Page 18 of 35
IM26.21-25 | Viral Infections: Herpesviruses, Respiratory Viruses, Rabies, and Dengue — SDL Guide
Learning Objectives
- Describe the pathogenesis, clinical features, diagnosis, and management of herpesvirus infections: HSV-1, HSV-2, and varicella-zoster virus (VZV)
- Describe the pathogenesis, clinical features, and management of COVID-19, SARS, and influenza, including pandemic preparedness principles
- Describe the pathogenesis, clinical features, post-exposure prophylaxis, and management of rabies
- Describe the pathogenesis, clinical features, diagnosis, and management of dengue fever including dengue haemorrhagic fever and dengue shock syndrome
INSTRUCTIONS
This SDL covers five major viral infection groups that every Indian physician will encounter in practice: herpesviruses (latent-reactivation biology), respiratory viruses including COVID-19 and influenza (droplet transmission, pandemic behaviour), rabies (invariably fatal once symptomatic — PEP is the intervention), and dengue (the most common arboviral disease in India — fluid management is the critical skill). For each group, the key diagnostic and management decisions are highlighted. Dengue and rabies PEP categories (Category I/II/III) per WHO/NVBDCP are examinable specifics.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 187 — Herpes Simplex Virus; Ch. 188 — Varicella-Zoster Virus; Ch. 197 — Influenza; Ch. 203 — SARS-CoV-2/COVID-19; Ch. 220 — Rabies; Ch. 228 — Dengue (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (Dengue, Viral Encephalitis, COVID-19 chapters) (textbook)
- National Vector Borne Disease Control Programme (NVBDCP) Dengue Clinical Management Guidelines, 2015 (revised) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Four presentations arrive at a general medicine ward in a monsoon-season week in Pune. A 19-year-old college student with painful vesicles on the lips, fever, and cervical lymphadenopathy — he has had two similar episodes before. A 62-year-old diabetic with a unilateral blistering rash following the T5–T6 dermatome and unbearable lancinating pain — the rash appeared 3 days ago and has spread to involve the right chest wall. A 7-year-old child brought by parents who are terrified — she was bitten on the foot by an apparently healthy dog 4 days ago and they delayed seeking care. A 22-year-old software engineer with 4 days of high fever, retro-orbital headache, severe myalgia, and a diffuse macular rash that appeared this morning — platelet count is 68,000/µL. These four presentations each demand a completely different response: the student needs oral acyclovir and reassurance about latency; the diabetic needs urgent IV acyclovir and pain management to prevent postherpetic neuralgia; the child needs an immediate wound wash, anti-rabies vaccine (Category III bite — vaccination + RIG), and urgent counselling to her parents; the software engineer needs careful fluid monitoring for dengue warning signs and education about the danger of NSAIDs. This module equips you with the clinical reasoning for each response — and the knowledge that getting each one wrong has potentially irreversible consequences.
WHY THIS MATTERS
Viral infections are numerically the most common cause of acute illness encountered in Indian clinical practice. Dengue fever is now endemic in virtually every Indian state, with over 100,000 cases officially notified annually (with true burden estimated 10–100× higher); dengue haemorrhagic fever and dengue shock syndrome account for preventable deaths when fluid management errors are made. Rabies kills an estimated 20,000 Indians annually — the highest rabies mortality in the world — almost all of which is preventable with prompt and correct post-exposure prophylaxis. COVID-19 demonstrated the pandemic potential of novel coronaviruses and permanently changed Indian public health preparedness. Herpes zoster causes severe morbidity in the ageing and immunocompromised population — postherpetic neuralgia is one of the most challenging chronic pain conditions in general medicine. Influenza causes annual epidemics and periodic pandemics with significant mortality in high-risk groups. Mastering the clinical management of these viral infections is foundational to modern internal medicine practice in India.
