Page 20 of 35
IM26.21-25 | Viral Infections: Herpesviruses, Respiratory Viruses, Rabies, and Dengue — SDL Guide (Part 3)
Self-Assessment: Viral Infections
You have now covered the five major viral infection groups in this SDL. The following scenarios apply the diagnostic and management principles across these conditions. Work through each before reading the analysis.
Provided image
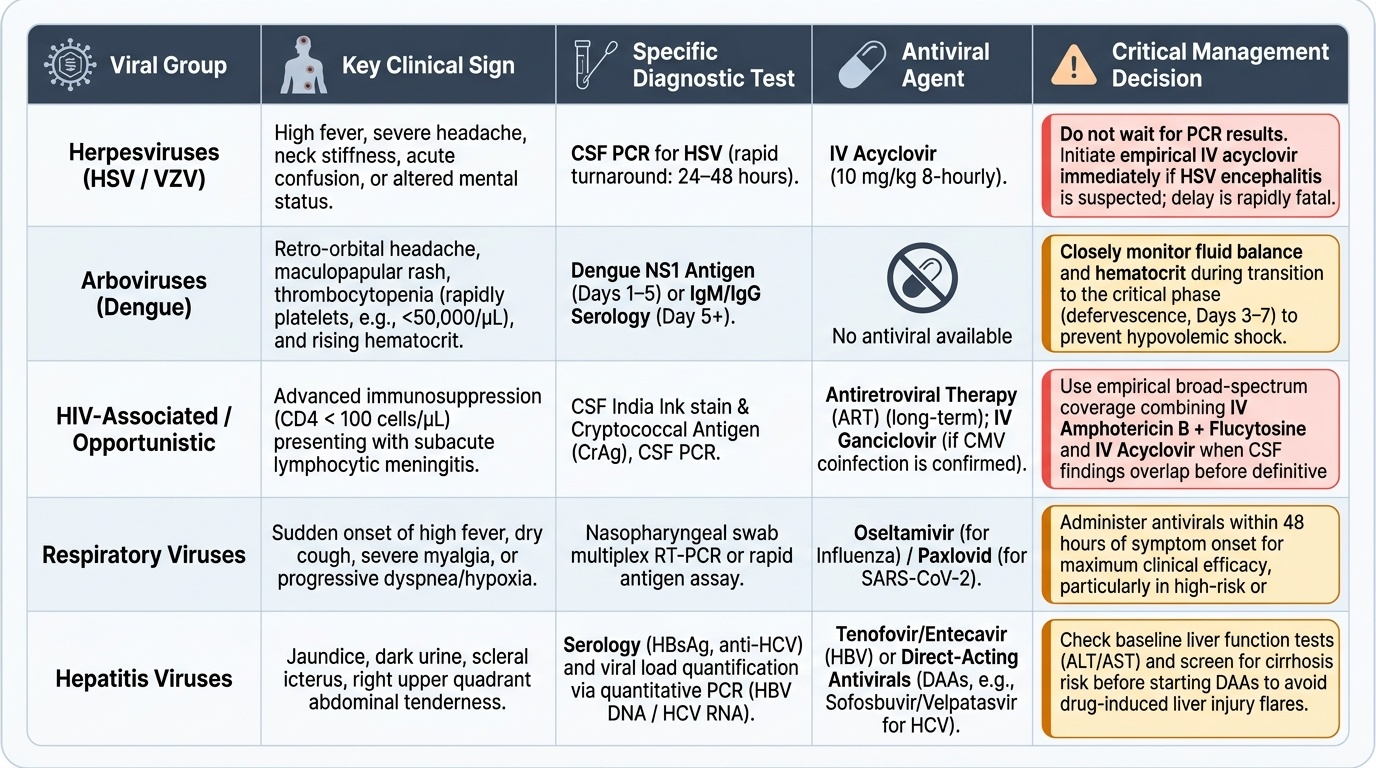
Scenario A: A 45-year-old HIV-positive patient (CD4 count 85 cells/µL) develops high fever, severe headache, neck stiffness, and confusion over 48 hours. CSF examination: opening pressure 320 mm H2O, lymphocytes 120 cells/µL, protein 110 mg/dL, glucose 30 mg/dL (blood glucose 90 mg/dL). CSF Gram stain: negative. India ink stain: pending.
