Page 2 of 35
IM26.1-7 | Infectious Disease Approach — SDL Guide (Part 2)
Diagnostic Investigations: Core Panel and Interpretation
Diagnostic investigation in infectious disease is most efficient when the core panel is ordered with specific interpretive questions in mind, and each result is read not in isolation but as a component of the evolving clinical picture. The goal is not to order every available test but to build a diagnostic picture systematically — starting with widely available, inexpensive investigations that rapidly stratify the severity and likely aetiology, then proceeding to more specific confirmatory tests guided by the clinical hypothesis. The core diagnostic panel encompasses haematological, biochemical, microbiological, and radiological investigations. Understanding the specific diagnostic yield and clinical interpretation of each test transforms a panel from a checklist into a reasoning tool. For example, a leucopenia in a febrile patient is as informative as leucocytosis — it immediately shifts the differential toward viral infections, intracellular bacteria, or overwhelming sepsis. Similarly, a platelet count of 40,000/µL in a febrile patient who returned from endemic areas is highly specific for dengue or malaria, even before serology or smear results are available. The physician who reads each result with a pre-formed question in mind extracts far more diagnostic value than one who waits passively for the laboratory report.
Complete blood count (CBC) with differential is the most information-rich single test in infectious disease. Key patterns:
- Leucocytosis with neutrophilia (WBC >11,000/µL, neutrophils >75%): bacterial infection, particularly pyogenic infections (pneumococcal pneumonia, pyelonephritis, abscess). Total WBC can reach 30,000–50,000 in severe sepsis.
- Leucopenia (WBC <4,000/µL): viral infections (dengue, typhoid early phase, HIV), rickettsial disease (scrub typhus), overwhelming bacterial sepsis (a poor prognostic sign).
- Left shift (band forms >10%): indicates the marrow is releasing immature neutrophils under demand pressure — a reliable sign of active bacterial infection or severe sepsis.
- Atypical lymphocytes (>10%): EBV infectious mononucleosis, CMV, viral hepatitis, dengue.
- Eosinophilia (>500/µL): helminth infections (during tissue migration phase — ascaris, hookworm, strongyloides) and drug reactions; notably ABSENT in most protozoan infections.
- Thrombocytopenia (platelets <150,000/µL): dengue (characteristic — monitor for critical-phase drop to <20,000), malaria, leptospirosis, rickettsial disease, severe sepsis, HUS.
Peripheral blood smear is indispensable for the diagnosis of malaria (thick smear for sensitivity, thin smear for species identification and parasite density), and also reveals platelet clumping in thrombocytopenia, rouleaux formation in myeloma, and sickle cells.
Blood biochemistry: Liver function tests — elevated transaminases in hepatitis, leptospirosis, dengue, and any sepsis-induced liver dysfunction; elevated bilirubin and LDH with low haptoglobin in haemolytic malaria; elevated creatinine in septic AKI, leptospirosis, or HUS. C-reactive protein (CRP) and procalcitonin (PCT) — PCT is a useful biomarker to distinguish bacterial infection (elevated) from viral infection (usually normal/mildly elevated). Creatine kinase — elevated in rhabdomyolysis from viral myositis or severe leptospirosis.
Blood cultures: Two sets (aerobic + anaerobic) from separate venepuncture sites before starting antibiotics — ideally when the patient is spiking fever. Modern automated culture systems (BACTEC, BacT/Alert) flag positivity within 12–48 hours for most organisms. Blood culture yield in typhoid is 60–80% in the first week. In suspected endocarditis, three sets over 24 hours increase sensitivity to >95%.
Urinalysis with microscopy: Pyuria (>10 WBC/HPF) + bacteriuria + nitrite positive = UTI. Haematuria + proteinuria in leptospirosis (renal tubular injury). Dipstick leucocyte esterase is a rapid screening tool but culture confirmation is needed.
Urine culture: Midstream clean-catch specimen; colony count ≥100,000 CFU/mL of a single organism = significant bacteriuria. Sensitivity falls with prior antibiotic use.