RECALL
Recall the fundamental virology underpinning this module. Herpesviruses (HSV, VZV, CMV, EBV) share a defining biological property: latency — after primary infection, the virus establishes a lifelong latent state in sensory ganglia (HSV in trigeminal/sacral ganglia, VZV in dorsal root ganglia); reactivation occurs when cell-mediated immunity is suppressed (stress, immunosuppression, malignancy). Dengue virus is a flavivirus (RNA, positive-sense) transmitted by the Aedes aegypti and Aedes albopictus mosquitoes; four serotypes (DENV-1 to 4) — primary infection with one serotype is followed by lifelong immunity to that serotype but enhanced susceptibility to severe disease upon infection with a different serotype, due to antibody-dependent enhancement (ADE). Rabies virus is a rhabdovirus (Lyssavirus) that travels centripetally along peripheral nerves to the brain — once it reaches the central nervous system and clinical rabies develops, mortality is virtually 100%. Influenza virus undergoes antigenic drift (gradual point mutations — basis of annual epidemics) and antigenic shift (major reassortment of haemagglutinin/neuraminidase — basis of pandemics).
Herpesvirus Infections: HSV and VZV
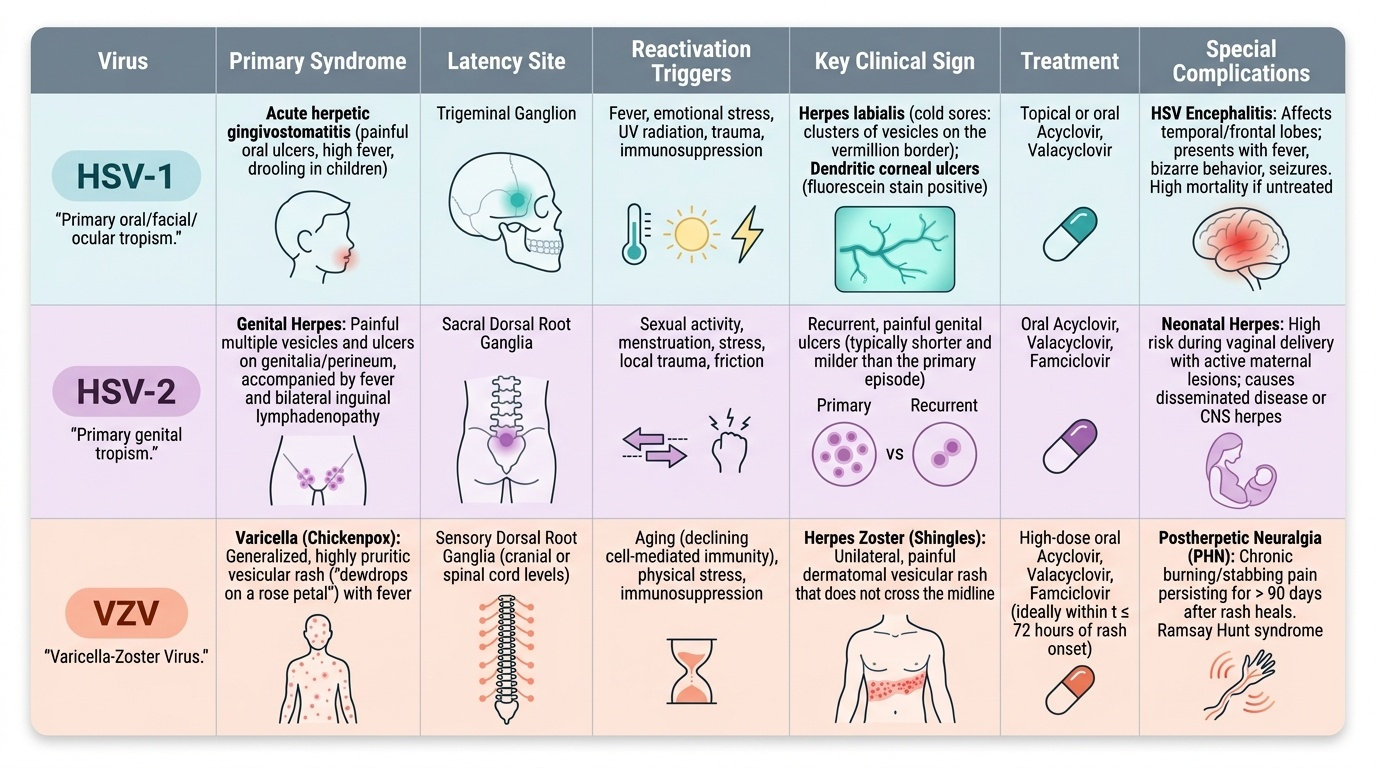
Herpes simplex virus (HSV) infections are caused by two antigenically distinct viruses — HSV-1 (primary tropism: oral, facial, corneal, encephalitis) and HSV-2 (primary tropism: genital, neonatal herpes). Both are ubiquitous: HSV-1 seroprevalence approaches 70–80% in Indian adults, with most primary infections occurring in childhood as subclinical or mild febrile illness. HSV-2 seroprevalence is lower but sexually transmitted; genital herpes is a significant STI burden. The defining biological feature of herpesviruses is latency and reactivation: after primary infection, HSV establishes latency in sensory ganglia (HSV-1 in the trigeminal ganglion; HSV-2 in the sacral dorsal root ganglia). Reactivation is triggered by fever, emotional stress, UV radiation, immunosuppression, menstruation, or trauma. This latency-reactivation cycle explains why antiviral drugs suppress but cannot eradicate HSV infections.
Provided image
Clinical syndromes of HSV:
- Primary HSV-1 (gingivostomatitis): in children — extensive painful ulcers on the gingiva, tongue, and oral mucosa; fever, drooling, cervical lymphadenopathy; lasts 1–2 weeks; self-limiting.
