Page 29 of 35
IM26.34-35 | Infection Communication and Prevention: Counselling, Contact Tracing, and Public Health Measures — SDL Guide (Part 2)
Follow-Up and Monitoring: Contact Tracing and Post-Exposure Prophylaxis
Effective contact tracing is the cornerstone of communicable disease control — it identifies individuals who have been exposed, assesses their risk, offers testing and prophylaxis where available, and breaks the transmission chain. Contact tracing is a public health skill that every physician must be able to initiate, even if specialist support (district health officer, IDSP surveillance officer) is available for complex outbreaks. The key principle is to define the exposure window precisely (using the incubation period of the disease), identify all contacts within that window who had sufficient exposure, and then prioritise contacts by their risk level and vulnerability.
TB contact tracing — the Indian context:
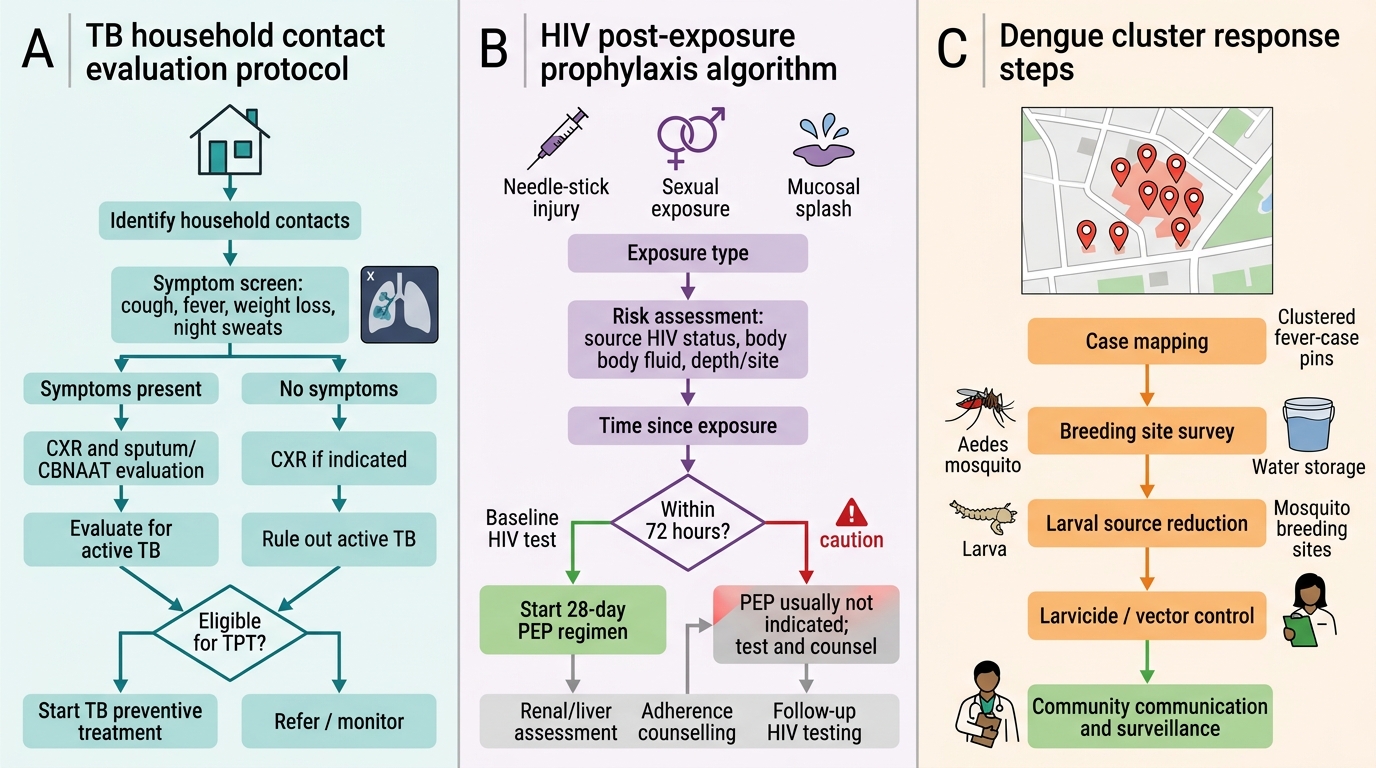
Under NTEP (India), all household contacts of a newly diagnosed smear-positive TB case must be evaluated. The evaluation protocol: (a) symptom screening (cough >2 weeks, fever, night sweats, weight loss) — if symptoms present, sputum TB NAAT/culture; (b) chest X-ray for all contacts; (c) TST (tuberculin skin test) or IGRA if available — not routinely done in all settings under NTEP. TB Preventive Therapy (TPT): indicated for all contacts in high-risk groups: children <5 years (isoniazid 6 months or 3HP regimen regardless of TST result); HIV-positive contacts (isoniazid 6H or 3HP — reduces TB risk by 60%); recently turned-positive TST contacts. School contact tracing for a teacher with TB: screen symptomatic students; CXR for those with cough; no routine TPT for healthy adult school contacts with negative symptoms.