Analysis: HIV with CD4 <200 + subacute meningitis + lymphocytic CSF with low glucose + elevated opening pressure → the differential is cryptococcal meningitis (most likely with these CSF findings in AIDS) OR HSV encephalitis (though HSV CSF typically has normal glucose). Pending India ink result: if positive = cryptococcal meningitis (IV amphotericin B + flucytosine induction × 2 weeks). However, HSV encephalitis must also be excluded — order CSF PCR for HSV (results in 24–48 hours). Until results return, empirical IV acyclovir 10 mg/kg 8-hourly should be added (given the temporal lobe involvement in HSV encephalitis is rapidly fatal without treatment). This is a case where empirical broad-spectrum treatment covering both diagnoses is safer than waiting.
Scenario B: A 32-year-old software professional presents to the emergency department at midnight with a 5-day fever, severe retro-orbital headache, maculopapular rash, and platelet count falling from 120,000 on day 3 to 38,000 today (day 5). He appears anxious but oriented. BP 102/78 mmHg, HR 108 bpm, SpO2 99% on room air. Haematocrit 48% (baseline 42%).
Analysis: Dengue fever in the critical phase — day 5 of illness with thrombocytopenia, rising haematocrit (+6% = significant haemoconcentration), tachycardia, and mildly low BP. This patient has dengue warning signs (rapid haematocrit rise + platelet fall, possibly impending shock — narrow pulse pressure 24 mmHg is borderline). Admit; IV isotonic crystalloid; close monitoring every 2–4 hours (HR, BP, urine output, haematocrit); avoid NSAIDs (already a risk — check what he has been taking for pain). Do NOT discharge. Paracetamol for fever only. Platelet transfusion is NOT indicated at 38,000/µL without active bleeding.
Scenario C: A healthcare worker who administered first aid to a rabies-affected patient (who was hypersalivating and had bitten a family member) asks about her rabies risk. She did not directly handle the patient's saliva but was splashed on the forearm (intact skin) with some saliva.
Analysis: Intact skin exposure to saliva = WHO Category I — rabies virus cannot penetrate intact, unbroken skin. Wash the area thoroughly with soap and water (always the first step). No vaccine or RIG is required. Educate the healthcare worker about the Category I classification and document the incident. Had her skin been broken (e.g., had a cut on the forearm), it would be Category III requiring full PEP.
Scenario D: A 70-year-old man with COPD and diabetes is admitted with high fever (39.5°C), severe myalgia, and progressive shortness of breath in January. CXR shows bilateral lower lobe infiltrates. He received no influenza vaccine this season. Rapid antigen test for influenza A: positive.
Analysis: Influenza A pneumonia in a high-risk patient (elderly, COPD, diabetes) — start oseltamivir 75 mg twice daily × 5 days immediately (within 48 hours of symptom onset, or at any point in severe disease); supplemental oxygen; monitor for secondary bacterial pneumonia (Streptococcus pneumoniae, Staphylococcus aureus — may require empirical antibiotics if deterioration occurs or infiltrates progress beyond 48–72 hours). This case also highlights the missed prevention opportunity — annual influenza vaccine is specifically recommended for COPD and diabetic patients.
CLINICAL PEARL
Four high-yield clinical pearls for this SDL: (1) In dengue, the critical phase is NOT when the patient feels worst — it is when the fever breaks on days 3–6 and the patient appears to be improving. Rising haematocrit signals plasma leakage and impending shock. Discharging a dengue patient at defervescence has caused preventable deaths. (2) Rabies PEP Category III requires BOTH vaccine AND RIG — vaccine alone is insufficient for a Category III bite. RIG is given only on day 0, at and around the wound; it is NOT given on subsequent vaccine days. (3) For HSV encephalitis, start IV acyclovir 10 mg/kg 8-hourly immediately on clinical suspicion — do not wait for CSF PCR results to return. Delay in treatment worsens outcomes; the treatment is safe and highly specific. (4) Dexamethasone 6 mg daily × 10 days reduces mortality in oxygen-requiring COVID-19 patients — but is NOT beneficial and may be harmful in mild COVID-19 that does not require oxygen.