- Herpes labialis ('cold sore'): the classic recurrence — prodromal tingling → cluster of vesicles on the vermillion border of the lip; resolves in 7–10 days.
- Herpes keratitis (ocular HSV): HSV-1 is the most common infectious cause of corneal blindness in developing countries; dendritic ulcer on fluorescein staining is pathognomonic.
- Genital herpes (HSV-2): primary episode — multiple painful vesicles and ulcers on the genitalia, perineum; fever, bilateral inguinal lymphadenopathy; lasts 2–3 weeks. Recurrences are shorter and milder than the primary episode.
- HSV encephalitis: the most common sporadic viral encephalitis — HSV-1 in adults; predominantly affects the temporal and frontal lobes (limbic encephalitis); presents with fever, bizarre behaviour, temporal lobe seizures, and aphasia; CSF: lymphocytic pleocytosis, elevated protein, normal glucose; MRI: hyperintense signal in the temporal lobes (T2/FLAIR); diagnosis: CSF PCR for HSV DNA (sensitivity >95%); treat with IV acyclovir 10 mg/kg 8-hourly × 14–21 days — outcome depends on speed of initiation.
- Neonatal herpes (HSV-2): acquired during delivery from a mother with active genital HSV; disseminated disease or CNS herpes in the neonate; very high mortality and neurological sequelae; treated with IV acyclovir 20 mg/kg 8-hourly × 21 days.
Treatment: acyclovir is the antiviral of choice for all HSV infections. Mechanism: acyclovir is phosphorylated by HSV thymidine kinase (preferentially in infected cells) → triphosphate inhibits viral DNA polymerase; highly selective for infected cells. Dosing: oral acyclovir 400 mg 5×/day × 7–10 days for primary genital herpes; oral acyclovir 200 mg 5×/day × 5 days for herpes labialis recurrence; IV acyclovir 10 mg/kg 8-hourly for HSV encephalitis, severe primary HSV, immunocompromised patients. Valacyclovir (oral prodrug, better bioavailability) is preferred over oral acyclovir in clinical practice for most adults. Suppressive therapy: valacyclovir 500 mg daily reduces recurrence frequency in patients with frequent recurrences (≥6/year).
Varicella-Zoster Virus (VZV) causes two distinct clinical syndromes: varicella (chickenpox) — primary infection; and herpes zoster (shingles) — reactivation from latency in dorsal root ganglia.
