Page 1 of 35
IM26.1-7 | Infectious Disease Approach — SDL Guide
Learning Objectives
- Describe the molecular mechanisms underlying microbial pathogenesis including virulence factors, toxins, and host immune evasion strategies
- Apply a structured clinical approach to a patient presenting with suspected infectious disease
- Elicit an infection-focused history covering symptom evolution, exposure history, occupational and travel risk factors
- Perform a systematic examination targeting signs of infection including skin, mucosal, lymph node, chest, liver, and spleen
- Order and interpret a core diagnostic panel for infectious disease including CBC with differential, blood cultures, peripheral smear, urinalysis, CSF, and CXR
- Enumerate the indications for newer diagnostic techniques such as PCR, antigen detection, and next-generation sequencing
- Describe a systematic approach to the acutely ill febrile patient incorporating severity scoring and empirical management principles
INSTRUCTIONS
This module builds the cognitive architecture for approaching any patient with suspected infectious disease. Rather than memorising isolated facts, you will construct a framework: understanding how microbes cause disease, how to systematically identify the likely pathogen from history and examination, and how to select and interpret the right investigations. This framework underpins every specific infection SDL that follows in the cluster.
References
- Harrison's Principles of Internal Medicine, 21st ed., Part 7 — Infectious Diseases (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 13 — Infectious Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM in the emergency department. A 38-year-old agricultural worker is brought in with three days of high fever, rigors, severe headache, and now altered consciousness. His wife mentions he worked near a waterlogged field during the monsoon. Examination reveals jaundice, conjunctival suffusion, and a tender, enlarged liver. Another patient in the same waiting area — a 24-year-old student returning from Rajasthan — has had a week of remittent fever, relative bradycardia, a faint rash on the trunk, and mild splenomegaly. These two patients have fever and altered mentation, but they need entirely different investigations, different antibiotics, and different timelines for empirical treatment. The physician who reaches for paracetamol and a generic antibiotic for both has failed both patients. The physician who can read the clinical story — the exposure, the pattern of fever, the organ signs — and translate it into a focused differential before any test returns: that physician saves lives. This module teaches you to become that physician.
WHY THIS MATTERS
Infectious diseases account for the single largest burden of hospitalisation and mortality in India. Malaria, enteric fever, leptospirosis, dengue, tuberculosis, and sepsis from Gram-negative organisms compete for the final-year physician's attention simultaneously, often with overlapping presentations. The ability to reason about infection at a mechanistic level — to know why a pathogen causes the pattern it does — transforms memorisation into understanding and allows you to manage novel or atypical presentations. The NMC competencies IM26.1–IM26.7 target this foundational skill set: pathogenesis, clinical approach, history, examination, investigations, and management of the acutely ill febrile patient. These competencies form the shared platform for all 8 SDLs in this cluster.
RECALL
Activate your prior knowledge before building on it. From microbiology: recall that viruses are obligate intracellular parasites that exploit host-cell machinery for replication; bacteria exist in planktonic and biofilm states and many secrete toxins that mediate disease at sites remote from infection; fungi and parasites exploit gaps in immune surveillance. From physiology: recall that fever is a cytokine-mediated response — IL-1, IL-6, and TNF-α act on the hypothalamic thermostat via prostaglandin E₂; this is a host defence mechanism, not merely a symptom to be suppressed. From pharmacology: recall the principle that antibiotic selection depends on identifying the likely organism, its susceptibility profile, and the drug's tissue penetration at the site of infection. From pathology: recall that the inflammatory response — though protective — is also the mechanism of organ damage in severe sepsis and meningitis. These foundations underpin everything in this module.