HIV post-exposure prophylaxis (PEP):
PEP must be started within 72 hours of exposure (ideally within 2 hours) and continued for 28 days. Standard PEP regimen in India (NACO guidelines): tenofovir + lamivudine + lopinavir/ritonavir (or dolutegravir-based regimen — preferred in current guidelines). PEP reduces HIV transmission risk by >80% if started early and completed fully. Exposures warranting PEP: needle-stick injury from HIV-positive source (per-act risk: hollow-bore needle ~0.3%); unprotected receptive anal intercourse with HIV-positive partner (~1–3% per act); rape/sexual assault. Do NOT delay PEP to await HIV test of source patient — start empirically if source is known or suspected HIV-positive.
Dengue/malaria outbreak response:
For vector-borne diseases, contact tracing involves mapping cases geographically to identify the transmission zone. The public health response: (a) notify the NVBDCP/IDSP; (b) active case finding — fever survey in the affected area; (c) larval source reduction — identify and eliminate mosquito breeding sites within 100–200 metres of the case cluster; (d) focal indoor residual spraying (IRS) for malaria; (e) community education on mosquito prevention (repellents, long sleeves, mosquito nets, emptying standing water).
Healthcare-associated infection (HAI) outbreak response:
A cluster of similar infections in hospitalised patients (e.g., three ICU patients developing carbapenem-resistant Klebsiella bacteraemia in 2 weeks) triggers an outbreak investigation: (a) identify the case cluster; (b) implement contact precautions for all colonised/infected patients; (c) screen ICU healthcare workers for carriage (nasal swab, rectal swab for ESBL/CRE); (d) deep cleaning and disinfection of shared equipment; (e) audit hand hygiene compliance; (f) reinforce standard precautions; (g) consult infection control team.
Contact Tracing Action Plan for TB, HIV Exposure, and Dengue
Complications, Troubleshooting, and Challenging Scenarios
Infection counselling and public health communication involve not only delivering information but navigating the emotional, social, and ethical complexities that arise when patients face stigmatised, notifiable, or highly transmissible infections. Anticipating and handling these challenging scenarios is part of the clinical skill.
Challenging scenarios and how to handle them:
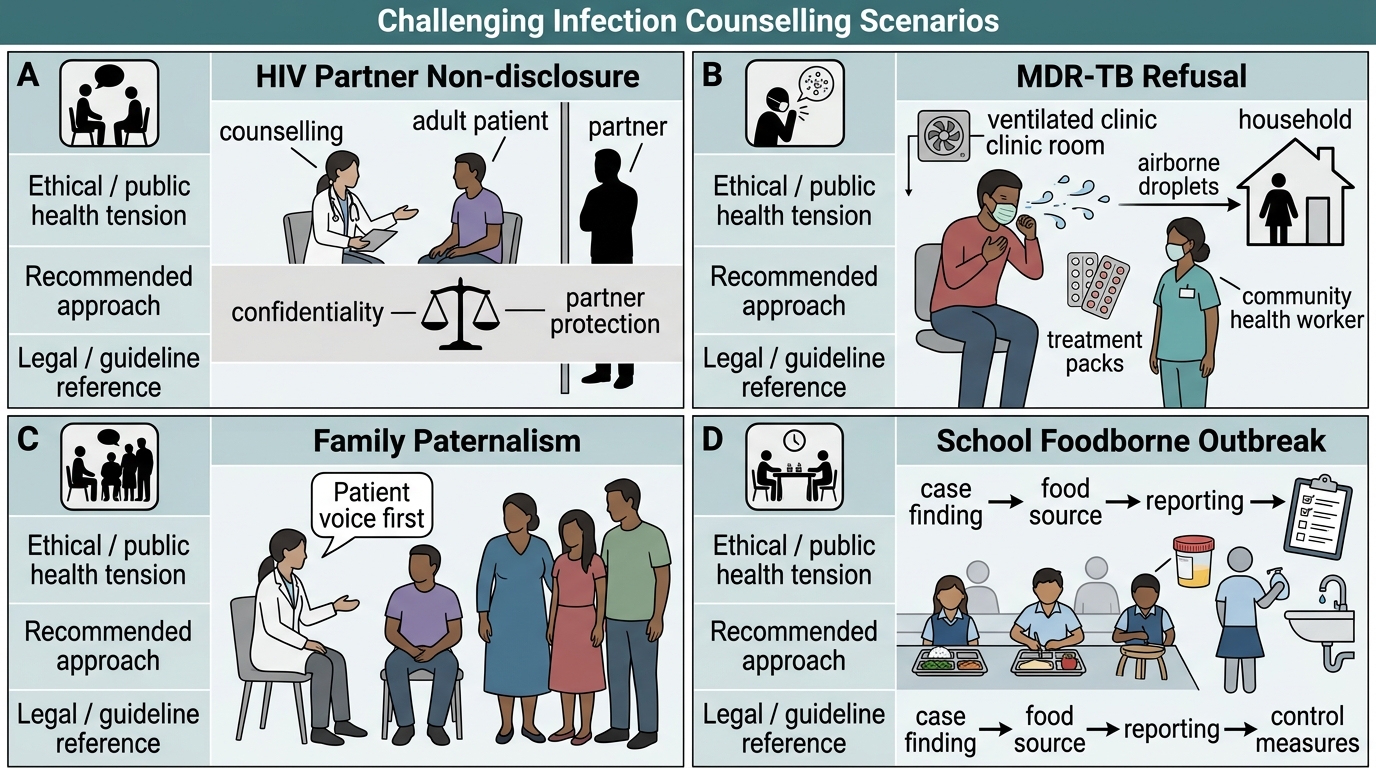