Varicella (chickenpox): predominantly a childhood illness in India, though with increasing adult susceptibility in urban populations. Transmitted by respiratory droplets and direct contact with vesicle fluid — highly contagious (secondary attack rate ~90% in susceptible household contacts). Incubation: 10–21 days. Clinical features: low-grade fever → pruritic rash starting on the trunk → face → extremities; key characteristic: polymorphic eruption — multiple stages of lesions coexist at the same time (macules, papules, vesicles, and crusts are all visible simultaneously, unlike other exanthems which progress in a uniform wave). Lesions are intensely pruritic. Complications: secondary bacterial infection (impetigo), varicella pneumonia (adults — severity is disproportionately higher in adults than children; VZV pneumonia in an adult can be life-threatening), encephalitis (cerebellar ataxia most common — good prognosis), Reye's syndrome if aspirin is used.
Herpes zoster (shingles): reactivation of VZV from dorsal root ganglia, typically in older or immunocompromised patients. The reactivated virus travels along the sensory nerve to produce a dermatomal eruption. Clinical features: prodromal pain and hyperaesthesia in a dermatomal distribution (1–4 days before rash) → vesicular eruption confined to a single dermatome — the pathognomonic unilateral dermatomal distribution distinguishes zoster from other vesicular rashes. The thoracic dermatomes (T3–T12) are most commonly affected. Herpes zoster ophthalmicus (HZO) — V1 (ophthalmic) branch of trigeminal nerve involvement; Hutchinson's sign (vesicles on the tip of the nose = nasociliary nerve involvement) predicts ocular complications; urgent ophthalmology referral. Ramsay Hunt syndrome — VZV reactivation in the geniculate ganglion of the facial nerve; vesicles in the external auditory canal, ipsilateral facial palsy, and tinnitus/vertigo. Postherpetic neuralgia (PHN) — pain persisting >90 days after rash healing; occurs in ~10–15% of all zoster patients, rising to ~50% in those >70 years; one of the most refractory chronic pain conditions.
Treatment of zoster: acyclovir 800 mg 5×/day × 7 days (or valacyclovir 1g 3×/day × 7 days — preferred); treatment reduces duration of eruption and reduces risk of PHN if started within 72 hours of rash onset (or at any time if new lesions are still appearing). For immunocompromised patients or disseminated zoster: IV acyclovir 10 mg/kg 8-hourly. PHN management: tricyclic antidepressants (amitriptyline), gabapentin, pregabalin (first-line neurogenic pain agents), topical capsaicin, lidocaine patches.
Dengue Fever: Pathogenesis, Clinical Staging, and Fluid Management
Dengue fever is the most important arboviral disease in India, caused by dengue virus (DENV) — a flavivirus with four serotypes (DENV-1 to 4). It is transmitted exclusively by the bite of Aedes aegypti (the primary vector) and Aedes albopictus mosquitoes — both of which breed in clean, stagnant water in and around human habitations (flower pots, coolers, tyres, water storage containers), making dengue an urban and peri-urban disease. Dengue is hyperendemic in most Indian cities and towns, with major epidemics occurring annually during and after the monsoon season when mosquito breeding is at its peak.
Pathogenesis and the basis of severe dengue: Primary DENV infection with any one serotype induces serotype-specific immunity but also produces cross-reactive non-neutralising antibodies against other serotypes. Upon secondary infection with a different DENV serotype, these cross-reactive antibodies facilitate viral entry into Fc receptor-bearing monocytes/macrophages — antibody-dependent enhancement (ADE) — leading to higher viraemia and a more intense cytokine storm. This is the mechanistic basis for the observation that dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS) are more common in secondary dengue infections than in primary infections. The hallmark of severe dengue pathophysiology is plasma leakage — cytokines (TNF-α, IL-6, IL-8) increase vascular permeability, leading to transudation of plasma from the intravascular space into third spaces (pleural cavity, peritoneum) — producing hypovolaemia, haemoconcentration, and shock.
