Page 5 of 18
IM27.{5-6,8} | Tuberculosis Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit a structured TB history covering symptom constellation (cough, fever, night sweats, weight loss, haemoptysis) and systematic risk-factor assessment (contact, prior TB, HIV, DM, immunosuppression, occupation)
- Perform a systematic physical examination for TB including general state, chest (inspection/palpation/percussion/auscultation), lymphatic system, and relevant CNS assessment
- Generate a prioritised differential diagnosis ranked by probability, with distinguishing clinical features identified for each entry, based on the history and examination findings
INSTRUCTIONS
This is a skills-based SDL focused on clinical evaluation of presumptive tuberculosis. All three competencies (IM27.5, IM27.6, IM27.8) are at the SH level — simulation practice and clinical encounters are essential to convert this knowledge into skill. Use this module to understand the rationale and sequence of each element of the evaluation; then practise on ward patients and in structured clinical simulation.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Clinical Evaluation of TB (textbook)
- API Textbook of Medicine, 10th ed. — Clinical features of Tuberculosis (textbook)
- Macleod's Clinical Examination, 14th ed. — Respiratory System (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Sunita, a 28-year-old schoolteacher, presents to the outpatient clinic with 'persistent cough' for three weeks. She had initially attributed it to a cold, but now notes evening fevers, difficulty sleeping due to soaking night sweats, and she has lost four kilograms over six weeks. Her husband was treated for TB two years ago. As you settle into the consultation, you realise that this encounter will test exactly the clinical skills that distinguish a competent physician from an average one: the ability to elicit a structured, complete TB history that covers risk factors, contacts, and the full symptom constellation; to perform a systematic chest and lymph node examination with enough precision to identify early signs of pulmonary TB; and to integrate history and examination findings into a prioritised differential diagnosis. Sunita's story could resolve in minutes into a high-probability clinical picture — or it could unfold into something far more complex. The outcome depends almost entirely on how you approach the next thirty minutes of clinical evaluation.
WHY THIS MATTERS
The clinical evaluation of a patient with presumptive tuberculosis is one of the highest-yield skill sets in internal medicine practice in India, where TB incidence is nearly 200 per 100,000 population. Competencies IM27.5 (eliciting and documenting a structured TB history including risk factors and contacts), IM27.6 (performing a systematic examination including general state, chest, lymphatic system, and relevant CNS assessment), and IM27.8 (generating a prioritised differential diagnosis from clinical history and examination findings) are assessed at the SH (Skill in structured or simulated setting) level in the NMC framework. This means you are expected not just to know what to ask and look for, but to actually do it — correctly, systematically, and in the right order — with a real or simulated patient in front of you. These skills are the gate through which every TB diagnosis passes before any investigation. A missed risk factor or an unseen cervical lymph node chain can mean a missed diagnosis, a delayed prescription, and weeks of continued transmission.
RECALL
Before you proceed, recall the clinical anatomy and physiology you will apply during this examination. The lungs occupy the thoracic cage bilaterally; the right lung has three lobes (upper, middle, lower), the left has two (upper and lower). The apices project above the clavicles anteriorly and above the first rib posteriorly — an area frequently involved in post-primary TB, making supraclavicular percussion and auscultation essential. The trachea is midline at rest; deviation occurs toward the side of collapse (lung volume loss) and away from the side of a large effusion or tension pneumothorax. Recall the percussion note qualities: resonant (normal air-filled lung), stony dull (pleural effusion — most dull note in clinical medicine), dull (consolidated lung or thick pleural disease), and hyper-resonant (pneumothorax or emphysema). Breath sounds: vesicular over normal lung, bronchial over consolidation (air bronchogram equivalent), diminished/absent over effusion or collapse. Added sounds: crepitations (crackling) — coarse in secretions/bronchiectasis, fine in alveolar disease; rhonchi (wheeze) in airway narrowing. The lymphatic drainage of the lungs runs to hilar, then paratracheal nodes — which is why hilar adenopathy is the radiological signature of primary TB and why cervical adenopathy is the most common extrapulmonary presentation.
