (4) follow-up and monitoring, (5) complications and troubleshooting, (6) patient communication and education. For this SDL, the 'skill' is the ability to counsel patients about communicable disease and to apply infection prevention and control principles — including both the interpersonal (one-to-one counselling) and systems-level (outbreak response, contact tracing) dimensions.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 139 — Hospital-Acquired Infections; Ch. 140 — Infection Prevention and Control (textbook)
- WHO Infection Prevention and Control Guidelines 2016; IDSP Guidelines for Integrated Disease Surveillance and Response, India (guideline)
- Park's Textbook of Preventive and Social Medicine, 26th ed. — Communicable Disease Control chapters (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old software professional tests positive for pulmonary tuberculosis during an incidental CXR done for a pre-employment medical. He is in a shared office with 40 colleagues and lives in a 2-bedroom flat with his parents and two younger siblings. He is terrified: he has googled TB and believes he is 'highly contagious' and will need to be 'hospitalised in isolation for months.' His elderly mother arrives at the clinic and asks, 'Will we all get TB? Should we move out of the house?' His HR manager has telephoned to ask whether the patient can return to work after starting medication and whether the office needs to be disinfected. These questions — from the patient, the family, and the employer — will all land on you within the next 30 minutes. You do not have a public health officer to delegate them to. You are the physician, the counsellor, the contact tracer, and the infection control advisor simultaneously. Can you tell the patient accurately how TB is transmitted, when he is no longer infectious after starting treatment, what his family members need, and whether his colleagues need screening? This SDL builds the structured communication skill and infection prevention knowledge that turns these conversations from anxious improvisation into confident, evidence-based clinical practice.
WHY THIS MATTERS
The ability to counsel patients about communicable infections and to apply infection prevention principles is a core clinical competency that directly affects patient outcomes, public health, and community safety. Poor infection counselling leads to missed contact tracing (allowing secondary cases), inadequate isolation adherence (fuelling transmission), stigma-driven non-disclosure (HIV, TB), and non-compliance with treatment (drug resistance). In India, where TB, HIV, dengue, malaria, and the Integrated Disease Surveillance Programme (IDSP) together create a complex communicable disease landscape, every physician is expected to recognise notifiable diseases, initiate