WHO 2009 dengue classification — three categories:
1. Dengue without warning signs: fever (abrupt onset, 39–41°C) lasting 2–7 days, severe headache, retro-orbital pain (classic 'behind the eyes' pain), severe myalgia and arthralgia ('bone-breaking fever' — dengue's colloquial name), macular/petechial rash (flushed face early → diffuse macular rash in days 3–4 → islands of white in a sea of red), nausea, vomiting. Tourniquet test (Rumpel-Leede test): inflate BP cuff to midpoint between systolic and diastolic pressure for 5 minutes; ≥10 petechiae per inch² = positive; indicates capillary fragility/thrombocytopenia; a positive tourniquet test in a febrile patient during dengue season is a strong indicator of dengue.
2. Dengue with warning signs (require hospital monitoring):
- Abdominal pain or tenderness
- Persistent vomiting
- Clinical fluid accumulation (ascites, pleural effusion, periorbital oedema)
- Mucosal bleed (gum bleed, epistaxis)
- Lethargy or restlessness
- Liver enlargement >2 cm
- Rapid increase in haematocrit with rapid decrease in platelet count
Warning signs indicate impending plasma leakage and evolving haemoconcentration — this is the critical stage where hospitalisation and active monitoring prevent progression to shock.
3. Severe dengue: severe plasma leakage → dengue shock syndrome (DSS); severe bleeding; severe organ impairment (liver, CNS, heart, kidneys). DSS presents with narrow pulse pressure (<20 mmHg), cold clammy extremities, tachycardia, and restlessness — hallmarks of distributive/hypovolaemic shock.
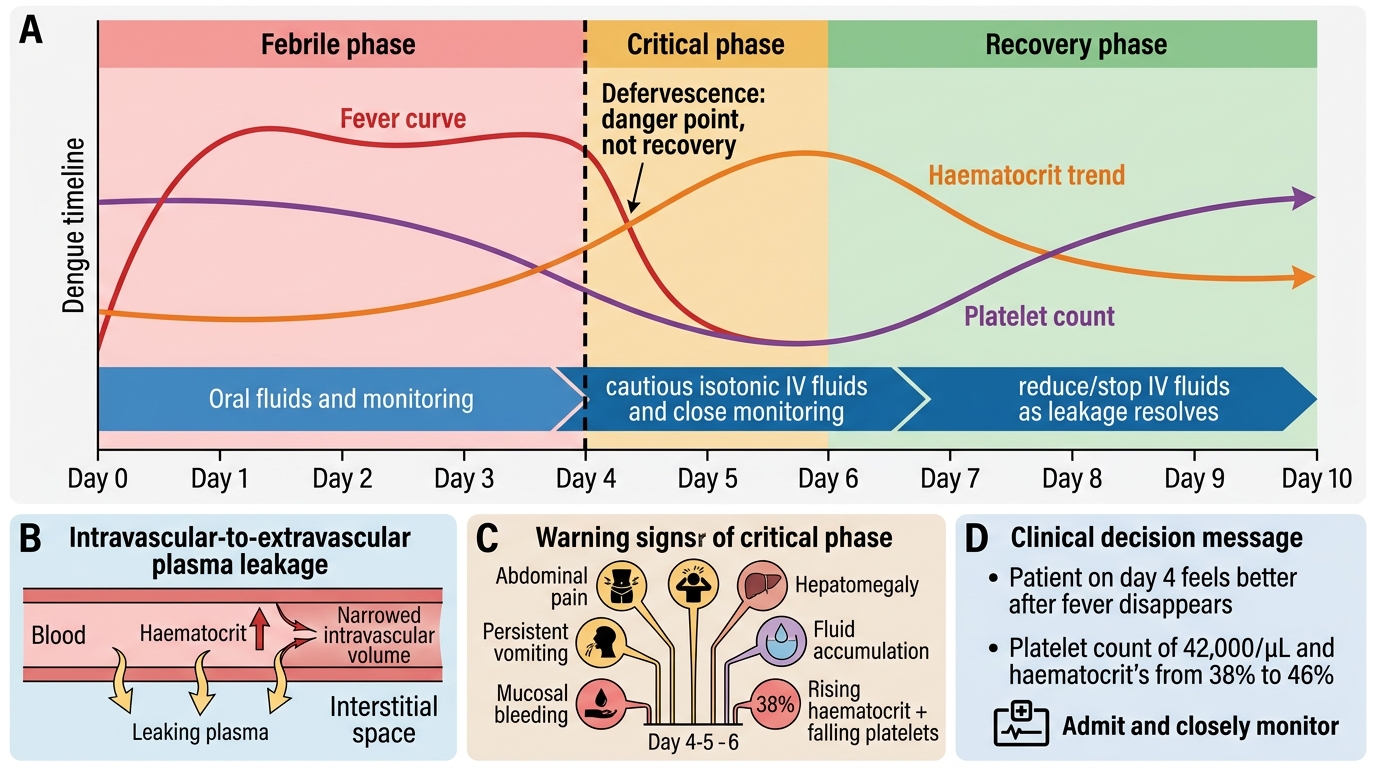
The critical phase: typically occurs day 3–6 of illness — the febrile phase ends (the patient appears to improve), but this is actually the danger window when plasma leakage is maximal. Careless discharge at defervescence, when the patient feels better, is the critical clinical error that leads to preventable dengue deaths.
