Page 19 of 35
IM26.21-25 | Viral Infections: Herpesviruses, Respiratory Viruses, Rabies, and Dengue — SDL Guide (Part 2)
COVID-19, SARS, and Influenza: Respiratory Viral Syndromes
COVID-19 (Coronavirus Disease 2019) is caused by SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2), a positive-sense single-stranded RNA virus of the family Coronaviridae. SARS-CoV-2 emerged in Wuhan, China in December 2019 and was declared a pandemic by WHO in March 2020. India experienced two major waves (2020 wave 1; 2021 wave 2 driven by the Delta variant — associated with the highest mortality), followed by the Omicron variant wave in early 2022. Understanding COVID-19 pathogenesis is now fundamental to internal medicine, not just as a historical event but because it exemplifies the principles of pandemic respiratory viral disease that will apply to future novel coronavirus or influenza pandemics.
Pathogenesis of COVID-19: SARS-CoV-2 enters cells via the ACE2 receptor (angiotensin-converting enzyme 2), expressed highly on type II pneumocytes, airway epithelium, cardiac myocytes, vascular endothelium, and intestinal enterocytes — explaining the multi-system disease. The spike protein S1 subunit binds ACE2; TMPRSS2 (a serine protease) primes the spike for membrane fusion. Two mechanisms of injury: (1) direct viral cytopathic effect in the first 1–2 weeks; and (2) dysregulated immune/inflammatory response ('cytokine storm') — predominating in the second week, causing ARDS, multi-organ dysfunction, and coagulopathy. SARS-CoV-2-associated coagulopathy (COVID-coagulopathy): elevated D-dimer, elevated fibrinogen, thrombocytopenia, and in-situ pulmonary and systemic thrombi — markedly increases mortality in hospitalised patients.
Clinical spectrum of COVID-19:
- Asymptomatic / mild illness (~80%): upper respiratory symptoms (coryza, sore throat, fever), loss of smell (anosmia) and taste (ageusia) — these were highly specific symptoms in early pandemic strains though less specific with Omicron. Managed at home; requires self-isolation.
- Moderate illness: persistent fever, significant dyspnoea, SpO2 88–94% on room air; bilateral infiltrates on CXR/CT; hospital admission and supplemental oxygen required.
- Severe/critical illness (~5%): ARDS (SpO2 <88%, bilateral infiltrates, PaO2/FiO2 <200 mmHg); cytokine storm; multi-organ failure; ICU, high-flow nasal oxygen, non-invasive or invasive mechanical ventilation; mortality 20–40% in critical cases.
Treatment: dexamethasone 6 mg daily × 10 days — reduces mortality in mechanically ventilated patients (RECOVERY trial — the landmark evidence), by suppressing cytokine storm; NOT beneficial in mild disease without oxygen requirement (may be harmful). Remdesivir (IV, days 1–5): antiviral; reduces time to recovery in hospitalised patients on oxygen but no clear mortality benefit in most trials. Anticoagulation: therapeutic-dose LMWH in moderate-severe hospitalised COVID-19 reduces thrombotic complications. Oxygen therapy: early, adequate supplemental oxygen (target SpO2 ≥94%) is the most critical intervention; prone positioning (awake proning) reduces the need for mechanical ventilation in moderate-severe hypoxaemia.
SARS (Severe Acute Respiratory Syndrome): caused by SARS-CoV-1 (2002–2003 epidemic); similar ACE2 entry mechanism; case fatality rate ~10%; contained by aggressive infection control measures — no vaccine developed. Important as a historical precursor to COVID-19.
Influenza: caused by influenza A (most clinically significant — causes pandemics) and influenza B viruses. Antigenic drift (gradual mutation of HA/NA — basis of seasonal epidemics, requires annual vaccine reformulation) and antigenic shift (reassortment of HA/NA segments between human and animal strains — H1N1 pandemic 2009, H3N2, H5N1 avian influenza — basis of pandemics). Clinical features: abrupt onset of fever, chills, severe myalgia (disproportionate — the hallmark distinguishing influenza from common cold, where myalgia is mild or absent), headache, dry cough, nasal congestion. Complications: primary influenza pneumonia, secondary bacterial pneumonia (Streptococcus pneumoniae, Staphylococcus aureus — most dangerous in the elderly), myocarditis, encephalitis. High-risk groups: elderly, pregnant women, children <5 years, immunocompromised, chronic disease (cardiac, pulmonary, renal, hepatic). Treatment: oseltamivir (Tamiflu) 75 mg twice daily × 5 days within 48 hours of symptom onset; reduces duration and complications. Prophylaxis: annual influenza vaccine (trivalent or quadrivalent inactivated; updated yearly); indicated for all high-risk groups. H5N1 avian influenza: bird-to-human transmission (not sustained human-to-human); very high CFR (~60%); pandemic threat if human-to-human transmission develops — a key public health surveillance priority.