Chest X-ray (CXR): Lobar consolidation = pneumococcal pneumonia; bilateral interstitial infiltrates = atypical pneumonia (Mycoplasma, Chlamydia, viral), PCP in HIV; pleural effusion = empyema, TB; hilar lymphadenopathy + upper-lobe infiltrate = TB; perihilar butterfly shadow + pleural effusions = cardiac pulmonary oedema (important non-infectious differential).
Sputum Gram stain and culture: Performed on deep-cough expectorated specimen (not saliva — >25 squamous cells/LPF = reject). Gram stain provides immediate pathogen characterisation: Gram-positive diplococci in pairs = Streptococcus pneumoniae; Gram-negative rods = Klebsiella, Pseudomonas, Haemophilus influenzae. Culture with sensitivity guides definitive antibiotic choice.
Sputum AFB smear and culture: Ziehl-Neelsen stain for acid-fast bacilli — 3 consecutive early-morning specimens. Three negative smears have ~50–70% sensitivity for pulmonary TB; culture on LJ medium (8 weeks) or MGIT liquid culture (2–3 weeks) is gold standard. GeneXpert MTB/RIF (cartridge-based PCR) detects TB DNA and rifampicin resistance simultaneously in 2 hours — recommended as the initial diagnostic test in India under NTEP for symptomatic patients.
CSF analysis: Lumbar puncture for suspected meningitis or encephalitis after excluding raised intracranial pressure (fundoscopy + CT head if papilloedema or focal neurology). The CSF profile distinguishes the causative agent with high specificity (see SDL: CNS and Clostridial Infections for full CSF table).
Stool examination: Microscopy for ova, cysts, and parasites (amoeba, Giardia, helminth ova, Cryptosporidium in immunocompromised). Stool culture for Salmonella, Shigella, E. coli O157. ELISA for Giardia and Cryptosporidium antigen.
Pleural and body fluid analysis: Any effusion in the context of infection warrants diagnostic aspiration. Light's criteria distinguish exudate from transudate; elevated fluid LDH, low pH (<7.2), and positive culture confirm empyema.
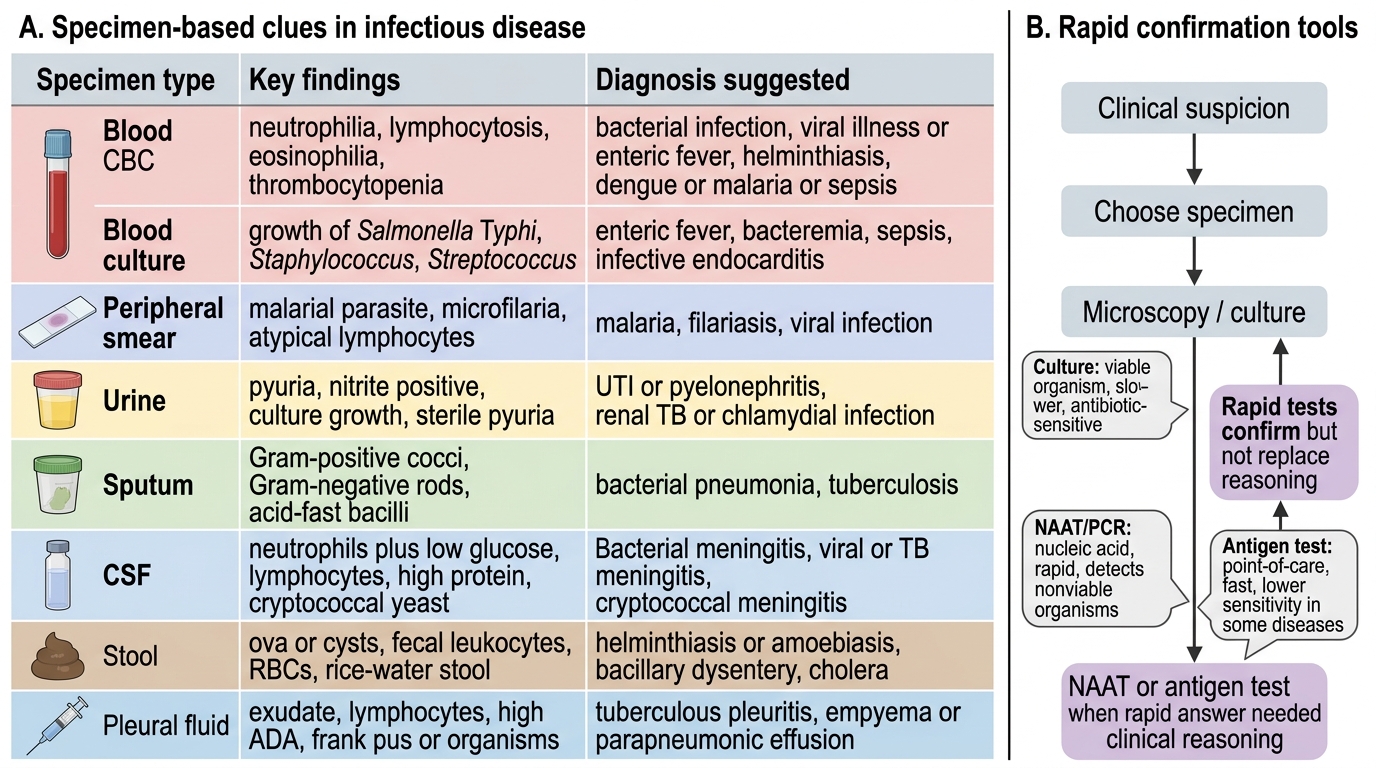
Specimen-Based Diagnostic Clues in Infectious Disease
Newer Diagnostic Techniques in Infectious Disease
