Page 3 of 35
IM26.1-7 | Infectious Disease Approach — SDL Guide (Part 3)
Antimicrobial Resistance: Understanding and Stewardship
Antimicrobial resistance (AMR) is the ability of a microorganism to survive and replicate in the presence of a drug that was previously able to kill or inhibit it. AMR has been declared one of the top ten global public health threats by the WHO, and India bears a disproportionate burden due to high antibiotic use density, over-the-counter availability without prescription, and inadequate infection control infrastructure. Every prescription decision made by a physician either contributes to or counters AMR, making this a core competency of clinical practice — not merely a public health abstraction. India is at the epicentre of the AMR crisis: the New Delhi Metallo-beta-lactamase (NDM-1) carbapenemase enzyme was first identified in India and has now spread globally; ESBL-producing Enterobacteriaceae are endemic in both hospital and community settings; and carbapenem-resistant organisms that leave clinicians with almost no treatment options are increasingly encountered in intensive care units across the country. Understanding resistance at the molecular level is not an academic exercise — it directly predicts which antibiotics will fail and which will succeed in a given clinical situation, and it underpins rational empirical antibiotic selection in the high-resistance environment of Indian healthcare. The key insight is that resistance mechanisms are specific: each mechanism confers resistance to particular antibiotic classes while leaving others intact, which means that knowing the mechanism allows you to predict the susceptibility pattern even before culture results return.
Mechanisms of antimicrobial resistance operate at the molecular level and must be understood to predict resistance patterns:
- Beta-lactamase production: the most common resistance mechanism in Gram-negative bacteria. Extended-spectrum beta-lactamases (ESBLs) — produced by E. coli and Klebsiella pneumoniae — hydrolyse most penicillins and cephalosporins, making these drugs ineffective. ESBL-producing organisms require carbapenem therapy. Carbapenemase-producing organisms (KPC, OXA-48, NDM-1 — New Delhi Metallo-beta-lactamase — originally isolated from India) are resistant to virtually all beta-lactams and require combination therapy with polymyxins and tigecycline.
- Modified target sites: methicillin-resistant Staphylococcus aureus (MRSA) produces an altered penicillin-binding protein (PBP2a encoded by the mecA gene) with low affinity for all beta-lactams. Vancomycin or linezolid is the treatment of choice.
- Efflux pumps: membrane proteins that actively pump antibiotic out of the bacterial cell; important in Pseudomonas aeruginosa and quinolone resistance in S. aureus.
- Altered uptake: changes in porin proteins reduce drug entry into Gram-negative cells — important in carbapenem resistance in Pseudomonas.
- Enzyme modification of drug: aminoglycoside-modifying enzymes (acetyltransferases, phosphotransferases) inactivate gentamicin and amikacin.