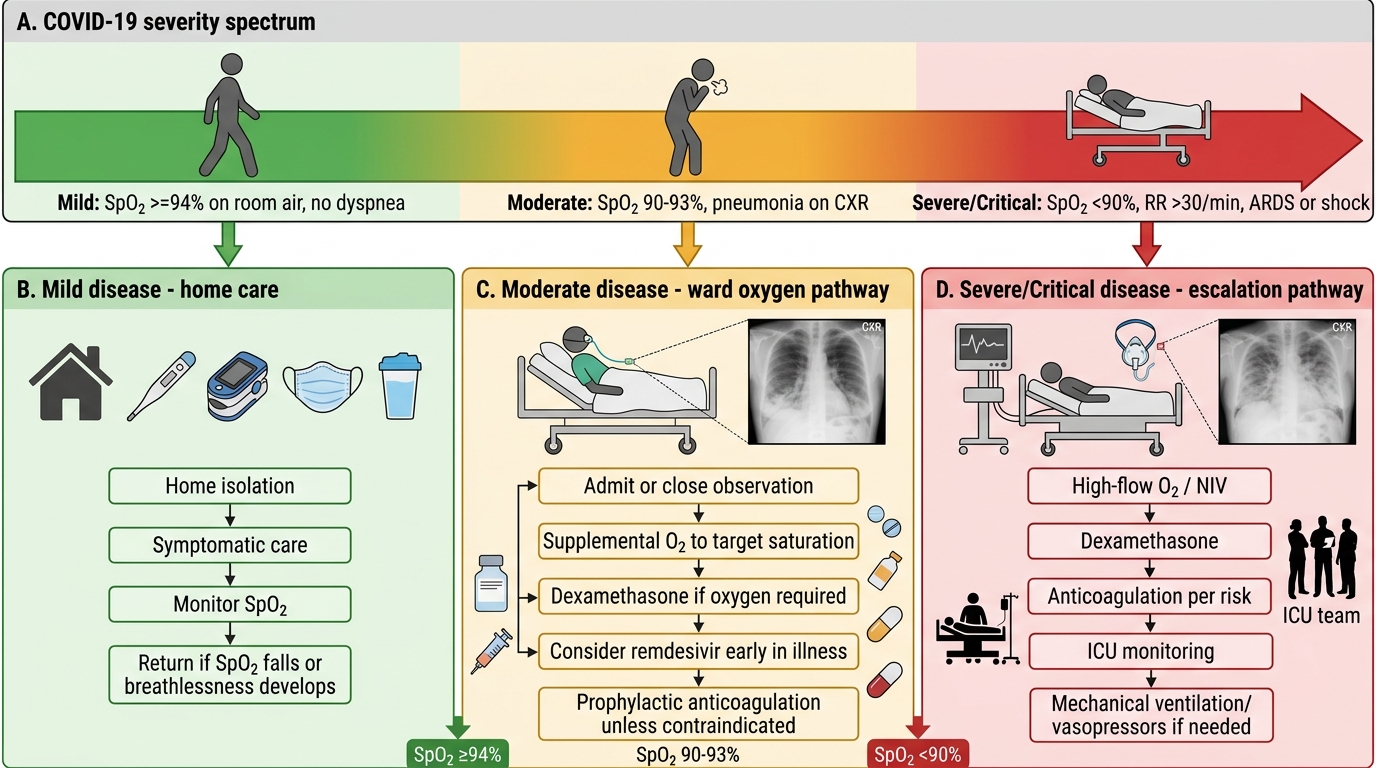
COVID-19 Severity Spectrum and Treatment Ladder
SELF-CHECK
A 35-year-old woman is bitten on the right hand by a stray dog while walking in Chennai. The bite breaks the skin and causes bleeding. She arrives at a clinic 6 hours later. The dog ran away and cannot be observed. What is the CORRECT post-exposure management?