The last two decades have produced a generation of molecular and point-of-care diagnostic tools that have transformed the speed and precision of infectious disease diagnosis. The final-year physician must know the indications, strengths, and limitations of these technologies — not simply their names — because they directly inform clinical decision-making and resource allocation in settings as varied as a district hospital in rural India and a tertiary referral centre. Traditional microbiological culture — the gold standard for pathogen identification — has inherent limitations: it requires a viable organism, takes 24–72 hours for bacteria (and weeks for mycobacteria), and is rendered falsely negative by prior antibiotic exposure, which is extremely common in the Indian healthcare context where self-medication with antibiotics is widespread. Newer molecular and immunological tools address these gaps by detecting pathogen-specific nucleic acid or antigens rather than viable organisms, and by returning results within hours rather than days. The key principle in selecting these tests is that they are not replacements for clinical reasoning — they confirm a hypothesis already formed from history and examination. Ordering a metagenomics panel without a prior clinical framework wastes resources and may generate uninterpretable results; ordering a targeted HSV PCR on CSF in a patient with temporal lobe changes on MRI and encephalitis is precise, actionable, and potentially life-saving.
Polymerase chain reaction (PCR) and its variants amplify specific nucleic acid sequences from a clinical specimen, allowing detection of organisms present in quantities too small to culture or visualise. Key applications and their indications:
- GeneXpert MTB/RIF: first-line TB diagnosis in India under NTEP; detects M. tuberculosis DNA and resistance to rifampicin (a rifampicin-resistance signal is a surrogate for MDR-TB) in approximately 2 hours from sputum; sensitivity ~88% (superior to smear microscopy at ~65%).
- HSV PCR on CSF: far superior to culture for herpes simplex encephalitis; sensitivity >95%; if HSV encephalitis is clinically suspected, aciclovir should not be withheld pending the result.
- Dengue NS1 PCR/antigen: detectable in the first 5 days when serology may be negative; NS1 antigen ELISA is the standard point-of-care tool.
- Multiplex respiratory PCR panels: simultaneous detection of influenza A/B, RSV, SARS-CoV-2, and other respiratory viruses from nasopharyngeal swabs — dramatically reduces unnecessary antibiotic use.