Eliciting a Structured TB History — Risk Factors, Contacts, and Symptom Constellation
The clinical indication for a structured TB history is the presence of any symptom lasting more than 2–3 weeks in a high-burden setting — but in India, the threshold for systematic TB history-taking should be even lower, given that the pre-test probability of TB in almost any symptomatic adult is significant. The NTEP four-symptom screen (cough, fever, night sweats, weight loss) is the entry-level alert; what follows is the more detailed structured history that every clinician should be capable of eliciting and documenting. The value of a complete, structured TB history lies not merely in confirming a suspicion, but in actively quantifying the pre-test probability before any investigation is ordered, in identifying risk factors that will change the treatment choice (HIV, prior TB, possible drug-resistant contact), and in flagging household contacts who require urgent evaluation. History-taking in TB is therefore both diagnostic and preventive — it is the first public health act of the clinical encounter.
Section 1 — Presenting complaint and symptom characterisation:
Begin with the presenting complaint in the patient's own words, then systematically characterise each symptom:
- Cough: Duration (the most important single datum — ≥2–3 weeks is the NTEP threshold for presumptive TB); character (productive/non-productive); sputum quantity and colour (mucopurulent, blood-stained); haemoptysis (amount — streaking versus frank, bright red versus dark). Haemoptysis in TB typically arises from erosion of a vessel by caseous necrosis or from a residual Rasmussen aneurysm in a healed cavity.
- Fever: Pattern (evening/nocturnal pyrexia is the TB hallmark — the Pel-Ebstein pattern of cyclic fever is associated with lymphoma, not TB); duration; associated rigors (uncommon in TB — rigors suggest pyogenic bacterial infection).
- Night sweats: Drenching (requiring change of clothes or bed linen) versus simple warmth at night — the former is the clinically significant descriptor. Night sweats in TB reflect circulating TNF-α and cytokines from ongoing granulomatous activity.
- Weight loss: Quantify — ask specifically how much weight lost over what period. Weight loss >5% in 6 months is clinically significant. Appetite change (TB typically causes anorexia; HIV-associated wasting may be more prominent).
- Breathlessness: Onset, exercise tolerance, orthopnoea. Breathlessness suggests pleural effusion (most common cause of new unilateral dull percussion in India), extensive pulmonary disease, or a pneumothorax.
- Chest pain: Pleuritic (sharp, worse on inspiration) suggests pleural inflammation; constant ache may reflect rib involvement in skeletal TB.
- Symptoms of extrapulmonary TB: Ask specifically about neck lumps (TB lymphadenitis), back pain and leg weakness (Pott's disease — urgent), headache and neck stiffness (TB meningitis — emergency), swelling of joints (TB arthritis), haematuria and dysuria (renal TB — sterile pyuria).
Section 2 — TB risk factors:
A structured risk-factor assessment transforms the consultation from a passive symptom list into an active probability estimation. Document each of the following:
- Contact history: Has the patient had prolonged close contact (household or workplace) with a known or suspected TB case? Was the contact smear-positive or drug-resistant? When did contact occur?
- Previous TB: Has the patient ever had TB before? Was it treated, for how long, and with what result? Prior TB doubles the risk of recurrence from reactivation or reinfection; prior treatment non-completion dramatically raises the risk of drug resistance.
- HIV status: Known positive? Last CD4 count? On ART? If HIV status unknown, counsel and offer testing — it is now routine in the NTEP framework.
- Diabetes: Known diabetic? Blood glucose control? Poorly controlled diabetes is an independent predictor of TB severity, treatment failure, and recurrence.
- Immunosuppressive therapy: Corticosteroids (dose and duration), TNF-α blockers, chemotherapy.
- Malnutrition/low BMI: Visually assess; confirm with weight and height.
- Occupation: Healthcare worker (high occupational exposure), dusty trades (silicosis + TB = silicotuberculosis — high risk, poor treatment response), overcrowded workplaces.