Molecular Mechanisms of Microbial Pathogenesis
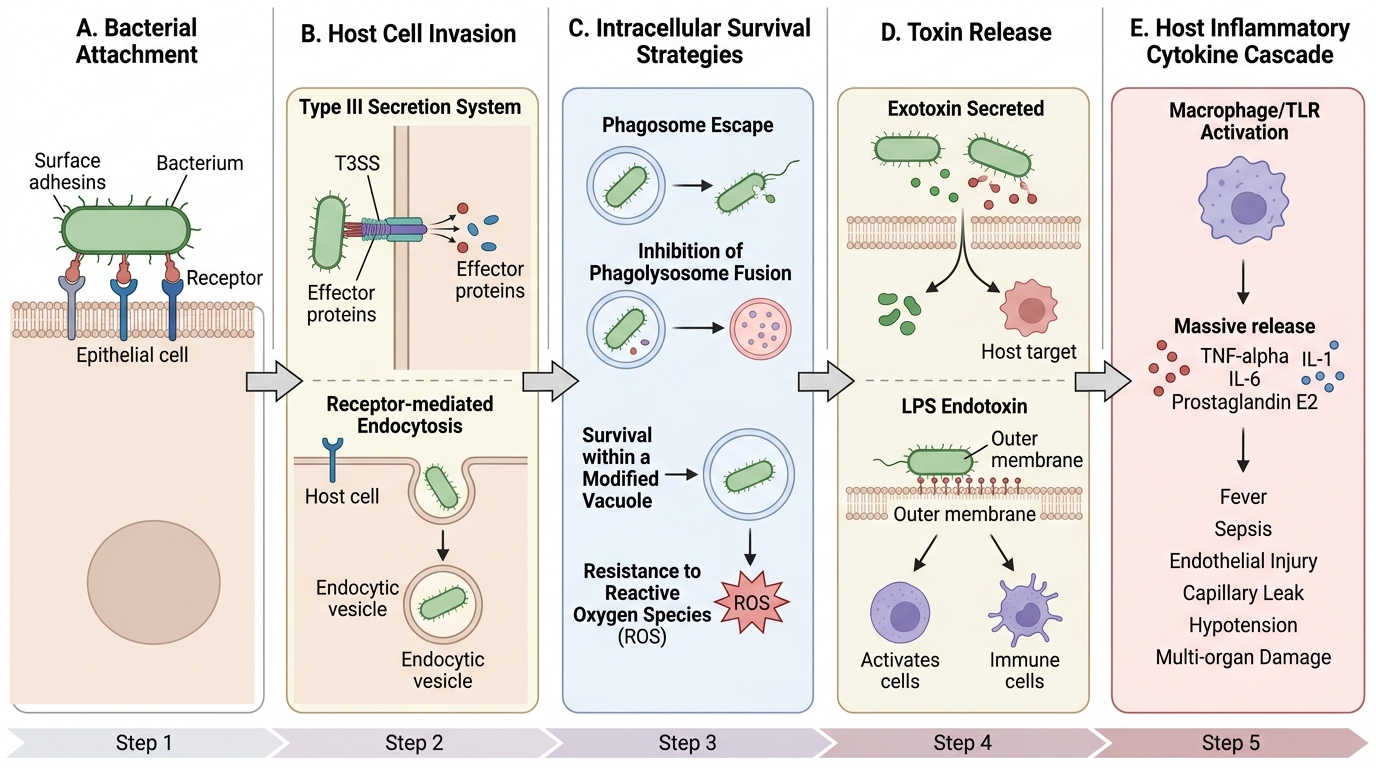
Microbial pathogenesis is the study of how microorganisms cause disease in the host. At the molecular level, pathogenesis involves a sequence of steps: entry and attachment, tissue invasion, evasion of host defences, acquisition of nutrients, and ultimately the injury that produces clinical disease. Understanding these steps allows the clinician to predict the syndrome that a pathogen will produce and to identify points at which therapeutic or preventive intervention is possible.
Adherence and colonisation are the obligatory first steps for virtually all pathogens. Bacteria express surface molecules called adhesins — such as pili (fimbriae), surface proteins, and lipopolysaccharide — that bind to specific host-cell receptors. Uropathogenic Escherichia coli, for example, uses type-1 fimbriae to bind mannose residues on uroepithelium, which is why it preferentially infects the bladder. Disruption of the normal host microbiome (e.g., by antibiotics or mucosal injury) removes competitive colonisation resistance and facilitates pathogen entry, explaining why Clostridium difficile infection follows antibiotic use.
Invasion describes the penetration of host tissue barriers. Obligate intracellular organisms such as Salmonella typhi use a type-III secretion system — effectively a molecular syringe — to inject effector proteins into enterocytes, inducing macropinocytosis and facilitating cellular entry. Listeria monocytogenes exploits the actin cytoskeleton to move intracellularly and spread from cell to cell without exposure to extracellular antibodies. Viruses enter cells via receptor-mediated endocytosis (e.g., SARS-CoV-2 binding ACE2 via its spike protein) or membrane fusion.