- 16S rRNA universal PCR: amplifies conserved bacterial ribosomal gene from any specimen; used in culture-negative endocarditis or CNS infections with prior antibiotic exposure.
Antigen detection tests are rapid immunoassay tools that detect pathogen proteins directly without culture or nucleic acid amplification:
- Urine Legionella antigen: detects serogroup 1 (responsible for 80% of Legionella pneumonia); result in 15 minutes; indicated in severe atypical pneumonia.
- Cryptococcal antigen (CrAg) in CSF and serum: latex agglutination or lateral flow assay; sensitivity >98% for cryptococcal meningitis; point-of-care test available in resource-limited settings.
- Rapid malaria antigen tests (RDTs): Histidine-rich protein-2 (HRP2) for P. falciparum; pan-specific aldolase for all Plasmodium species; sensitivity ~96% for falciparum, lower for non-falciparum; microscopy should still be performed for species confirmation and parasite density when RDT positive.
Serological tests (antibody detection):
- Widal test for enteric fever: IgM/IgG antibodies to Salmonella typhi O and H antigens; rising titres (≥4-fold between acute and convalescent samples) are meaningful but a single titre is unreliable in endemic areas due to background seropositivity.
- Weil-Felix test: agglutination of Proteus species as a surrogate for rickettsial antibodies — insensitive and non-specific; largely replaced by indirect immunofluorescence for Orientia and Rickettsia species.
- IgM ELISA for leptospirosis (LEPTO IgM ELISA): positive from day 5 of illness; Microscopic Agglutination Test (MAT) is gold standard but requires reference laboratory.
- HIV 4th-generation combo Ag/Ab ELISA: detects both HIV antibodies AND p24 antigen — shortens the window period to ~18 days.
Imaging in infectious disease: Ultrasound (rapid, bedside, no radiation — amoebic liver abscess, splenic abscess, endocarditis vegetation screening, pleural effusion characterisation); CT chest (PCP interstitial disease, invasive pulmonary aspergillosis — characteristic halo sign and air-crescent sign in neutropenic patients, tree-in-bud pattern in endobronchial TB spread); CT abdomen (retroperitoneal collections, psoas abscess); MRI brain (herpes encephalitis — temporal lobe hyperintensity on FLAIR; tuberculoma; toxoplasma — ring-enhancing lesions).
Next-generation sequencing (metagenomic NGS): High-throughput sequencing of all nucleic acid in a clinical specimen, capable of identifying any pathogen — including novel organisms — without prior diagnostic hypothesis. Currently used in reference laboratories for culture-negative encephalitis, culture-negative endocarditis, and undiagnosed febrile illness. Not yet standard care but increasingly available in tertiary centres.