A. Observe for 10 days — if the dog is not found and shows no signs of rabies, no PEP is needed
B. Wound washing + anti-rabies vaccine (Essen 5-dose schedule) only — Category II bite does not require immunoglobulin
C. Wound washing + anti-rabies vaccine + rabies immunoglobulin (RIG) at and around the wound — this is a Category III exposure
D. Wound washing only — dog bites rarely cause rabies in India and the bite is on the hand, not the face
Reveal Answer
Answer: C. Wound washing + anti-rabies vaccine + rabies immunoglobulin (RIG) at and around the wound — this is a Category III exposure
A transdermal bite (breaking skin, causing bleeding) is a Category III exposure per WHO/NVBDCP — requiring wound washing + anti-rabies vaccine + rabies immunoglobulin (RIG). A bite on the hand is still Category III because it breaks the skin. RIG (HRIG 20 IU/kg or ERIG 40 IU/kg) must be infiltrated at and around the wound site on day 0; it is NOT given with subsequent vaccine doses. The stray dog ran away and cannot be observed — this eliminates the 10-day observation option (observation is only useful when the biting animal is available for monitoring). India is high-endemicity for rabies; the presumption in the absence of the animal is that PEP is required. Wound washing alone is wholly insufficient for a Category III bite.
Clinical Approach to Diagnosis of Major Viral Infections
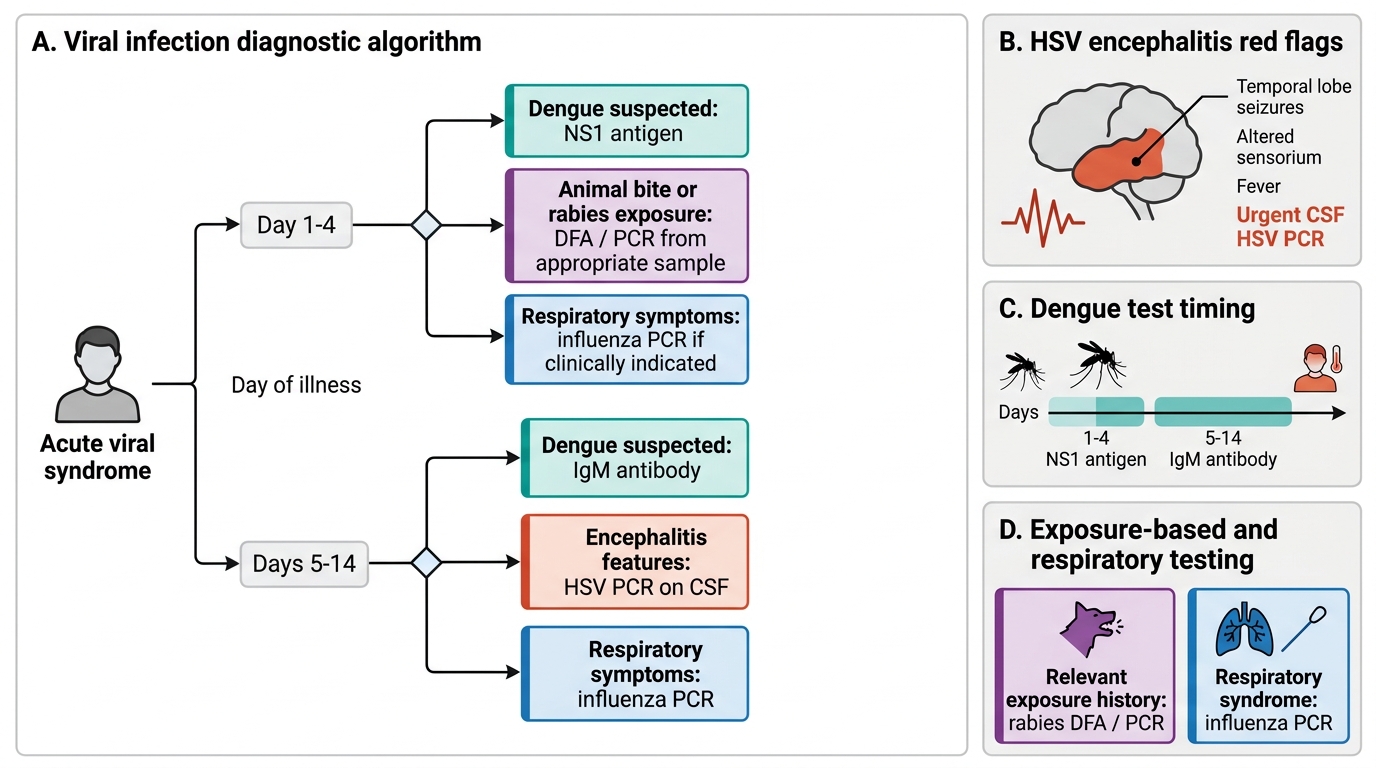
A structured diagnostic approach to viral infections requires integrating the exposure history, incubation period, and clinical syndrome before ordering tests. The following principles apply across the viral infections covered in this SDL.