Toxin production is a dominant virulence mechanism for many bacteria. Toxins are classified as exotoxins (secreted proteins) or endotoxin (lipopolysaccharide — LPS — released from Gram-negative bacterial cell walls on death or during infection):
- Exotoxins: most are proteins that damage host cells by enzymatic action or receptor binding. Examples: cholera toxin (activates adenylate cyclase, producing massive secretory diarrhoea), tetanospasmin (blocks inhibitory neurotransmitter release in spinal cord → spastic paralysis), botulinum toxin (cleaves SNARE proteins at neuromuscular junction → flaccid paralysis), Shiga toxin of E. coli O157 (inhibits protein synthesis in endothelium → haemolytic uraemic syndrome).
- Endotoxin (LPS): triggers the innate immune system via TLR-4 on macrophages, inducing massive cytokine release (IL-1β, TNF-α, IL-6, IL-8). When endotoxin load overwhelms regulatory mechanisms, the result is septic shock — distributive shock with endothelial dysfunction, capillary leak, coagulopathy, and multi-organ failure.
Immune evasion strategies extend the survival of pathogens in the host. Streptococcus pneumoniae uses its polysaccharide capsule to resist phagocytosis. Staphylococcus aureus produces protein A, which binds the Fc portion of IgG antibodies and prevents opsonisation. Mycobacterium tuberculosis inhibits phagosome–lysosome fusion within macrophages, surviving intracellularly for years. Viruses downregulate MHC class I expression to evade cytotoxic T-cell killing. Plasmodium falciparum undergoes antigenic variation of its surface proteins (PfEMP1), continuously escaping antibody-mediated clearance.
Biofilm formation is critical to understanding chronic and device-associated infections. Bacteria in biofilms are encased in a self-produced polysaccharide matrix, rendering them 100–1000-fold more resistant to antibiotics than planktonic bacteria and largely impervious to host immune cells. This explains why prosthetic joint infections, catheter-associated urinary tract infections, and endocarditis on prosthetic valves require prolonged antibiotic courses or device removal rather than short-course treatment.
Molecular Pathogenesis of Bacterial Infection
Clinical Approach to the Infectious Disease Patient: History
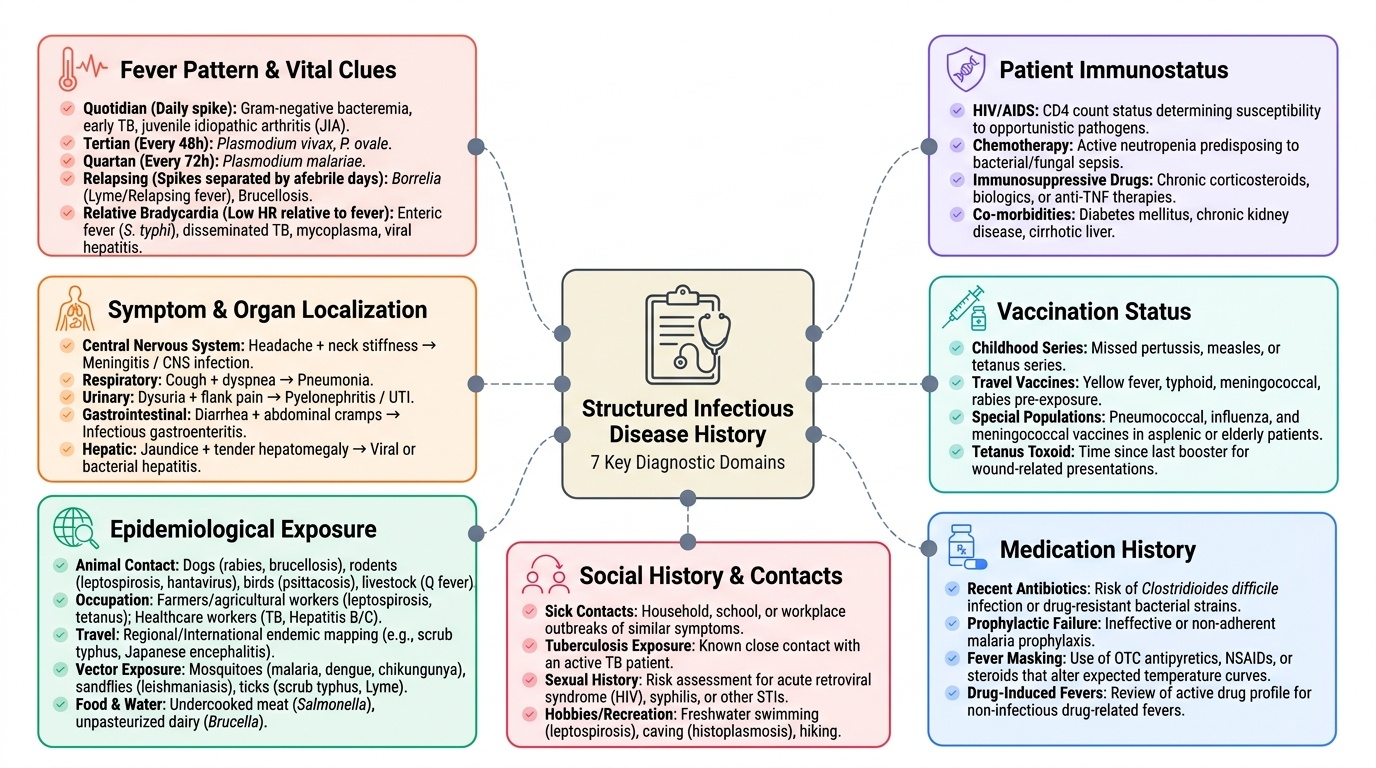
The history in infectious disease is a diagnostic instrument of remarkable precision. Unlike many chronic diseases where the history establishes a pattern over years, in infection the history captures a story that unfolds over days to weeks — and the details of that story frequently point to the diagnosis before a single test is ordered. A structured, infection-focused history covers seven domains:
Provided image