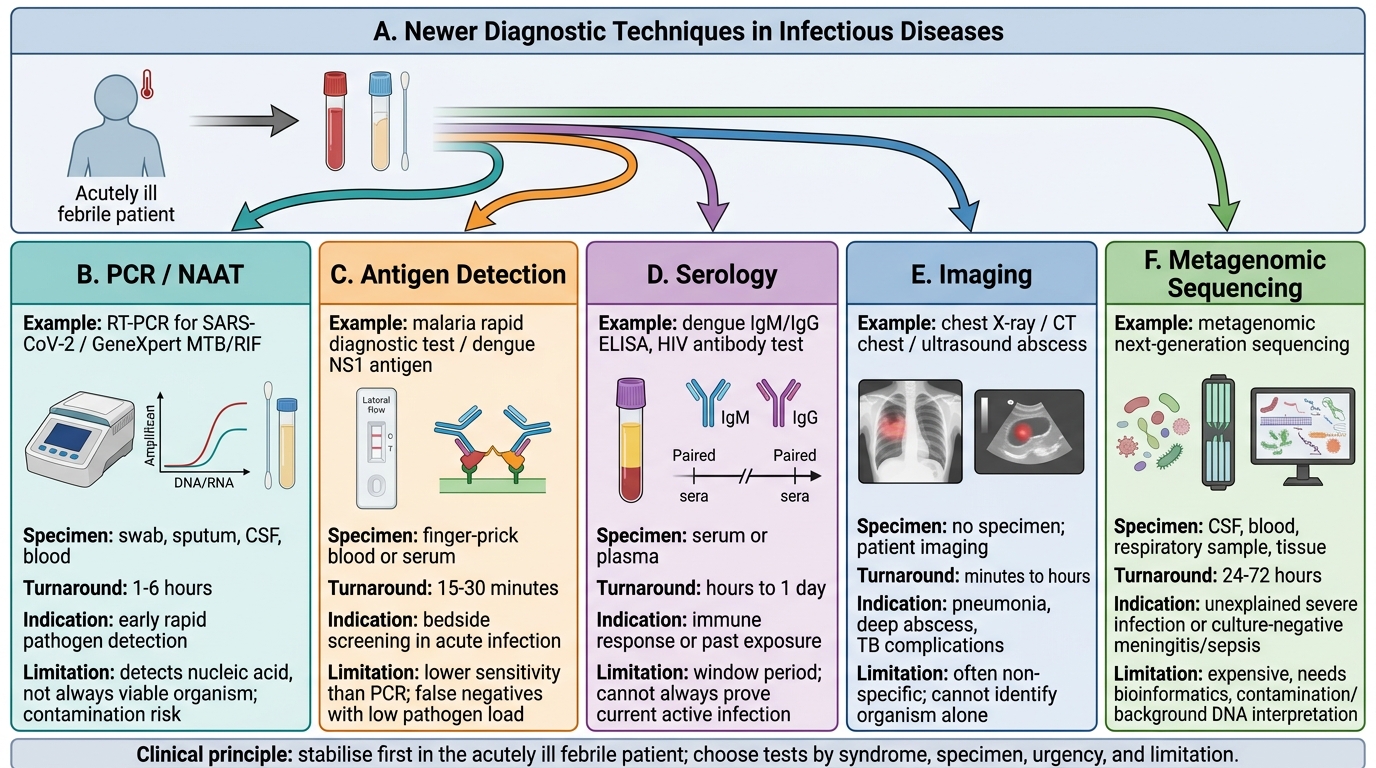
Newer Diagnostic Techniques in Infectious Diseases
Approach to the Acutely Ill Febrile Patient
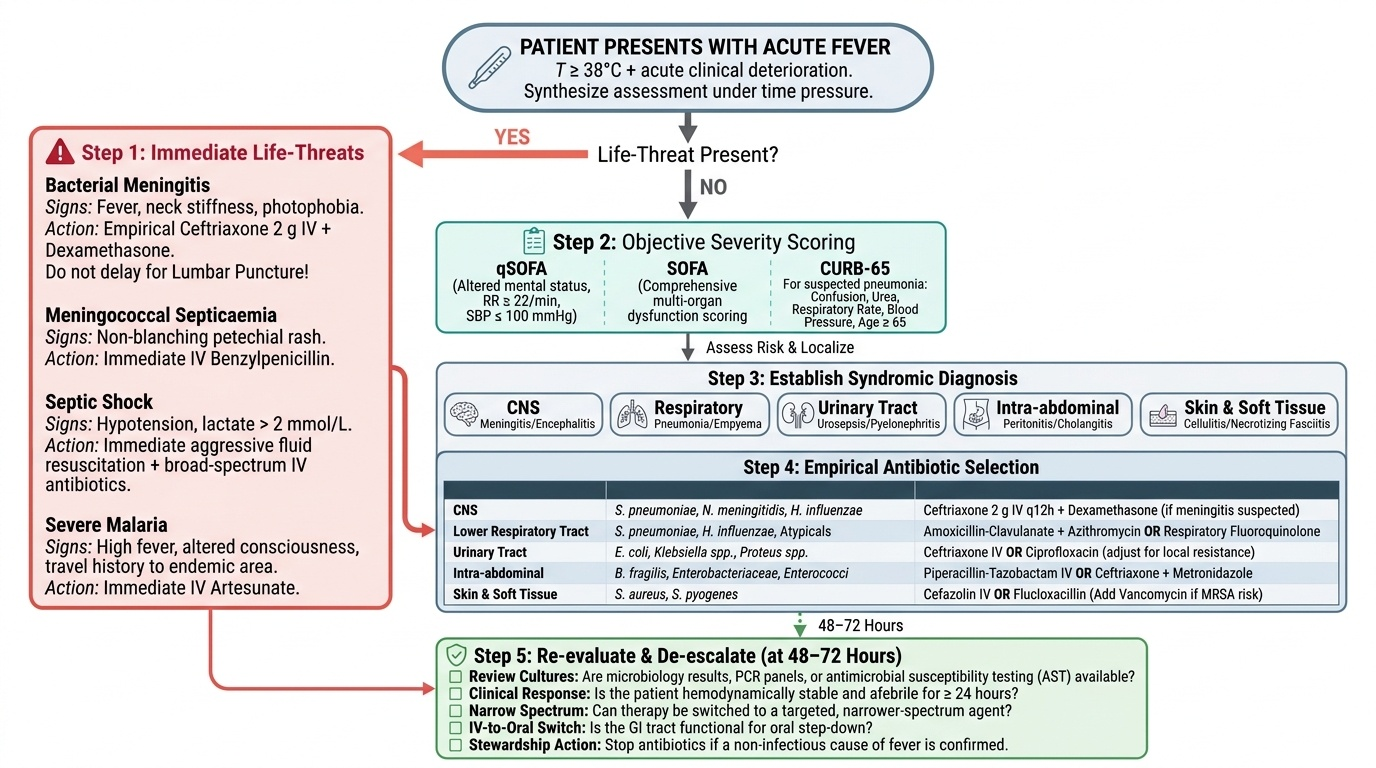
The acutely ill febrile patient demands a synthesis of rapid clinical assessment and structured decision-making that happens simultaneously, not sequentially. The first clinical question is not 'what organism?' but 'how sick is this patient, and do they need immediate intervention before I know the diagnosis?' This priority — stabilise first, investigate second — is what distinguishes emergency management from elective workup. Recognising when a febrile presentation is life-threatening requires both pattern recognition and knowledge of the time-sensitive syndromes that kill if treatment is delayed even by one or two hours. The physician who orders a full diagnostic panel before starting antibiotics in a patient with septic shock has allowed the window of opportunity to narrow; conversely, the physician who starts broad-spectrum antibiotics for every febrile patient without considering the clinical probability of serious bacterial infection contributes directly to the antimicrobial resistance crisis. Managing the acutely ill febrile patient is therefore the integration of all the preceding content in this module — pathogenesis, history, examination, investigations, and antibiotic principles — applied under time pressure with incomplete information. The structured five-step approach below provides an operational framework for this integration in clinical practice.