Herpes infections — diagnostic approach: HSV and VZV are predominantly clinical diagnoses when the rash is typical. HSV encephalitis is the major exception — all patients with acute encephalitis must have CSF PCR for HSV immediately, since early antiviral treatment is life-saving. For atypical mucocutaneous HSV, Tzanck smear (multinucleated giant cells — rapid but non-specific) or viral culture can confirm. For HSV keratitis, slit-lamp examination with fluorescein staining reveals the pathognomonic dendritic ulcer — do NOT apply topical steroids before this examination.
Dengue — diagnostic approach: The choice of diagnostic test depends on the day of illness:
- Day 1–5 (febrile phase): NS1 antigen — sensitivity 90% on day 1, declines after day 5.
- Day 5 onwards (critical/recovery phase): dengue IgM ELISA — rises after day 5; paired IgM/IgG ratio distinguishes primary from secondary infection.
- CBC throughout: leucopenia (hallmark of viral fever in dengue), thrombocytopenia, rising haematocrit (haemoconcentration in critical phase). A daily CBC in hospitalised dengue patients tracks the three key parameters: WBC (rising WBC may indicate bacterial superinfection), platelet trend (falling rate is clinically more important than the absolute count), and haematocrit (rising = plasma leakage).
- USS abdomen: detects ascites and pleural effusion (markers of plasma leakage) even before clinical signs are obvious.
Rabies — diagnostic approach: In the encephalitic phase, diagnosis is clinical (hydrophobia + aerophobia + bite history = pathognomonic). For laboratory confirmation: skin biopsy DFA (nape of neck — tests hair follicle nerve fibres), saliva or CSF PCR, corneal impression smear. Serology is only meaningful in vaccinated patients. Brain biopsy post-mortem: Negri bodies (eosinophilic intraneuronal inclusion bodies in the hippocampus and cerebellum) — the histological hallmark of rabies.
Influenza — diagnostic approach: Rapid antigen test (nasal/nasopharyngeal swab) — low sensitivity (~50–70%), useful for point-of-care triage. RT-PCR (nasopharyngeal swab) — the gold standard, sensitivity >95%; used for outbreak investigation and antiviral decision-making in high-risk patients. In severe influenza pneumonia, CXR shows bilateral interstitial infiltrates.
COVID-19 — diagnostic approach: RT-PCR (nasopharyngeal swab) remains the confirmatory standard. Rapid antigen tests — useful for surge situations, lower sensitivity. HRCT chest: ground-glass opacities in bilateral peripheral/subpleural distribution (COVID-19 CT pattern) — useful for characterising severity and complications; not required for routine diagnosis. D-dimer elevation >1 µg/mL is a marker of COVID-coagulopathy and poor prognosis in hospitalised patients.
Viral Infection Symptom-to-Test Diagnostic Algorithm
Antiviral Treatment and Vaccination: Principles and Specific Agents
The management of viral infections combines specific antiviral therapy (where available) with supportive care. For several important viral infections covered in this SDL — dengue, rabies once symptomatic — there is NO effective antiviral treatment, and management is entirely supportive. This underscores the critical importance of prevention: vector control for dengue, PEP for rabies, and vaccination for influenza, varicella, and COVID-19.