Diagnosis: NS1 antigen detectable from day 1 to day 5 (early diagnosis, sensitivity 90% on day 1); dengue IgM ELISA becomes positive from day 5–6; PCR for dengue RNA (gold standard but not practical in most Indian centres). CBC: leucopenia (early hallmark), thrombocytopenia (progressively falling platelet count from day 3–4 onwards; rapid fall = warning sign), rising haematocrit (haemoconcentration = plasma leakage).
Dengue fluid management — the critical skill: There is no antiviral treatment for dengue; management is entirely supportive, with fluid resuscitation guided by clinical monitoring.
- Dengue without warning signs: oral rehydration; rest; paracetamol (NOT aspirin, NOT NSAIDs, NOT ibuprofen — all increase bleeding risk and can cause acute liver failure in dengue). Patient must be educated to return immediately if warning signs develop.
- Dengue with warning signs: IV isotonic crystalloid resuscitation — NS or Hartmann's solution; rate guided by haematocrit trends, urine output (target ≥0.5 mL/kg/hour), and vital signs; avoid over-hydration (causes pulmonary oedema — plasma continues to leak regardless of IV fluids, so the goal is to maintain perfusion, not to replace all leaked fluid).
- Dengue shock syndrome: rapid IV fluid bolus (10 mL/kg over 15–20 minutes); if haematocrit falls after improvement (suggests bleeding, not leakage), consider packed red cell transfusion; maintain oxygen; close ICU monitoring.
- Platelet transfusion: reserved for platelet count <10,000/µL OR platelet count <20,000/µL with active bleeding — NOT routine prophylactic transfusion for thrombocytopenia without bleeding.
Dengue Fever Timeline: Defervescence and Critical Phase
SELF-CHECK
A 28-year-old patient is admitted with dengue fever. On day 4 of illness, his fever suddenly disappears and he feels much better. His platelet count is 42,000/µL and haematocrit has risen from 38% to 46% over the past 24 hours. The MOST appropriate next action is:
A. Discharge the patient — fever resolution indicates recovery from dengue
B. Admit and closely monitor — defervescence on day 3–6 is the critical phase when plasma leakage is maximal despite apparent clinical improvement
C. Give prophylactic platelet transfusion to prevent bleeding
D. Start IV antibiotics — fever resolution indicates superimposed bacterial infection requiring coverage
Reveal Answer
Answer: B. Admit and closely monitor — defervescence on day 3–6 is the critical phase when plasma leakage is maximal despite apparent clinical improvement
Defervescence in dengue (day 3–6) is the critical phase, not recovery — this is when plasma leakage from the intravascular space is at its peak. The rising haematocrit (38%→46% = haemoconcentration) is a direct marker of plasma leakage. Discharging a patient at defervescence is the classic clinical error responsible for most preventable dengue deaths — the patient feels better but is at highest risk of progressing to dengue shock syndrome over the next 24–48 hours. Platelet transfusion is reserved for platelet count <10,000/µL or <20,000/µL with active bleeding — not prophylactic use at 42,000/µL. There is no indication for antibiotics — this is a viral illness without evidence of superinfection.