Scenario: The patient refuses to disclose HIV status to their sexual partner. The tension between patient confidentiality and the partner's right to know their exposure risk is one of the most difficult ethical situations in HIV care. The approach: (a) Explore the patient's fears — discrimination, rejection, violence; acknowledge these are real risks in the Indian social context; (b) Counsel about U=U (Undetectable = Untransmittable) — starting ART and achieving viral suppression is the most effective way to protect the partner; (c) Offer assisted partner notification — many ICTC (Integrated Counselling and Testing Centre) facilities provide confidential partner notification services where the patient is not directly identified; (d) If the patient absolutely refuses and a high-risk partner is identifiable, seek guidance from the ICTC counsellor and the hospital ethics committee — there is a public health duty to warn vs. patient confidentiality, and the legal framework in India (Clinical Establishments Act, not a specific HIV disclosure law) is evolving.
Scenario: A patient with MDR-TB refuses hospitalisation and continues working in a crowded school. MDR-TB (rifampicin-resistant TB) requires prolonged treatment and carries a high risk of transmission to contacts. If the patient refuses admission and continues to work in a high-risk setting, the physician must: (a) clearly document the counselling and the risk communicated; (b) notify the district TB officer (mandatory under NTEP); (c) the district health officer has legal authority under the Epidemic Diseases Act, 1897 (and state epidemic disease acts) to enforce isolation when public health risk is demonstrated. However, compulsory isolation is a last resort and should be preceded by all reasonable counselling attempts.
Scenario: A family demands that the diagnosis of TB be withheld from the patient (a paternalistic family request common in Indian clinical practice). Guidance: the patient has the right to know their own diagnosis. The physician's duty is to the patient, not to the family. However, the manner and pace of disclosure can be sensitive to cultural context. Discuss with the family the importance of the patient's informed consent to treatment — without disclosure, the patient cannot give informed consent. The family's role is supportive, not gatekeeping.
Scenario: An outbreak of watery diarrhoea affects 45 students at a school after a mid-day meal. Outbreak investigation steps: (a) confirm the outbreak (two or more cases of similar illness linked by time and place); (b) develop a case definition (watery diarrhoea + nausea + onset within 24 hours of eating at the school cafeteria); (c) count cases and draw an epidemic curve; (d) identify the suspected source (which food items were consumed; stool samples from ill students; food samples from kitchen); (e) implement control measures (suspend the suspected food item; strengthen kitchen hygiene; provide ORS); (f) report to IDSP; (g) environmental health inspection of the kitchen. Cholera (if suspected from rice water stools) is a notifiable epidemic-prone disease requiring immediate reporting.