- Residential history: Overcrowded housing, prison, hostel, tea estate worker.
- Substance use: Smoking (impairs mucociliary clearance and macrophage function — approximately doubles TB risk), alcohol (hepatotoxicity relevant to drug monitoring, immune suppression).
- Age and sex: Young adult males most at risk in India; post-menopausal women also at risk from hormonal immune modulation.
Section 3 — Documenting and presenting the history:
When documenting the TB history, use a structured format: presenting complaint → history of present illness (chronological, symptom-by-symptom) → risk factors (enumerated systematically) → past medical history (prior TB, other chronic illness) → drug history (current medications, prior anti-TB drugs) → family history (TB in parents or siblings) → social history (occupation, housing, contacts, substance use). In the clinical setting, the presentation should conclude with a summary statement that contextualises the probability: "This is a 28-year-old schoolteacher with 3 weeks of productive cough, evening fever, night sweats, and 4 kg weight loss, with a household contact with TB 2 years ago. The pre-test probability for active pulmonary TB is high."
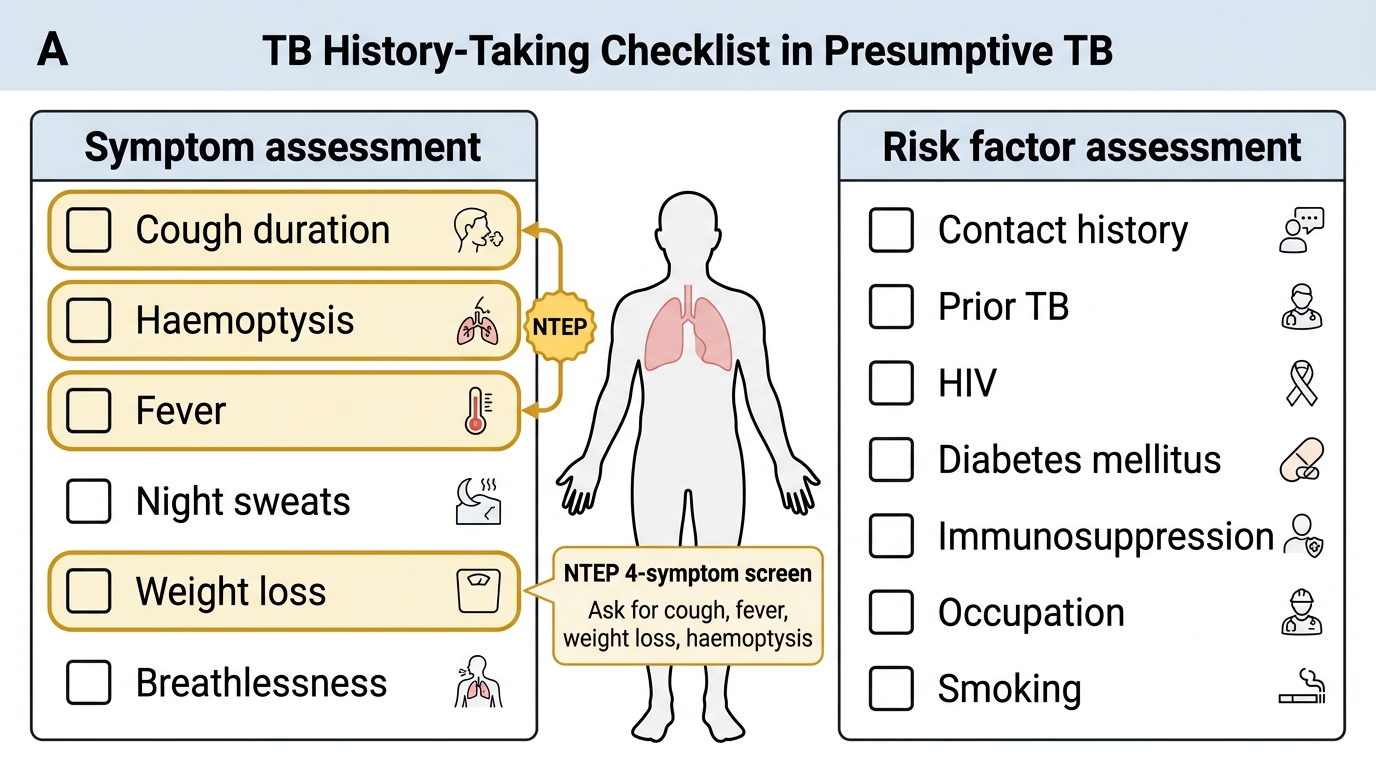
Structured TB History-Taking Checklist
Systematic Physical Examination in Presumptive TB
The clinical examination of a patient with presumptive TB requires a structured, head-to-toe approach that begins with general observation and proceeds through specific organ systems. The examination integrates findings from the general state, the chest and lungs, the lymphatic system, and — where clinical context demands — the neurological system. Each component provides data that refines the differential diagnosis and identifies complications before investigations are ordered. The governing principle underlying every element of the TB examination is this: the body's immune and physiological responses to M. tuberculosis are detectable on physical examination weeks before they are confirmed microbiologically. Apical dullness, post-tussive crepitations, matted cervical nodes, and meningeal signs are physical-examination translations of granuloma formation, cavitation, lymph node caseation, and basilar meningitis respectively. Learning to elicit and interpret these signs correctly is the difference between a diagnosis made at the bedside and one deferred for days while the patient continues to be infectious.
A. General Examination:
Begin before the formal examination begins — observe the patient walking into the room and sitting before you. Systematically document:
- Nutritional status: Body habitus, muscle wasting (temporal wasting, thenar wasting), BMI. TB classically produces cachexia — loss of both fat and muscle from chronic high-cytokine state.
- Pallor: Anaemia of chronic disease is universal in active TB — examine conjunctivae for pallor.
- Fever: Record temperature formally; the diurnal pattern (temperature peaks in late afternoon/evening) is characteristic.
- Respiratory rate: Count for a full minute while pretending to take the pulse — an elevated rate (>20/min) indicates significant respiratory compromise.
- Lymphadenopathy: Palpate the cervical (anterior and posterior triangles), supraclavicular, axillary, and inguinal nodes. Any palpable firm or matted node should be characterised: size (in cm), consistency (firm, soft, fluctuant), tenderness, fixity to skin or deep structures, and presence of sinus formation or discharge.
- Clubbing: Present in chronic suppurative conditions — empyema, bronchiectasis — and occasionally in advanced TB. Examine all fingers systematically.
- Jaundice: Hepatotoxicity is a major concern during ATT; baseline jaundice assessment is important before starting isoniazid, rifampicin, and pyrazinamide.
- Oral cavity: Angular stomatitis and glossitis suggest nutritional deficiency; oral candidiasis suggests immunosuppression and prompts HIV testing.
- Neck stiffness: If meningeal signs are clinically suspected, test for nuchal rigidity, Kernig's sign, and Brudzinski's sign in this phase of the general examination.
B. Examination of the Chest and Lungs:
Proceed in the classical sequence: inspection → palpation → percussion → auscultation. Examine anteriorly and posteriorly; never omit the posterior chest in a TB examination.
Inspection:
- Respiratory pattern: Rate, depth, symmetry of chest expansion, use of accessory muscles, intercostal retraction.
- Shape of chest: Bilateral apical flattening (loss of infraclavicular fullness) is an important early sign of post-primary TB — look for asymmetry of the infraclavicular fossae. A scaphoid chest (flat or concave anteriorly) can reflect old TB with fibrosis and volume loss.
- Tracheal position: Deviation of the tracheal ring from the midline — toward the affected side in collapse/fibrosis, away in effusion.
- Spinal curvature: Gibbus deformity (sharp angular kyphosis, usually thoracolumbar) = Pott's disease until proven otherwise.