Provided image
Step 1 — Identify the immediately life-threatening presentations. Certain fever presentations require immediate action without waiting for any investigation result:
- Bacterial meningitis: fever + neck stiffness + photophobia → begin empirical ceftriaxone 2g IV and dexamethasone before lumbar puncture if any delay in LP; minutes matter in bacterial meningitis
- Meningococcal septicaemia: non-blanching petechial rash spreading rapidly → IV benzylpenicillin or ceftriaxone immediately (even before hospital transfer if in the community)
- Septic shock (fever + hypotension + altered consciousness + tachycardia): begin the Surviving Sepsis Campaign 1-hour bundle — blood cultures ×2, IV broad-spectrum antibiotics (do NOT wait for cultures), IV fluid resuscitation (30 mL/kg crystalloid over 1 hour), vasopressors if hypotension persists, lactate measurement
- Falciparum malaria with severe features: IV artesunate immediately (do not await full species confirmation if thick smear shows any Plasmodium in a patient with altered consciousness or haemoglobin <7 g/dL)
- Rabies after category III exposure: RIG to wound + start vaccine series immediately
Step 2 — Assess severity and allocate resources. Validated scoring tools allow objective severity assessment and guide the level of care:
- qSOFA score (Quick SOFA): respiratory rate ≥22/min (1 point), altered mentation (1 point), systolic BP ≤100 mmHg (1 point). Score ≥2 in a patient with suspected infection identifies high risk of organ dysfunction (sepsis criteria) — triggers ICU evaluation.