1. Symptom characterisation: Fever is the cardinal symptom of infection but its pattern is informative. A quotidian fever (daily spike returning to baseline) suggests Gram-negative bacteraemia, early TB, or juvenile idiopathic arthritis. Tertian fever (spike every 48 hours) is classic for Plasmodium vivax or P. ovale; quartan fever (every 72 hours) for P. malariae. Relapsing fever (days of fever separated by afebrile periods) characterises Borrelia infection or Brucellosis. Relative bradycardia — heart rate lower than expected for the degree of fever — is a valuable clue for enteric fever (Salmonella typhi or paratyphi), disseminated TB, mycoplasma, and viral hepatitis. The accompanying symptoms determine the organ system: headache + neck stiffness → CNS; cough + dyspnoea → respiratory; dysuria + flank pain → urinary; diarrhoea + abdominal cramps → GI; jaundice + tender hepatomegaly → hepatic.
2. Exposure and epidemiological history: This is the most frequently omitted domain and yet often the most diagnostically decisive. Ask systematically about:
- Animal contact: dogs (rabies, brucellosis), rodents (leptospirosis, plague, hantavirus), birds (psittacosis), cattle/goats/sheep (brucellosis, Q fever)
- Occupation: farmers and agricultural workers exposed to waterlogged soil or animal products are at risk for leptospirosis, tetanus, and zoonoses; healthcare workers for TB, hepatitis B/C
- Travel: domestic travel within India — North India (Brucellosis, plague), Northeast India (scrub typhus, Japanese encephalitis), coastal India (leptospirosis, cholera); international travel raises the differential for tropical diseases endemic elsewhere
- Vector exposure: mosquito bites (malaria, dengue, chikungunya, filariasis), sandfly bites (leishmaniasis), tick bites (scrub typhus, Lyme disease in travellers)
- Food and water: consumption of undercooked meat (Salmonella, tapeworm), unpasteurised dairy (brucellosis), street food (typhoid), contaminated water sources (cholera, typhoid, hepatitis A)
- Sexual history and intravenous drug use: relevant to HIV, hepatitis B/C, STIs
3. Immunocompromise history: The organism spectrum broadens dramatically with impaired immunity. HIV/AIDS (opportunistic infections: Pneumocystis jirovecii pneumonia, CMV retinitis, cryptococcal meningitis, Toxoplasma encephalitis); corticosteroid or immunosuppressant use (Aspergillosis, Mucormycosis, TB reactivation); diabetes (mucormycosis, emphysematous pyelonephritis, necrotising fasciitis); asplenia (encapsulated organisms — Pneumococcus, Haemophilus influenzae, Neisseria meningitidis).
4. Vaccination history: Marks of protection — BCG scar for TB, hepatitis B immunisation, meningococcal vaccine — and unprotected vulnerabilities.
5. Medication history: Prior antibiotics (selects resistant organisms, predisposes to C. difficile), proton pump inhibitors (reduce gastric acid barrier, increase susceptibility to Salmonella and C. difficile), immunosuppressants.