Key resistant organisms in India:
- ESBL-producing E. coli and Klebsiella — extremely prevalent in community and hospital settings; empirical carbapenem for sepsis when ESBL is suspected (prior UTI history, prior antibiotics, healthcare exposure)
- MRSA — prevalent in hospital settings (HA-MRSA); vancomycin for confirmed MRSA infections; teicoplanin as alternative in India
- Carbapenem-resistant Enterobacteriaceae (CRE/CPE) — rising incidence, very limited treatment options
- Drug-resistant M. tuberculosis — MDR-TB (resistance to isoniazid + rifampicin), XDR-TB (additional fluoroquinolone + injectable resistance); increasing incidence in India; all new TB cases should receive GeneXpert to screen for rifampicin resistance at diagnosis
Principles of antimicrobial stewardship in clinical practice:
1. Culture before antibiotics — always attempt cultures before starting antibiotics, especially in serious infections; this is the single most impactful stewardship action
2. Prescribe only when needed — bacterial infection must be likely before antibiotics are prescribed; viral upper respiratory infections, dengue, and uncomplicated influenza do not require antibiotics
3. Use the narrowest effective spectrum — if the organism and its sensitivities are known, de-escalate to the narrowest effective drug; reserve carbapenems and vancomycin for confirmed resistant organisms
4. Use the correct dose and duration — underdosing selects resistant mutants; excessive duration increases side-effects and resistance selection pressure; 5–7 days is adequate for most community-acquired bacterial infections
5. IV-to-oral switch — most patients with bacterial infection who are improving can switch from IV to oral antibiotics at 48–72 hours; this reduces line-related complications, enables earlier discharge, and reduces costs
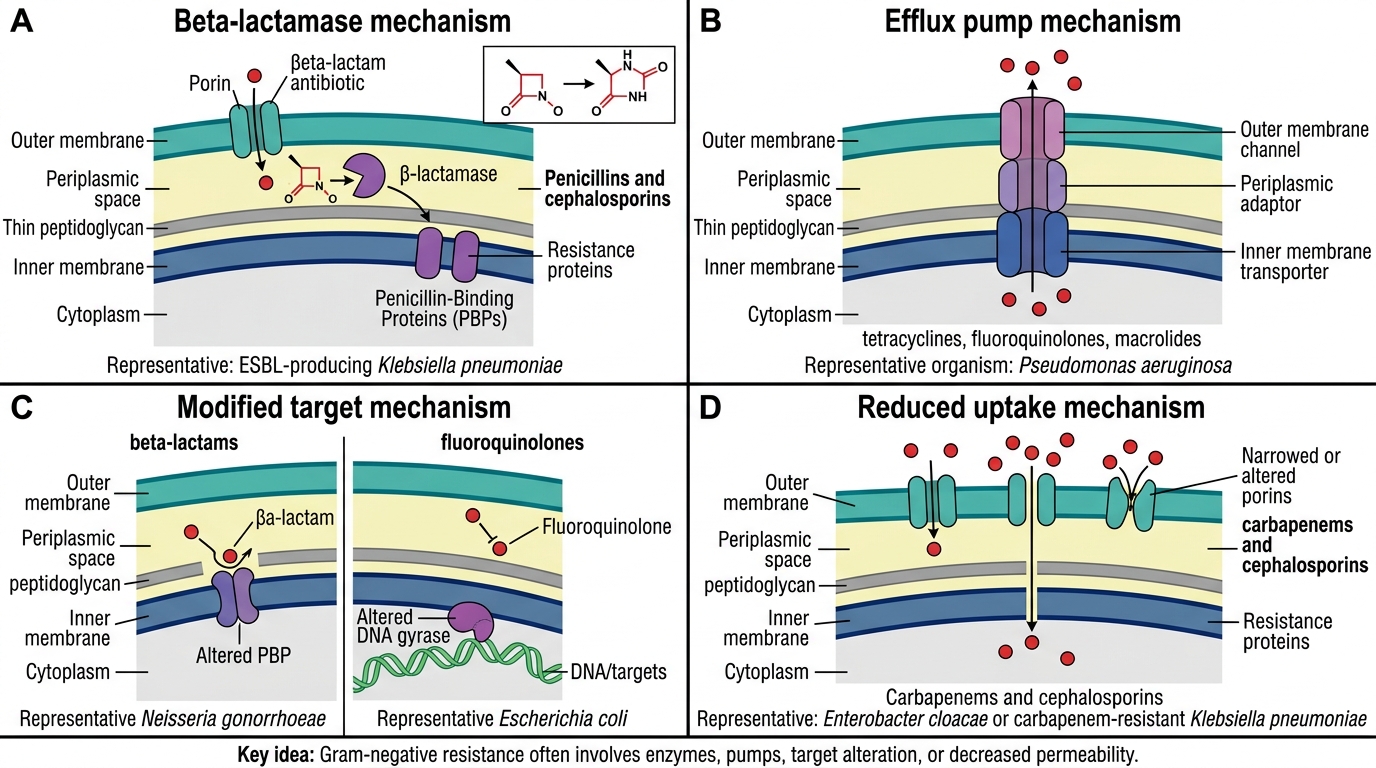
Gram-Negative Antimicrobial Resistance Mechanisms
SELF-CHECK
A 65-year-old woman is hospitalised for severe pneumonia. Sputum culture grows Klebsiella pneumoniae producing ESBL. She is currently receiving IV ceftriaxone empirically. The MOST appropriate next step is:
A. Continue ceftriaxone at a higher dose, as it is effective against ESBL producers at higher concentrations
B. Switch to IV meropenem, as ESBL-producing organisms are resistant to all cephalosporins and penicillins
C. Add IV metronidazole to the ceftriaxone for improved Gram-negative coverage
D. Switch to IV vancomycin, as ESBL producers require glycopeptide therapy
Reveal Answer
Answer: B. Switch to IV meropenem, as ESBL-producing organisms are resistant to all cephalosporins and penicillins
ESBL-producing Gram-negative organisms are resistant to all cephalosporins (including ceftriaxone) and penicillins — higher doses do not overcome this. Carbapenems (meropenem, imipenem, ertapenem) remain the drugs of choice for serious infections with ESBL producers. Metronidazole covers anaerobes and is not useful against Gram-negative aerobes. Vancomycin is effective only against Gram-positive organisms (MRSA) and has no activity against Gram-negative bacteria.