Challenging Infection Counselling Scenarios
Patient Communication and Education: Infection Prevention in Practice
The final step of the IM-skills arc — patient communication and education — involves translating infection prevention principles into practical, accessible guidance for patients and their families. This step requires communication skills adapted to the patient's health literacy, language, and social context, and it closes the loop from diagnosis to safe community reintegration.
Health literacy and communicating infection risk: Medical terminology creates barriers. Replace: 'airborne transmission' with 'the bacteria/virus travels in the air on tiny droplets from coughing'; 'droplet precautions' with 'wear this mask and stand more than an arm's length away'; 'contact transmission' with 'the infection spreads by touching — wash your hands after contact with the patient'. Use teach-back method: 'Can you tell me in your own words what you will do when you get home to prevent spreading this to your family?' — confirm understanding before ending the consultation.
Standard prevention messages for common infections:
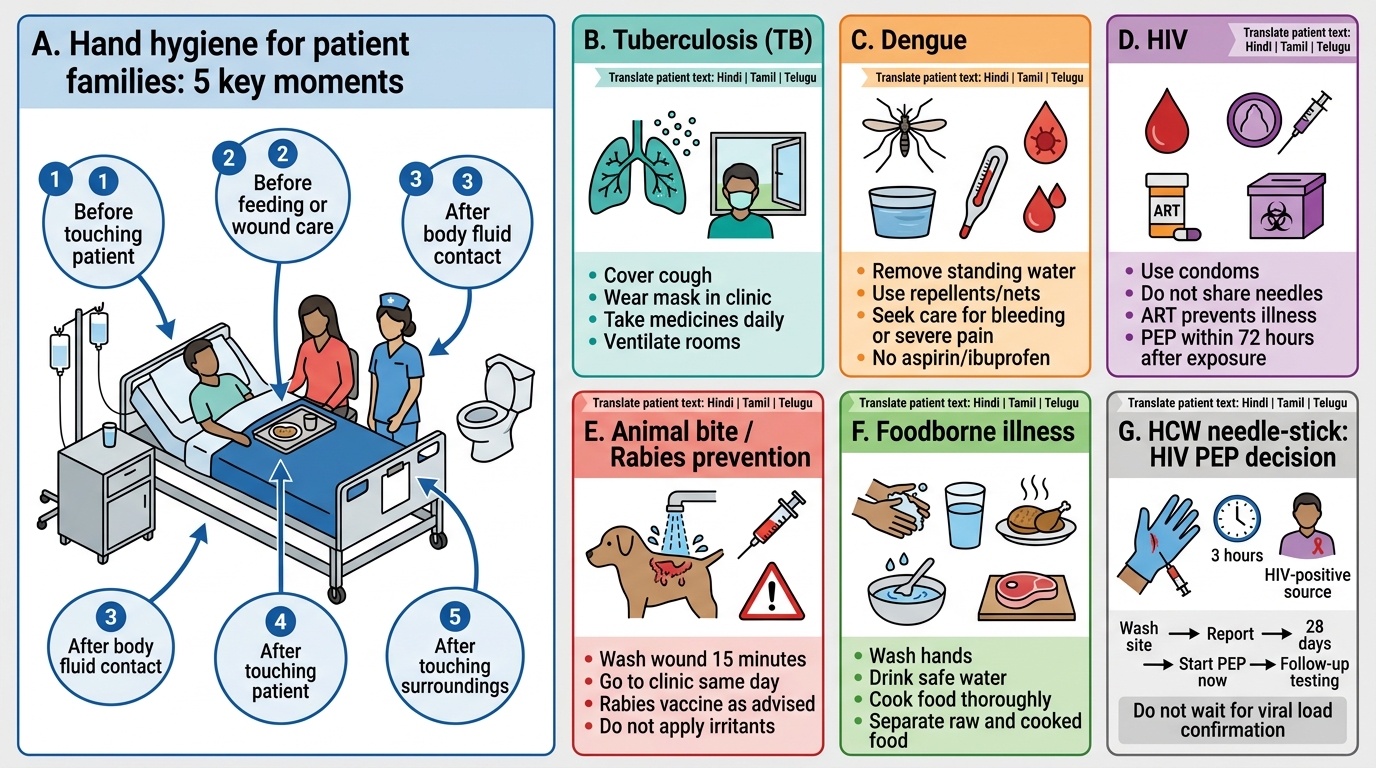
TB: ventilate the bedroom well (open windows); sleep in a separate room until 2 weeks of treatment; cover mouth when coughing (cough etiquette); dispose of used tissues safely. No need to isolate in a separate house or disinfect surfaces.