Rabies: Pathogenesis, Clinical Features, and Post-Exposure Prophylaxis
Rabies is caused by the rabies virus (genus Lyssavirus, family Rhabdoviridae), a bullet-shaped RNA virus transmitted in the saliva of infected animals — predominantly dogs (>95% of human cases in India), followed by bats, monkeys, cats, and jackals. India accounts for approximately 36% of the world's rabies mortality — an estimated 20,000 deaths annually — making it the global epicentre of human rabies. This burden is almost entirely preventable through prompt and correct post-exposure prophylaxis (PEP), yet delays in seeking care and incomplete PEP administration remain major barriers.
Provided image
Pathogenesis — why rabies is universally fatal once symptomatic: After inoculation by an infected animal bite, the rabies virus binds to nicotinic acetylcholine receptors and enters peripheral nerve endings at the wound site. The virus then travels centripetally (towards the CNS) via retrograde axoplasmic transport along peripheral nerves at approximately 3 mm/hour. This slow, protected travel through the nerve means that the virus is inaccessible to the immune system during the incubation period. Once the virus reaches the brain — specifically the hippocampus, cerebellum, and brainstem — it spreads rapidly throughout the CNS. At this point, clinical rabies develops, and the disease is virtually universally fatal (only a handful of authenticated survivals in world literature, all with incomplete vaccination history). The key clinical implication: the incubation period is the only window for intervention through PEP. The incubation period ranges from 10 days to more than 1 year (average 1–3 months); it is shorter for bites on the face/head/neck (proximity to the CNS) and longer for bites on the limbs.
Clinical phases of rabies:
- Prodromal phase (2–10 days): fever, malaise, headache, and — importantly — pain or paraesthesia at the healed bite site (this highly specific symptom occurs in ~50–80% of patients and indicates viral ascending neuritis at the original wound site; its presence should prompt immediate rabies workup even if the bite was weeks to months earlier).
- Encephalitic ('furious') rabies (~80% of cases): hydrophobia (violent pharyngeal/laryngeal spasms upon attempting to swallow water — triggered by the sensation of water against the throat, caused by virus-induced excitation of the swallowing reflex circuits); aerophobia (similar spasms triggered by air blowing on the face); hypersalivation; autonomic instability; periods of extreme agitation alternating with lucid intervals. This clinical picture is virtually pathognomonic of rabies.
- Paralytic ('dumb') rabies (~20%): ascending flaccid paralysis mimicking Guillain-Barré syndrome; less dramatic than furious rabies; more commonly associated with vampire bat bites in South America but occurs in India too; more easily misdiagnosed.
- Death occurs within 4–20 days of symptom onset, from respiratory failure or autonomic storm.
Diagnosis: clinical diagnosis in the encephalitic phase is straightforward. In the prodromal or paralytic phase: direct fluorescent antibody (DFA) test on a skin biopsy from the nape of the neck (hair follicle nerves) — the most accessible antemortem test; CSF or saliva PCR for rabies virus RNA; serum and CSF antibodies (only meaningful in vaccinated patients, since unvaccinated patients mount minimal antibody response before death).