- SOFA score: full sequential organ failure assessment used in ICU to define sepsis (increase ≥2 points from baseline) and septic shock (vasopressor need + lactate >2 mmol/L despite adequate resuscitation).
- CURB-65 for community-acquired pneumonia: confusion, urea >7 mmol/L, RR ≥30/min, BP <90/60 mmHg, age ≥65. Score 0–1 = outpatient; score 2 = consider hospitalisation; score ≥3 = ICU review.
Step 3 — Determine the syndromic diagnosis. Even without definitive microbiological identification, a syndromic diagnosis (pneumonia, UTI, meningitis, febrile neutropenia, enteric fever, dengue fever, malaria) allows empirical antibiotic selection and avoids both under-treatment and inappropriate broad-spectrum overuse.
Step 4 — Select empirical antibiotic therapy rationally. Empirical therapy is the antibiotic started before microbiological confirmation, based on:
(a) The most likely organism for the syndrome and host (e.g., Pneumococcus + atypical organisms in community-acquired pneumonia; enteric Gram-negative rods in pyelonephritis; Staphylococcus or Streptococcus in necrotising fasciitis)
(b) Local antibiogram patterns (critical in settings with high ESBL-producing Enterobacteriaceae prevalence)
(c) Patient factors — prior antibiotic exposure, healthcare-associated risk factors (MR Staphylococcus aureus, MDR Gram-negatives)
(d) Severity of illness — mild community-acquired infection can begin with oral narrow-spectrum agents; life-threatening infections begin with IV broad-spectrum coverage and are de-escalated when culture results return.
Step 5 — De-escalation and antimicrobial stewardship. The principle of antimicrobial stewardship is: use the right antibiotic, at the right dose, for the right duration, and stop it as soon as it is no longer needed. Unnecessary broad-spectrum antibiotic use drives antimicrobial resistance (AMR), which is now one of the ten leading global health threats. Practical stewardship principles: (a) review blood culture results within 48–72 hours and narrow the regimen (de-escalate from broad-spectrum to targeted therapy); (b) switch from IV to oral at 48–72 hours when the patient is improving and can swallow; (c) 5–7 days is sufficient for most community-acquired bacterial infections; (d) never use antibiotics for confirmed viral infections (influenza, dengue, viral hepatitis) except to treat superimposed bacterial complications.