appropriate contact tracing, counsel patients and families clearly, and implement infection prevention precautions. The COVID-19 pandemic exposed the consequences of inadequate public health communication and infection control at a national scale. For Indian MBBS graduates, these skills are tested in OSCE stations and are immediately operational on day one of internship — when you will be managing communicable disease patients without specialist supervision.
RECALL
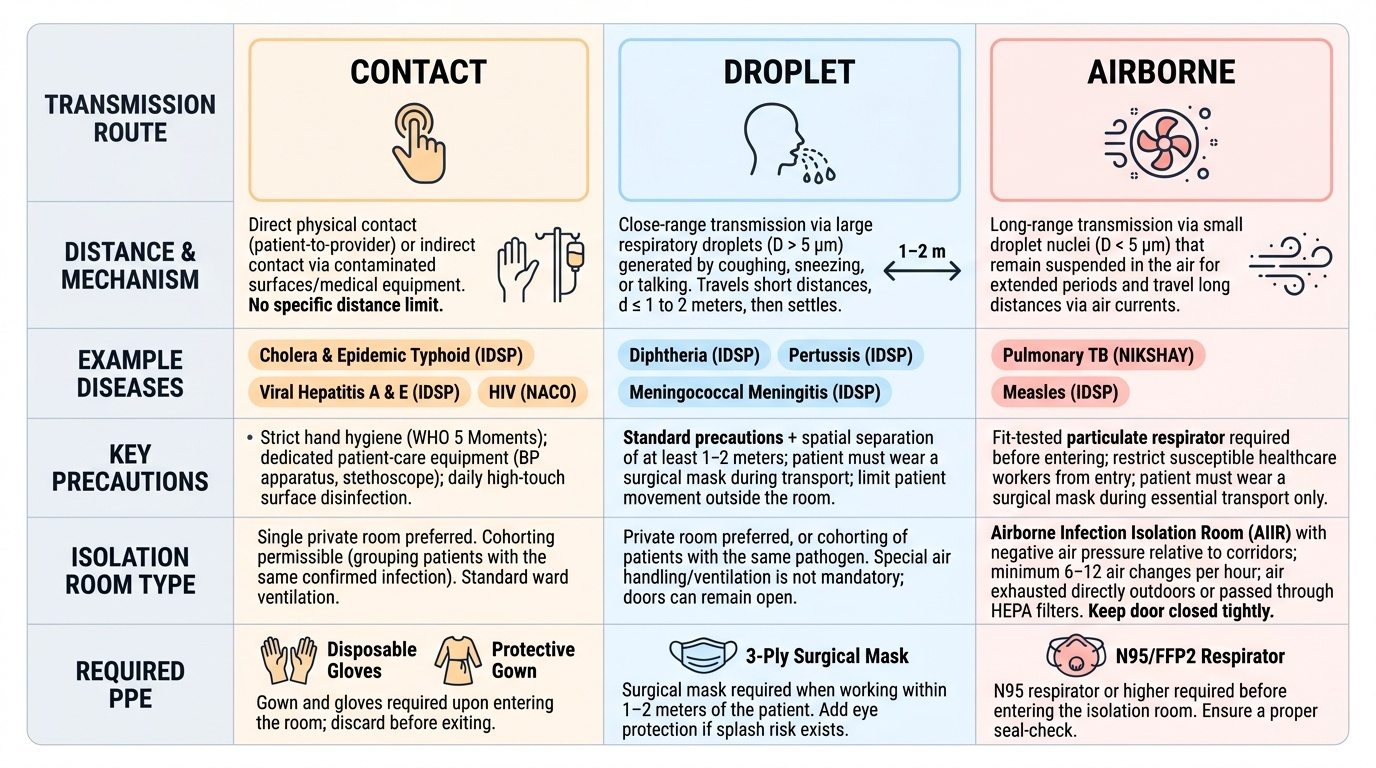
Recall the framework before proceeding. Infection transmission routes determine both the precautions needed and the key counselling messages: contact transmission (direct skin-to-skin or indirect via fomites — impetigo, scabies, MRSA, C. difficile) requires contact precautions (gloves, gown, hand hygiene); droplet transmission (large respiratory droplets >5 µm, travel <1 metre — influenza, meningococcal disease, RSV, pertussis) requires droplet precautions (surgical mask within 1 metre); airborne transmission (droplet nuclei <5 µm, travel >1 metre and remain suspended — TB, measles, varicella/zoster) requires airborne precautions (N95 respirator, negative-pressure isolation room). Standard precautions apply to ALL patients regardless of diagnosis: hand hygiene (5 moments of the WHO framework), gloves for blood/body fluid contact, mask and eye protection for splash risk, safe sharps disposal, respiratory hygiene/cough etiquette. Notifiable diseases in India (under the Integrated Disease Surveillance Programme, IDSP): include cholera, malaria, dengue, kala-azar, Japanese encephalitis, acute flaccid paralysis, rabies, TB (under NIKSHAY programme), HIV, and epidemic-prone diseases — all must be reported to the local health authority.
Indications and Preparation: When Is Infection Counselling and Public Health Reporting Required?
Effective infection prevention and control begins with recognising which clinical situations trigger a structured public health response — not just individual patient treatment. Every physician must know the categories of diseases requiring notification, isolation, and contact tracing, and the process for initiating these responses. In India, this framework is primarily governed by the Integrated Disease Surveillance Programme (IDSP) under the National Centre for Disease Control (NCDC), with parallel programmes for specific diseases (RNTCP/NTEP for TB, NACO for HIV, NVBDCP for vector-borne diseases). A physician who cannot identify which diseases require mandatory reporting, or who defers infection counselling entirely to a public health specialist, fails in a fundamental professional obligation — because in most primary and secondary care settings in India, there is no specialist to defer to, and the responsibility lands squarely with the treating doctor.