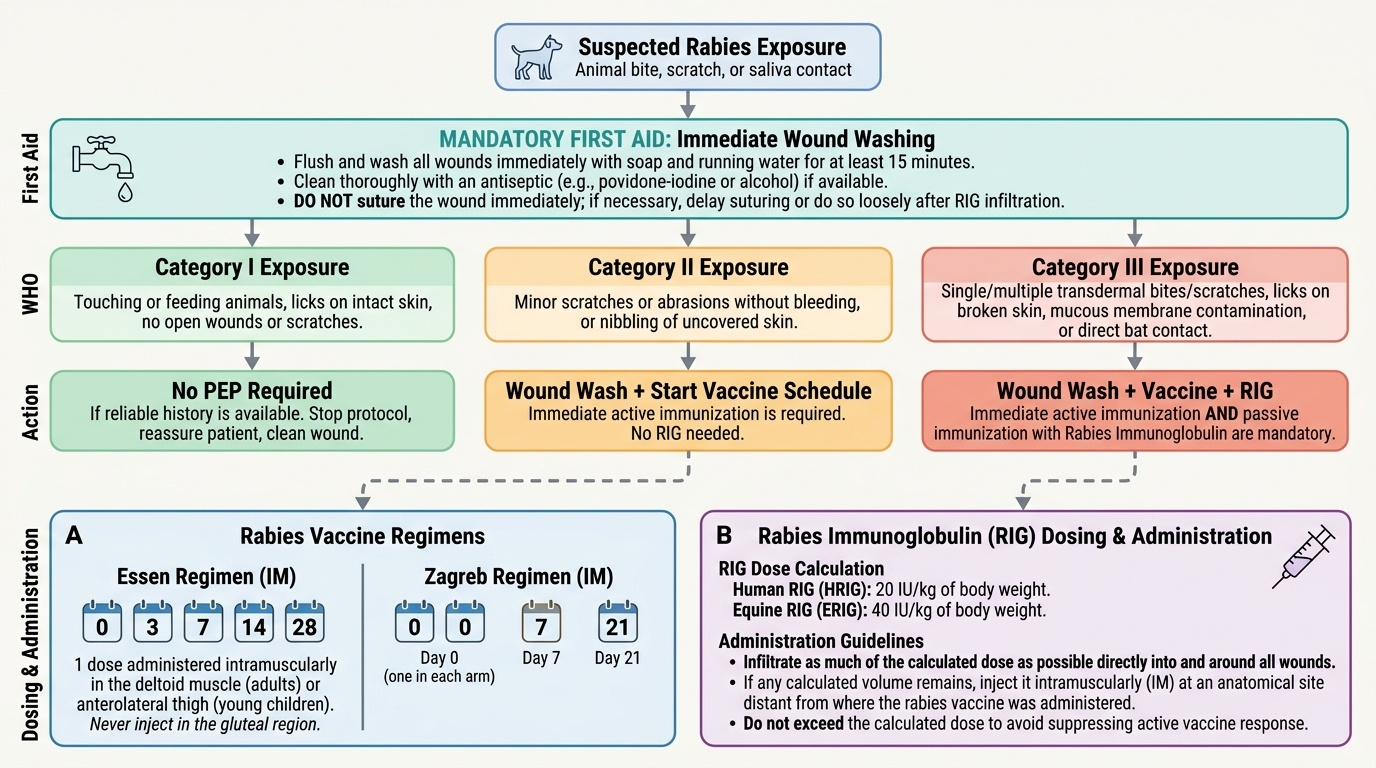
WHO/NVBDCP Post-Exposure Prophylaxis (PEP) — animal bite categories:
- Category I (touching or feeding of animals, licks on intact skin): no PEP required — rabies virus cannot penetrate intact skin.
- Category II (nibbling of uncovered skin, minor scratches/abrasions without bleeding, licks on broken skin): wound washing + anti-rabies vaccine. Vaccine schedule: Essen regimen — 5 doses IM (days 0, 3, 7, 14, 28); or updated Zagreb regimen — 4 doses (days 0×2 sites, 7, 21) — now preferred by WHO for cost-effectiveness.
- Category III (single or multiple transdermal bites/scratches, licks on mucous membranes, exposure to bats, all bites on the head/face/neck/hands/feet or in children): wound washing + anti-rabies vaccine + rabies immunoglobulin (RIG). RIG is injected at and around the wound site (to neutralise virus at the entry point before it enters nerve endings). Human RIG (HRIG): 20 IU/kg; equine RIG (ERIG): 40 IU/kg (less expensive, used where HRIG unavailable; skin test first — anaphylaxis risk). RIG is given on day 0 only.
Wound washing — the most important and most underperformed PEP step: Immediate, thorough wound washing with soap and water for ≥15 minutes — removes a large proportion of surface virus before it can enter nerve endings. This single step dramatically reduces the probability of rabies development even before the first vaccine dose. Patients must be educated to perform this at home immediately after a bite and before coming to the clinic.