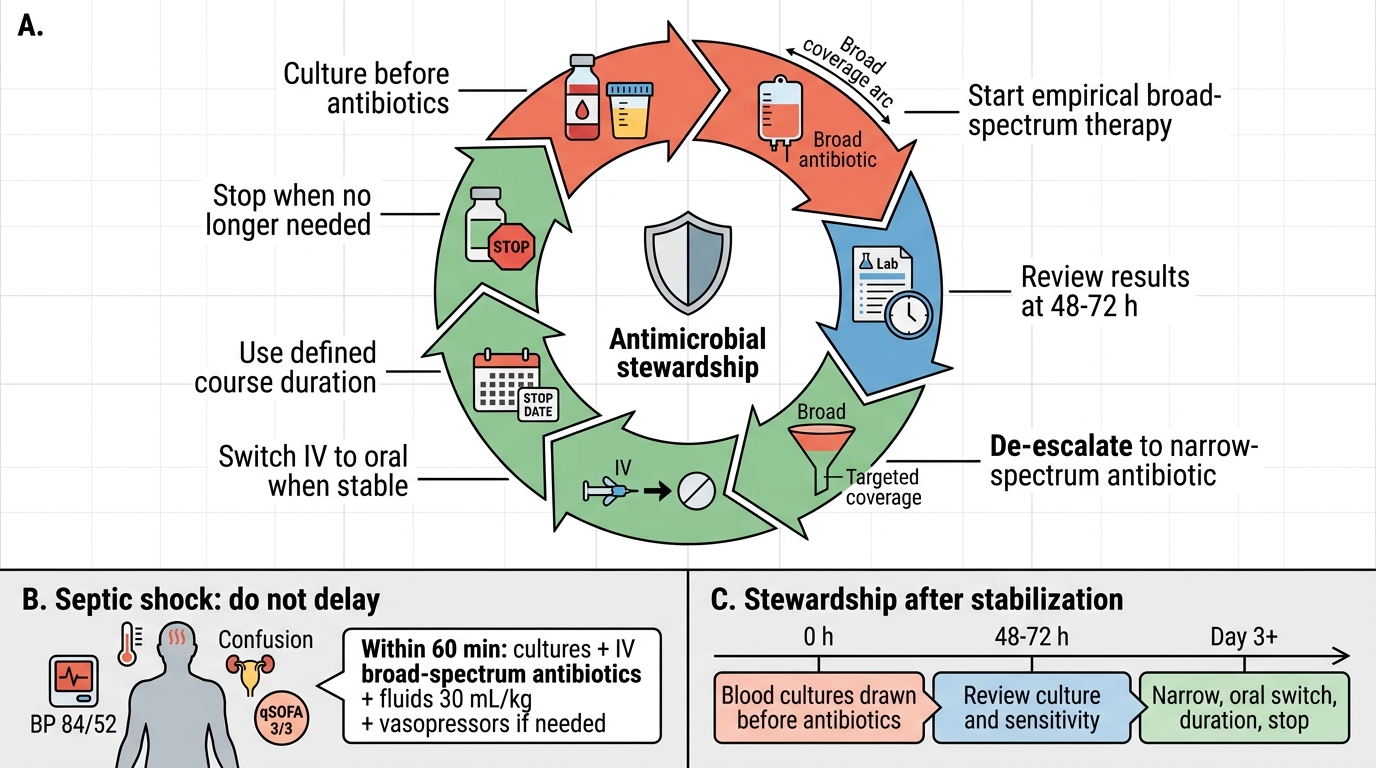
Antimicrobial Stewardship Cycle
SELF-CHECK
A 55-year-old diabetic man is brought to the emergency department with 2 days of fever (39.5°C), confusion, hypotension (BP 84/52 mmHg), and urinary symptoms. His qSOFA score is 3/3. Blood cultures are drawn. Which action is MOST critical in the next 60 minutes?
A. Await blood culture results before starting antibiotics to ensure appropriate antibiotic selection
B. Start intravenous broad-spectrum antibiotics, IV fluid resuscitation 30 mL/kg, and vasopressors if hypotension persists after fluids
C. Perform lumbar puncture immediately to exclude meningitis
D. Order CT abdomen to locate the source of infection before antibiotics
Reveal Answer
Answer: B. Start intravenous broad-spectrum antibiotics, IV fluid resuscitation 30 mL/kg, and vasopressors if hypotension persists after fluids
This patient has septic shock — the Surviving Sepsis Campaign 1-hour bundle mandates blood cultures AND immediate IV broad-spectrum antibiotics, fluid resuscitation, and vasopressors (if refractory hypotension) within 60 minutes. Awaiting culture results before antibiotics in septic shock has been shown to increase mortality by ~7% per hour of delay. The source is likely the urinary tract (urinary symptoms + diabetes), but this does not change the immediate priority. LP is not indicated here (no meningism). CT may be needed later but must not delay antibiotics in a shocked patient.