Provided image
When infection counselling and public health action is indicated:
- Notifiable diseases: any confirmed or suspected case of a notifiable communicable disease triggers mandatory reporting to the local health authority (district health officer). The list under IDSP includes cholera, typhoid (epidemic-prone clusters), malaria, dengue, kala-azar, Japanese encephalitis, acute flaccid paralysis, rabies, measles, diphtheria, pertussis, meningococcal meningitis, viral hepatitis (A and E — outbreak-prone), and any disease causing an unusual cluster of illness.
- TB and HIV: under the NIKSHAY system, all TB cases (new, previously treated, drug-resistant) must be notified at the time of diagnosis. Under NACO guidelines, HIV diagnosis triggers a specific post-test counselling protocol and partner notification process.
- Healthcare-associated infections (HAIs): any cluster of similar infections in hospitalised patients suggests a potential outbreak requiring infection control investigation.
- Common source outbreaks: two or more cases of similar illness linked by time, place, and exposure (e.g., food poisoning at a function, gastroenteritis cluster in a school) trigger an outbreak investigation.
Preparation for the counselling encounter:
Before the counselling session, the physician must know: (a) the route of transmission (contact, droplet, airborne, faecal-oral, vector-borne, blood-borne) — this determines the isolation requirement and the key counselling message; (b) the incubation period — this determines the contact tracing window; (c) the period of communicability — when is the patient infectious? This determines when isolation can be lifted and when contacts are at risk; (d) the available intervention for contacts (post-exposure prophylaxis, vaccination, or surveillance only); (e) the patient's social context (household composition, occupation, school/workplace setting) — this determines who the contacts are and what practical advice is feasible.
Gathering Information: Taking the Infection Exposure and Social History
The infection prevention assessment requires a structured history that goes beyond the standard medical history to include the epidemiological and social dimensions of the patient's illness. This 'infection-focused social history' is the information-gathering step that defines who the contacts are, how long the exposure window was, and what the risk to others is. Gathering this information sensitively — especially for stigmatised infections like TB and HIV — is a communication skill that requires both accuracy and empathy. The quality of the contact history determines the completeness of the contact tracing intervention: missed contacts are missed opportunities to prevent secondary cases, and in diseases like TB and HIV, each missed contact is a potential new case that will be diagnosed weeks or months later with preventable morbidity.
The infection exposure and contact history — key questions:
For TB:
- Who does the patient live with? (household contacts — highest risk, especially children and immunocompromised)
- Where does the patient work or study? (workplace/school contacts — lower but real risk for prolonged exposure)
- How long has the patient been symptomatic? (defines the exposure window — contacts from symptom onset to start of treatment are at greatest risk)
- Is there any close social contact who is HIV-positive, on immunosuppressants, or an infant/young child? (high-risk contacts who need priority follow-up)
- Has any household contact had unexplained weight loss, cough, or fever recently? (symptom screening for active TB in contacts)
For HIV:
- Sexual contact history: partners in the past 3 months; type of sexual exposure (receptive anal intercourse carries the highest per-act transmission risk — approximately 1–3%); condom use
- Injecting drug use: sharing of needles, syringes, preparation equipment
- Blood product exposure: transfusions, organ transplant
- Occupational exposure (healthcare worker): needle-stick injury, mucous membrane exposure
- Partner notification: who needs to be informed of their potential exposure? This must be done sensitively and within the confidentiality framework.