Dengue: eliminate all standing water — empty coolers, flower vases, plant saucers, outdoor containers every 3–4 days; use bed nets and repellents (DEET-containing); wear long-sleeved clothing during the day (Aedes aegypti bites during the day, not night). Educate on warning signs: bleeding, severe abdominal pain, persistent vomiting, restlessness after fever breaks — return immediately. Do NOT take aspirin or ibuprofen for dengue fever (risk of haemorrhage).
HIV: consistent condom use; partner testing; ART adherence (goal = viral suppression → U=U); do not share needles; do not donate blood; the patient may breastfeed ONLY if on suppressive ART (Option B+ of PMTCT).
Rabies (animal bite): wash wound immediately with soap and water ×15 minutes; come to the clinic for PEP; complete the full vaccine schedule; Category III bite requires RIG on day 0. Educate that a 'healthy-looking' dog can still carry rabies in India — if in doubt, Category III PEP should not be delayed.
Hand hygiene — the most powerful infection prevention intervention: The WHO '5 Moments of Hand Hygiene' framework must be taught to patients visiting family members in hospital: before touching the patient, before clean/aseptic procedures, after body fluid exposure, after touching the patient, and after touching patient surroundings. Alcohol-based hand rub (ABHR) is effective in 20–30 seconds and is superior to soap and water for most organisms except C. difficile spores and norovirus (use soap and water for these).
Immunisation as infection prevention: For contacts of vaccine-preventable diseases — measles, meningococcal disease, hepatitis B, varicella — post-exposure vaccination (where within window) or pre-exposure vaccination of identified close contacts is a preventive intervention. Review the patient's own immunisation status and recommend catch-up vaccines where indicated. In India, the Universal Immunisation Programme (UIP) covers BCG, hepatitis B, polio, DTP, Hib, pneumococcal, rotavirus, MMR, typhoid (in high-burden states), and JE (in endemic areas). Adult vaccines often missed: hepatitis B (healthcare workers), influenza, typhoid, varicella, HPV.
Infection Prevention Patient Education Cards
SELF-CHECK
A healthcare worker sustains a needle-stick injury from a hollow-bore needle that was used to draw blood from a known HIV-positive patient with an undetectable viral load on ART. The needle-stick occurred 3 hours ago and the HCW has not yet received HIV PEP. What is the MOST appropriate course of action?
A. No PEP is required — the source patient has an undetectable viral load, which makes transmission risk negligible
B. Start HIV PEP immediately (within the 72-hour window) and continue for 28 days, since the source is HIV-positive regardless of viral load, and PEP is the standard of care for Category III occupational exposures
C. Wait for the source patient's HIV viral load confirmation report before deciding on PEP
D. Only HIV testing of the HCW is needed; PEP is not standard practice for healthcare workers in India
Reveal Answer
Answer: B. Start HIV PEP immediately (within the 72-hour window) and continue for 28 days, since the source is HIV-positive regardless of viral load, and PEP is the standard of care for Category III occupational exposures
PEP should be started immediately for a hollow-bore needle-stick injury from an HIV-positive source, regardless of the source's viral load. Although U=U (Undetectable = Untransmittable) substantially reduces transmission risk in sexual exposure, it does not fully apply in the context of occupational needle-stick injuries, and PEP is the standard of care for confirmed HIV-positive source exposures in healthcare settings (NACO guidelines, WHO 2016). PEP must be started within 72 hours (ideally within 2 hours) and continued for 28 days. Waiting for viral load confirmation wastes critical time — PEP effectiveness falls sharply beyond 24 hours. The standard regimen in India: tenofovir + lamivudine + lopinavir/ritonavir (or dolutegravir-based).
CLINICAL PEARL
Three critical clinical pearls for infection communication and prevention: (1) TB transmission counselling: 'Two weeks of effective treatment, not six months' — after 2 weeks of first-line anti-TB therapy, a smear-positive pulmonary TB patient is no longer considered infectious for practical purposes. Overcorrecting this myth prevents unnecessary stigma, job loss, and social isolation. (2) HIV PEP has a hard 72-hour window — but the earlier the better (ideally within 2 hours). Do not wait for the source patient's HIV test result to start PEP; if the source is known or strongly suspected HIV-positive, start empirically. (3) Dengue patient education must include 'Do NOT take ibuprofen or aspirin for fever' — these are the most commonly taken OTC medications in India for fever, yet they significantly increase bleeding risk in dengue and can precipitate dengue shock syndrome.