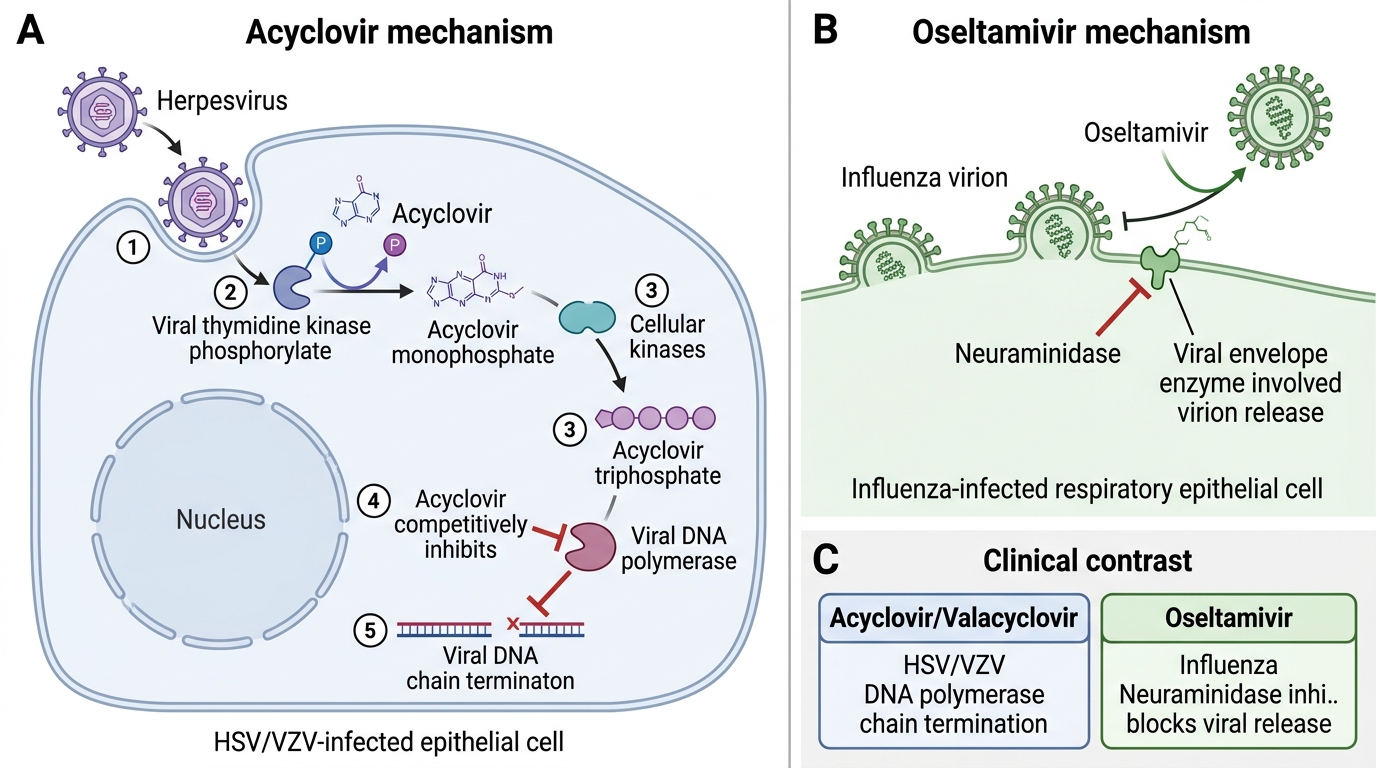
Acyclovir and antiherpesviral agents: Acyclovir is the prototype nucleoside analogue antiviral. It is phosphorylated preferentially by HSV/VZV thymidine kinase (TK) to acyclovir monophosphate, then by cellular kinases to the active triphosphate, which acts as a selective inhibitor of viral DNA polymerase — with minimal toxicity to uninfected cells. Acyclovir-resistant HSV (TK-deficient mutants) occurs in immunocompromised patients who receive prolonged acyclovir therapy; second-line: IV foscarnet (does not require TK phosphorylation). Valacyclovir (prodrug → acyclovir, higher oral bioavailability) is preferred over oral acyclovir in clinical practice for most outpatient HSV/VZV indications. Famciclovir (another oral antiviral for HSV/VZV) has equivalent efficacy.