For foodborne/waterborne outbreaks:
- What food/water was consumed in the 48–72 hours before onset of illness? (incubation period determines the exposure window — Salmonella 12–72 hours, Staphylococcal toxin 2–6 hours, Hepatitis A 15–50 days)
- Did others who consumed the same food also become ill? (defines a common source outbreak)
- Where was the food prepared? (identifies the source for investigation and control)
- Occupation: food handler, healthcare worker, childcare worker? (determines public health urgency)
For vector-borne diseases (malaria, dengue):
- Travel history and residential address: where has the patient been in the past 2–4 weeks? (determines vector exposure area and guides case mapping)
- Mosquito breeding sites nearby: stagnant water containers, coolers, construction sites? (Aedes aegypti breeds in stored clean water — dengue; Anopheles breeds in slow-moving water — malaria)
- Other household members with similar symptoms? (cluster = local transmission)
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
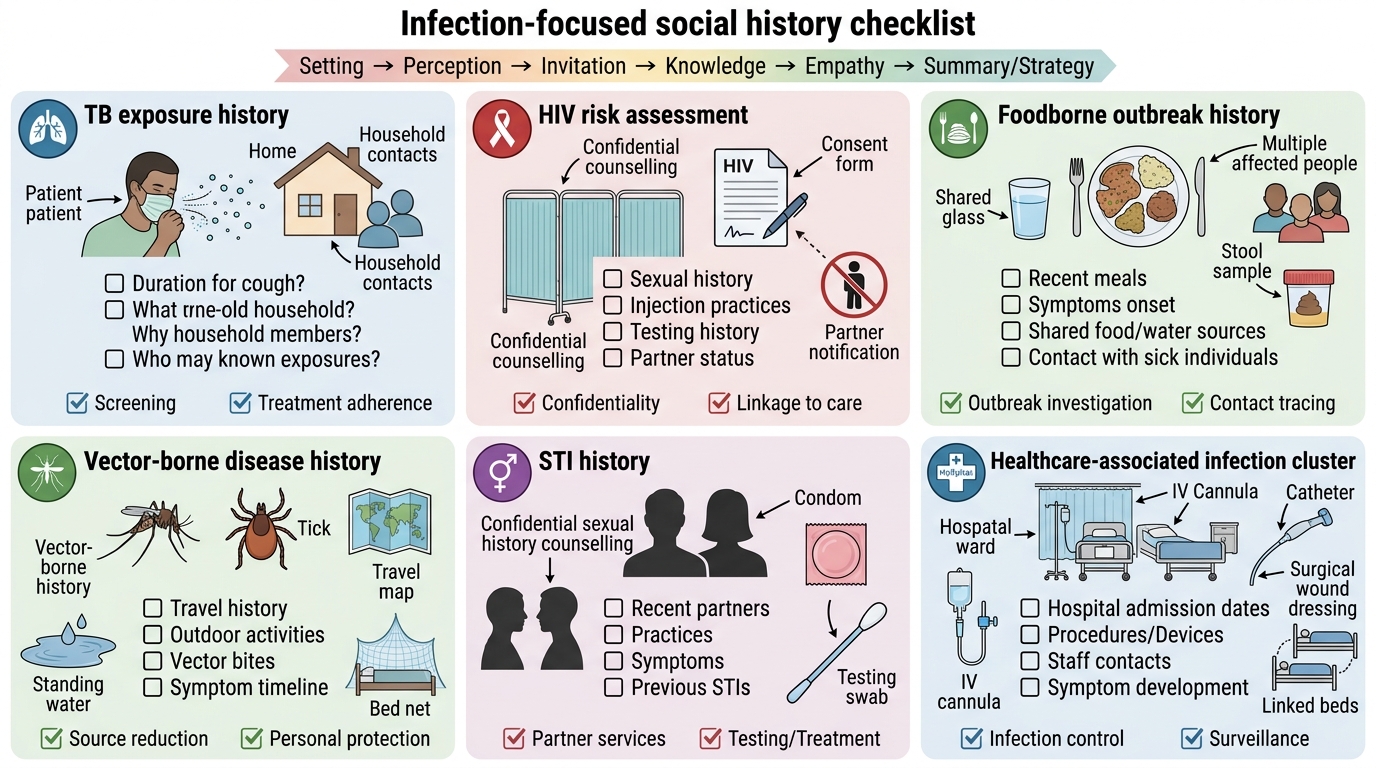
Infection-Focused Social History Checklist
Performing the Skill: Structured Infection Counselling
Structured infection counselling is a communication skill that combines accurate clinical information, empathetic delivery, and actionable public health guidance. Poorly delivered counselling — even when the information is correct — can cause stigma, non-disclosure, and non-adherence. The SPIKES framework (originally developed for breaking bad news) is directly applicable to infectious disease counselling: Setting, Perception, Invitation, Knowledge, Empathy, Summary/Strategy. Adapting this framework to communicable disease contexts — where the patient's private illness has immediate implications for family members, workplaces, and communities — requires comfort with difficult conversations and a non-judgemental communication style.