6. Contact history: Close contacts with TB, COVID-19, meningococcal disease, viral haemorrhagic fever.
7. Review of systems: A rapid organ-system sweep may uncover a second focus of infection or a complication of the presenting illness that alters severity assessment and management.
Systematic Physical Examination in Infectious Disease
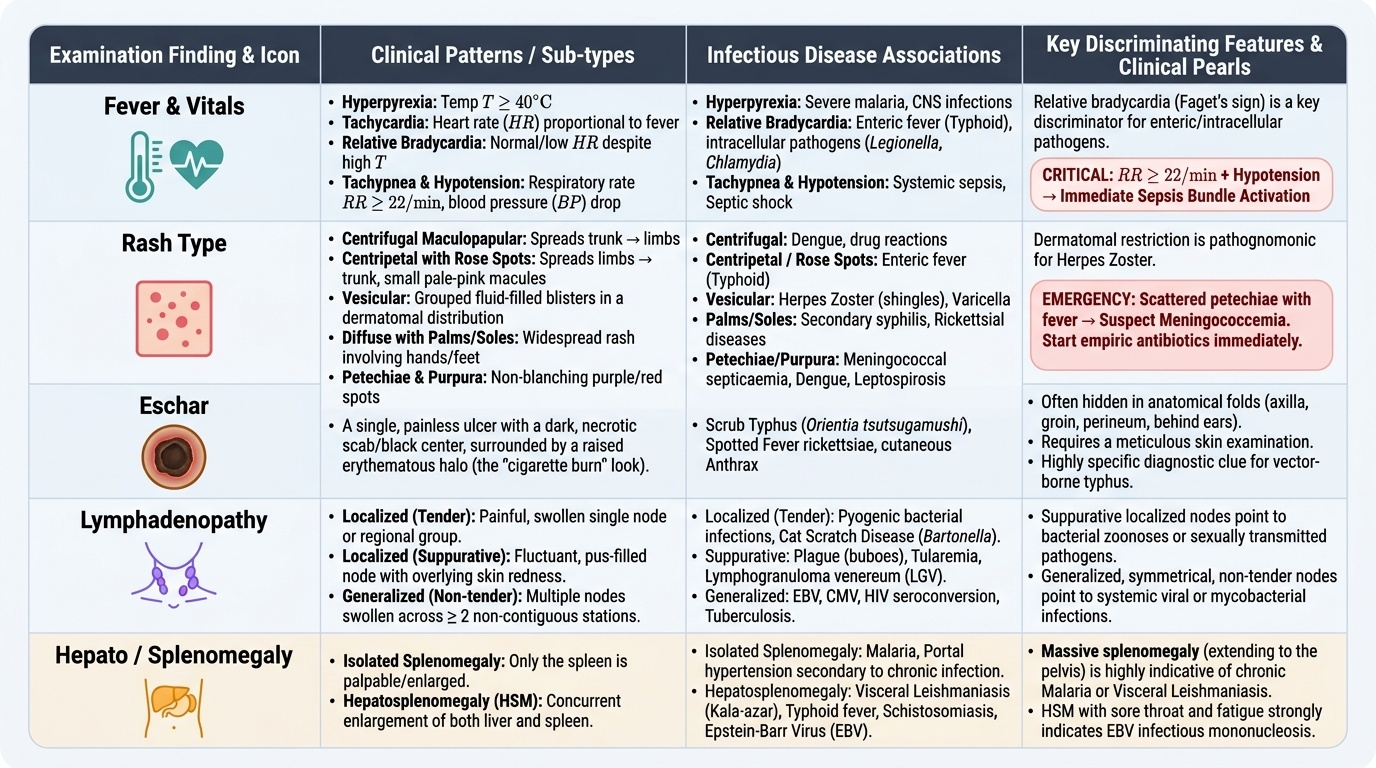
The physical examination in infectious disease is directed by the history but must be systematic to avoid missing the pathognomonic sign that unlocks the diagnosis. The examination follows the general-to-specific sequence: general inspection and vital signs first, then organ-targeted examination informed by the clinical hypothesis. Several examination domains deserve particular emphasis in infection because they are both high-yield and frequently performed incompletely.
Provided image
Vital signs and severity: Temperature (≥38.3°C = fever; ≥40°C = hyperpyrexia), heart rate (tachycardia = sepsis; relative bradycardia = enteric fever/intracellular pathogens), blood pressure (hypotension = septic shock requiring urgent intervention), respiratory rate (≥22/min = one of the qSOFA criteria for sepsis identification), oxygen saturation (SpO₂ <94% = significant respiratory compromise). Together, these define whether the patient is stable for standard assessment or requires immediate resuscitation and sepsis-bundle activation.