Antiviral agents in this SDL:
| Infection | First-line antiviral | Route/dose | Duration | Key condition for efficacy |
|---|---|---|---|---|
| HSV labialis/genital | Acyclovir 200 mg 5×/day or valacyclovir 500 mg BD | Oral | 5–10 days | Start within 48–72 h of rash |
| HSV encephalitis | Acyclovir 10 mg/kg IV 8-hourly | IV | 14–21 days | Start immediately, don't wait for PCR |
| Varicella (adult/immunocompromised) | Acyclovir 800 mg 5×/day or valacyclovir 1g TDS | Oral or IV | 7 days | Start within 24h of rash |
| Herpes zoster | Valacyclovir 1g TDS or acyclovir 800 mg 5×/day | Oral | 7 days | Start within 72h of rash |
| Influenza | Oseltamivir 75 mg BD | Oral | 5 days | Start within 48h of symptoms |
| COVID-19 (hospitalised, oxygen) | Remdesivir + dexamethasone 6 mg OD | IV + oral | 5 days / 10 days | Oxygen-requiring patients |
| Dengue | No antiviral available | — | — | Supportive care only |
| Rabies (symptomatic) | No effective antiviral | — | — | PEP before symptoms = only intervention |
Vaccination — preventable viral diseases:
- Influenza: annual inactivated influenza vaccine; recommended for all adults >65, healthcare workers, pregnant women, children 6 months–5 years, and patients with chronic cardiorespiratory/metabolic disease. Live attenuated intranasal vaccine available for children 2–49 years.
- Varicella: varicella vaccine (live attenuated Oka strain) is part of the private immunisation schedule in India (2 doses at 12–15 months and 4–6 years); not yet in the national immunisation programme. Adults without prior varicella: 2 doses of varicella vaccine, 4–8 weeks apart.
- Herpes zoster: recombinant zoster vaccine (RZV — Shingrix) is recommended for adults ≥50 years (even if they previously had zoster); 94% efficacy against zoster and PHN; 2-dose schedule (0 and 2–6 months). NOT available in India's public sector at present.
- COVID-19: multiple vaccines used in India — Covaxin (inactivated whole virus, BBV152), Covishield (ChAdOx1 — adenoviral vector), Corbevax (protein subunit); booster doses recommended for immunocompromised and elderly.
- Rabies (pre-exposure prophylaxis — PrEP): indicated for veterinarians, laboratory workers handling rabies virus, forest/wildlife officers, travellers to highly endemic areas; 3-dose schedule (days 0, 7, 21) intramuscularly.
Acyclovir and Oseltamivir: Antiviral Mechanisms
SELF-CHECK
A 68-year-old diabetic patient presents with a 4-day history of severe lancinating pain along the left T6 dermatome, followed 1 day ago by a unilateral vesicular rash along the same distribution. He has not yet started any treatment. The MOST appropriate management is:
A. Topical acyclovir cream applied to the vesicles — systemic antivirals are not required for localised herpes zoster
B. IV acyclovir 10 mg/kg 8-hourly — all herpes zoster in immunocompromised/diabetic patients requires IV treatment
C. Oral valacyclovir 1g three times daily × 7 days + adequate analgesia — initiate within 72 hours of rash onset
D. Wait 5 days before starting antivirals — treatment is only effective if started after the rash has reached its maximum extent
Reveal Answer
Answer: C. Oral valacyclovir 1g three times daily × 7 days + adequate analgesia — initiate within 72 hours of rash onset
Herpes zoster in an older diabetic patient (high risk for postherpetic neuralgia) should be treated with oral valacyclovir 1g TDS × 7 days (or acyclovir 800 mg 5×/day × 7 days) initiated within 72 hours of rash onset — this reduces both the duration of the acute eruption and the risk of postherpetic neuralgia. The rash appeared 1 day ago, so treatment is timely and appropriate. Topical acyclovir cream has no efficacy for herpes zoster (poor skin penetration, not indicated). IV acyclovir is reserved for disseminated zoster, ophthalmic zoster with threatened vision, zoster in severely immunocompromised patients, or patients unable to take oral therapy — not required for uncomplicated dermatomal zoster in a diabetic patient who is not severely immunocompromised. Delaying antivirals reduces their efficacy — treatment must start within 72 hours.