TB counselling — a worked example:
Setting: Private room, no interruptions; invite a family member if the patient wishes.
Perception: Ask what the patient already knows about TB — 'Many people have heard different things about TB; what do you understand about this disease?' Correct myths before adding new information.
Key messages to deliver accurately:
- 'TB of the lungs (pulmonary TB) spreads through the air — when an infected person coughs, sneezes, or speaks, small particles containing the bacteria can be inhaled by people nearby.'
- 'However, TB is NOT spread by sharing food, cups, or touching the same surfaces.'
- 'Once you start treatment (the combination of four medications — RNTCP/NTEP category-based regimen), you become much less infectious — in most cases, within 2 weeks of starting effective treatment, you are no longer capable of spreading TB to others.'
- 'You do NOT need to be hospitalised in isolation for months. You can be treated at home, as long as the household is well-ventilated.'
- 'Your household contacts (the people who live with you) need to be screened — we will arrange chest X-ray and symptom review for everyone. Children under 5 and HIV-positive contacts will also receive preventive treatment (TB preventive therapy, TPT — isoniazid 6H or 3HP regimen).'
- 'You must continue ALL medications for the full course — 6 months for new cases. Stopping early allows the bacteria to become drug-resistant, which is much harder and more expensive to treat.'
- 'TB is a notifiable disease in India — I am required to report your case to the health authorities, which ensures you receive free treatment under the government programme (NTEP) and follow-up.'
Workplace guidance: 'You can return to work once you have been on effective treatment for 2 weeks and feel well enough. Notify your HR that you have started treatment, but you do not need to disclose the specific diagnosis to your colleagues. Office disinfection is NOT necessary for TB — the bacteria only spread in close, prolonged enclosed spaces.'
HIV post-test counselling — key elements:
- Deliver the result clearly and non-judgementally: 'The result shows that the HIV test is positive. I know this is difficult news.'
- Explain what HIV means in 2025: 'With modern antiretroviral therapy (ART), HIV is a manageable chronic condition — people on ART live near-normal lifespans. This is not a death sentence.'
- Initiation of ART: 'We will start treatment today or very soon — the sooner we start, the better for your immune system and the lower your chance of passing HIV to others.'
- Prevention of onward transmission: 'With effective ART, your viral load becomes undetectable — U=U (Undetectable = Untransmittable). You will not transmit HIV to an HIV-negative partner through sex if your viral load is undetectable.'
- Partner notification: 'I would like to talk with you about informing your partner(s) so they can get tested and, if needed, start pre-exposure prophylaxis (PrEP). This is called partner notification — it is a public health responsibility, and we can help you do it in a confidential and supported way.'
- Confidentiality: HIV status is protected information — it must not be disclosed to the employer without the patient's explicit consent.
Standard precautions — communicating to patients and families:
For all hospitalised patients with communicable infections, clear instructions reduce anxiety and prevent transmission: 'Please use the alcohol hand rub on your way in and out; wear this mask while in the patient's room [if droplet precautions]; do not share the patient's food utensils or personal items; we will place a sign on the door that tells the nurses what precautions to take.'