Self-Assessment: Integrating the Infectious Disease Framework
At this point in the module you have built the four pillars of the infectious disease framework: molecular pathogenesis, infection-focused history and examination, diagnostic investigation, and antimicrobial management principles including stewardship. The clinical vignettes below challenge you to apply all four pillars simultaneously, as you will need to do in the wards and in examinations. Work through each case before reading the analysis.
Provided image
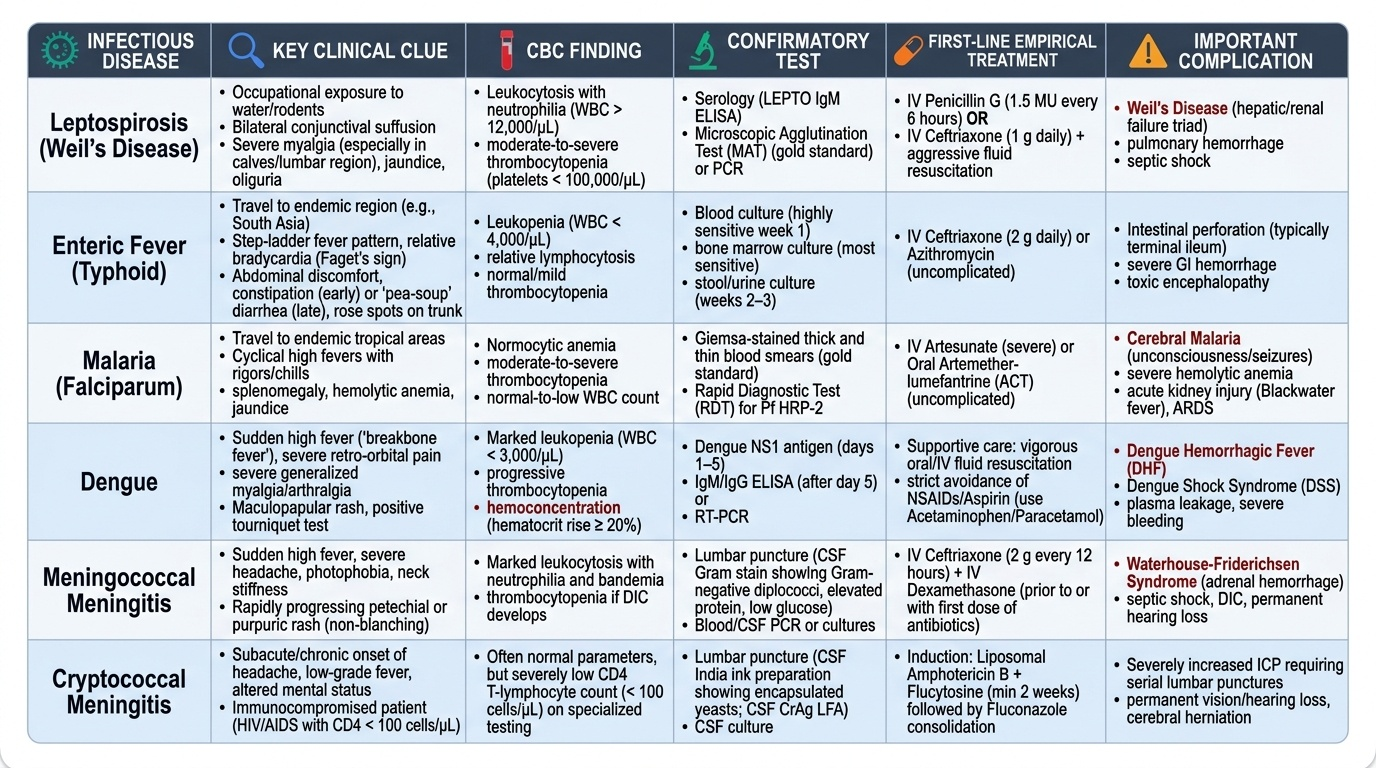
Vignette 1: A 32-year-old rice-field worker from Kerala presents in September with 5 days of fever, severe myalgia, headache, jaundice, and oliguria. HR 110/min, BP 90/60 mmHg. He has bilateral conjunctival suffusion and tender hepatomegaly. Urine dipstick: 3+ proteinuria, haematuria. CBC: WBC 14,000/µL with neutrophilia, Hb 9.8 g/dL, platelets 62,000/µL. Creatinine 4.1 mg/dL. What is the most likely diagnosis? What is the immediate investigation priority? What is the empirical treatment?