Skin and mucosal examination: The skin is an underutilised diagnostic window in infection. Look systematically for:
- Exanthem distribution and morphology: centrifugal maculopapular rash spreading from trunk → limbs (dengue, drug reaction); centripetal maculopapular with rose spots (enteric fever); vesicular grouped dermatomal distribution (herpes zoster); diffuse erythematous maculopapular with palm and sole involvement (scrub typhus eschar on the primary lesion; also secondary syphilis, rickettsial disease)
- Petechiae and purpura: scattered petechiae with fever = meningococcal septicaemia (a medical emergency — diagnose before rash becomes confluent); thrombocytopenic purpura in dengue or leptospirosis; splinter haemorrhages in infective endocarditis
- Eschar: a painless black eschar at the site of tick/chigger bite is the hallmark of scrub typhus (Orientia tsutsugamushi); search carefully in the groin, axillae, belt line, and hairline where the bite is often hidden
- Jaundice: scleral icterus (leptospirosis, viral hepatitis, falciparum malaria with haemolysis, enteric fever complications)
- Conjunctival suffusion: bilateral non-purulent conjunctival injection without discharge, characteristic of leptospirosis
- Oral mucosal findings: koplik spots (measles — small white spots on buccal mucosa opposite the molars, appearing just before the exanthem); oropharyngeal membrane (diphtheria); thrush (candidiasis in immunocompromised); aphthous ulcers (HIV)
Lymph node examination: Palpate all nodal regions systematically. Tender localised lymphadenopathy = reactive to a regional infection (e.g., inguinal adenopathy + genital ulcer = chancroid or syphilis; cervical adenopathy + pharyngitis + splenomegaly = EBV). Generalised lymphadenopathy (>2 regions) = systemic illness: HIV, EBV, CMV, secondary syphilis, systemic TB, lymphoma (non-infectious differential). Discrete, hard, fixed nodes suggest malignancy rather than infection. Tender, fluctuant nodes suggest suppurative bacterial lymphadenitis — possibly requiring drainage.
Chest examination: Dullness to percussion + bronchial breathing or crackles = consolidation (pneumonia); stony dullness + absent breath sounds = pleural effusion (empyema, TB). Wheeze in an immunocompromised patient with fever may indicate Pneumocystis or allergic bronchopulmonary aspergillosis. Crackles in a returning traveller with fever = melioidosis, Q fever, or atypical pneumonia.
Abdominal examination (hepatosplenomegaly): The liver is enlarged in viral hepatitis (tender, smooth), amoebic liver abscess (tender, smooth, may be dull with right-side diminished breath sounds if subphrenic), and right heart failure from sepsis. The spleen is the organ most closely associated with systemic infection — it is the body's largest filter of the bloodstream. Splenomegaly in a febrile patient narrows the differential substantially: malaria (especially P. vivax), enteric fever (Salmonella species), viral infections (EBV, CMV, viral hepatitis), kala-azar (massive splenomegaly — spleen reaching the right iliac fossa), leptospirosis, brucellosis, and infectious endocarditis. Spleen size should be measured in centimetres below the left costal margin in the right lateral position.
SELF-CHECK
A 28-year-old farmer from coastal Karnataka presents with 5 days of fever, severe myalgia, jaundice, and conjunctival suffusion after working in a waterlogged paddy field. The single most discriminating examination finding pointing to leptospirosis rather than viral hepatitis is:
A. Tender hepatomegaly
B. Jaundice with pale stools
C. Bilateral conjunctival suffusion (non-purulent injection)
D. Splenomegaly
Reveal Answer
Answer: C. Bilateral conjunctival suffusion (non-purulent injection)
Conjunctival suffusion — bilateral conjunctival injection without discharge — is a characteristic and relatively specific sign of leptospirosis, reflecting the generalised vasculitis that Leptospira causes. Tender hepatomegaly and splenomegaly can occur in both viral hepatitis and leptospirosis. Pale stools suggest cholestatic hepatitis (hepatitis A/B) rather than leptospirosis, where jaundice is haemolytic and hepatocellular. The combination of occupational waterlogged-field exposure + jaundice + conjunctival suffusion + myalgia should prompt immediate leptospirosis workup and empirical doxycycline or penicillin.