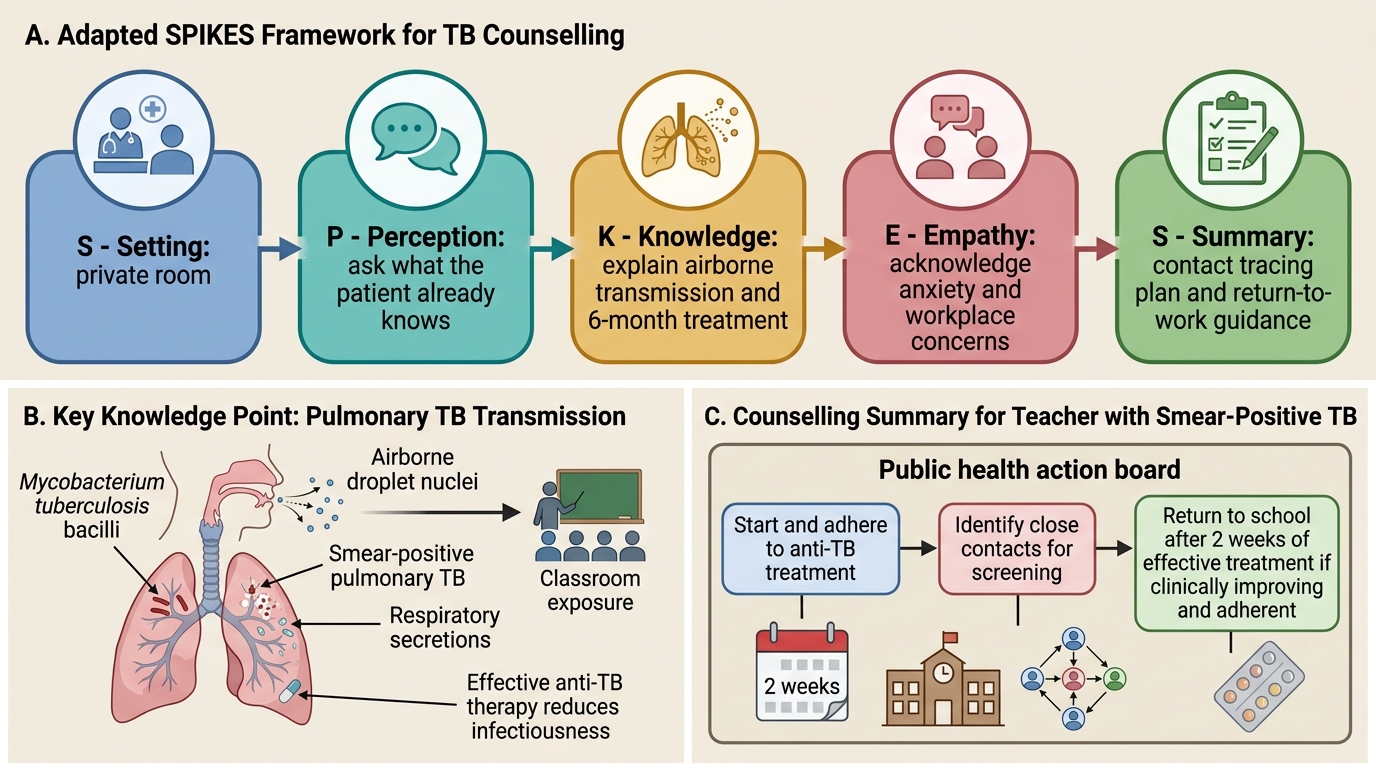
Adapted SPIKES Framework for TB Counselling
SELF-CHECK
A 30-year-old teacher is diagnosed with smear-positive pulmonary tuberculosis. He is concerned about his students and asks when he can safely return to school. Based on RNTCP/NTEP guidelines and standard infection control principles, the MOST accurate advice is:
A. He must not return to school for 6 months — until the full TB treatment course is complete
B. He can return immediately — TB is not airborne and classroom exposure does not pose a risk
C. He can return to school after 2 weeks of effective anti-TB treatment, provided he is clinically improving and adhering to his medication
D. He must wait until two consecutive sputum smear results are negative before returning to school
Reveal Answer
Answer: C. He can return to school after 2 weeks of effective anti-TB treatment, provided he is clinically improving and adhering to his medication
After 2 weeks of effective first-line anti-TB therapy, the infectious bacterial burden in respiratory secretions is dramatically reduced and the patient is considered non-infectious for practical public health purposes. Most guidelines (RNTCP/NTEP, WHO, CDC) allow return to work/school after 2 weeks of effective treatment in smear-positive pulmonary TB, provided the patient is adherent and clinically improving. Requiring 6 months off work is impractical, stigmatising, and not evidence-based. Waiting for two negative smear results is overly restrictive for most settings. Saying 'TB is not airborne' is factually incorrect. For drug-resistant TB (MDR-TB), stricter return-to-work criteria apply, but this is not stated in the question.