Analysis: Occupational waterlogged exposure + conjunctival suffusion + jaundice + renal failure + thrombocytopenia = leptospirosis (Weil's disease — the severe form). Immediate investigations: blood culture, LEPTO IgM ELISA, urine culture, LFTs, coagulation screen, ABG. He is in septic shock — begin the 1-hour sepsis bundle. Empirical treatment: IV penicillin G 1.5 MU 6-hourly (or IV ceftriaxone 1g daily as an alternative) + ICU-level fluid and electrolyte management for AKI.
Vignette 2: A 19-year-old student from Bihar presents with 10 days of progressively worsening fever (initially 37.5–38°C, now 39.8°C), headache, abdominal discomfort, and constipation. HR 86/min (relative bradycardia for a fever of 39.8°C). He has faint rose spots on the abdomen and mild splenomegaly. WBC 3,800/µL (leucopenia), platelets 120,000/µL. ALT slightly elevated. What is the working diagnosis? What is the first investigation to confirm? What treatment should be started?
Analysis: Stepwise fever over 10 days + relative bradycardia + rose spots + splenomegaly + leucopenia = enteric fever (typhoid fever; Salmonella typhi). First investigation: blood culture (sensitivity 60–80% in the first week — the single most important diagnostic test). Widal test is unreliable as a single titre in endemic areas. Start IV ceftriaxone 2g once daily (first-line in India given high nalidixic acid resistance and intermediate ciprofloxacin sensitivity; azithromycin oral is an alternative for uncomplicated enteric fever).
Vignette 3: A 45-year-old man known to be HIV-positive (CD4 count 42 cells/µL, not on ART) presents with 3 weeks of progressive headache and one episode of vomiting. He has mild photophobia but no neck stiffness on examination. CT head shows no mass lesion or raised ICP. India ink preparation of CSF: encapsulated yeasts present. CrAg positive. What is the diagnosis? What is the induction treatment?
Analysis: HIV + CD4 <100 cells/µL + chronic headache + India ink encapsulated yeasts = cryptococcal meningitis. Induction treatment (2 weeks): IV amphotericin B (0.7–1.0 mg/kg/day, liposomal formulation preferred) + oral flucytosine (25 mg/kg four times daily). Consolidation (8 weeks): oral fluconazole 400 mg/day. Maintenance (lifelong until CD4 >200): oral fluconazole 200 mg/day. Commence ART after 5 weeks of antifungal treatment (not immediately — immune reconstitution inflammatory syndrome — IRIS — risk).
CLINICAL PEARL
The three most dangerous errors in managing the febrile patient are: (1) starting antibiotics for a viral illness (denies benefit, drives resistance, may delay the correct diagnosis); (2) delaying antibiotics for a bacterial emergency (meningococcaemia, septic shock, suspected bacterial meningitis — each hour of delay worsens outcomes measurably); (3) treating 'the organism' rather than 'the patient' — a blood culture positive for Candida in a patient who is systemically well with a peripheral IV line may represent line contamination, while the same result in an ICU patient on TPN with a Hickman catheter demands immediate antifungal therapy and line removal. The scaffold of clinical context — the patient's immunological state, the site of infection, the severity of illness, and the plausibility of the organism as a true pathogen — determines whether a positive culture demands treatment.