Palpation:
- Tracheal deviation: Palpate with the index finger in the tracheal notch above the manubrium; confirm the degree and direction of deviation.
- Mediastinal shift: Check apex beat position — displaced with mediastinal shift.
- Chest expansion: Place both thumbs on the spine posteriorly; assess symmetry of expansion — reduced on the affected side in consolidation, effusion, collapse, or extensive fibrosis.
- Tactile vocal fremitus (TVF): Ask the patient to say "ninety-nine" while palpating symmetrical points of the chest wall. TVF is increased over consolidated lung (better conduction of sound through solid tissue) and decreased/absent over an effusion (fluid dampens transmission) or collapse.
Percussion:
- Use the pleximeter technique — middle finger of non-dominant hand placed firmly on the chest wall, struck by the middle finger of the dominant hand with a crisp wrist-flick.
- Percuss systematically: begin at the apices (supraclavicular and infraclavicular areas), proceed down each intercostal space, comparing left to right at each level. Always percuss posteriorly from the upper to lower zones.
- Dullness over a lung zone = consolidation (TB pneumonia), thickened pleura, or collapse.
- Stony dullness = pleural effusion — the dullest note in clinical medicine, with a characteristic "wooden" quality.
- Kronig's isthmus (the resonant band over the upper trapezius): dullness here indicates upper-lobe disease — highly significant in post-primary TB.
Auscultation:
- Bronchial breathing over a consolidated zone (coarse, blowing character, equal inspiration and expiration, with a gap between the two): indicates open consolidation — TB pneumonia, lobar pneumonia. Associated with increased vocal resonance and whispered pectoriloquy.
- Diminished/absent breath sounds with stony dullness = effusion. Auscultate above the level of effusion for bronchial breathing (from compressed lung at the effusion margin — Ewart's sign in pericardial effusion; similar mechanism here).
- Amphoric breathing over a large cavity (hollow, cavernous sound) — a rare but dramatic sign in large TB cavities.
- Post-tussive crepitations (crepitations that appear or worsen after a short cough) are highly specific for TB cavitation — the cough displaces secretions, unmasking the crackling of moist secretion in the cavity wall.
- Rhonchi (wheeze): may be present if TB causes endobronchial disease or if the patient is also a smoker with COPD.
C. Examination of the Lymphatic System:
Palpate each lymph node group systematically and describe each abnormal node precisely. For TB lymphadenitis:
- Cervical nodes are the most commonly involved. Palpate the submental, submandibular, anterior cervical chain, posterior cervical triangle, and supraclavicular fossae.
- Cold abscess formation: TB lymph nodes become fluctuant ("cold" because there is no warmth or erythema) and may develop a pointing abscess that discharges through the skin forming a collar-stud abscess (a dumbbell-shaped abscess with upper and lower collections connected through a defect in the deep fascia).
- Matting: Nodes that are fused together (matted) by periadenitis are characteristic of TB and sarcoidosis; pyogenic adenitis tends to be tender and not matted.
D. Relevant CNS Examination:
In any patient with: prolonged fever, headache, confusion, vomiting, altered sensorium, focal neurological deficits, or visual disturbance, perform a targeted neurological examination to exclude TB meningitis or tuberculoma. Key elements:
- Level of consciousness: Glasgow Coma Scale (GCS).
- Meningeal signs: Neck stiffness (resistance to passive flexion), Kernig's sign (inability to fully extend the knee with the hip at 90° flexion due to meningeal irritation), Brudzinski's sign (involuntary knee flexion when the neck is passively flexed).
- Cranial nerve examination: CN II (optic disc oedema = raised intracranial pressure — fundoscopy mandatory); CN III, IV, VI (ocular motor palsies from basal meningitis); CN VII (facial nerve palsy from tuberculous parotitis or basal meningitis).
- Fundoscopy: Look for choroidal tubercles — 1–2 mm discrete yellowish/grey lesions in the choroid visible on fundoscopy — pathognomonic of miliary TB (present in 10–20% of miliary TB cases; absence does not exclude miliary TB).
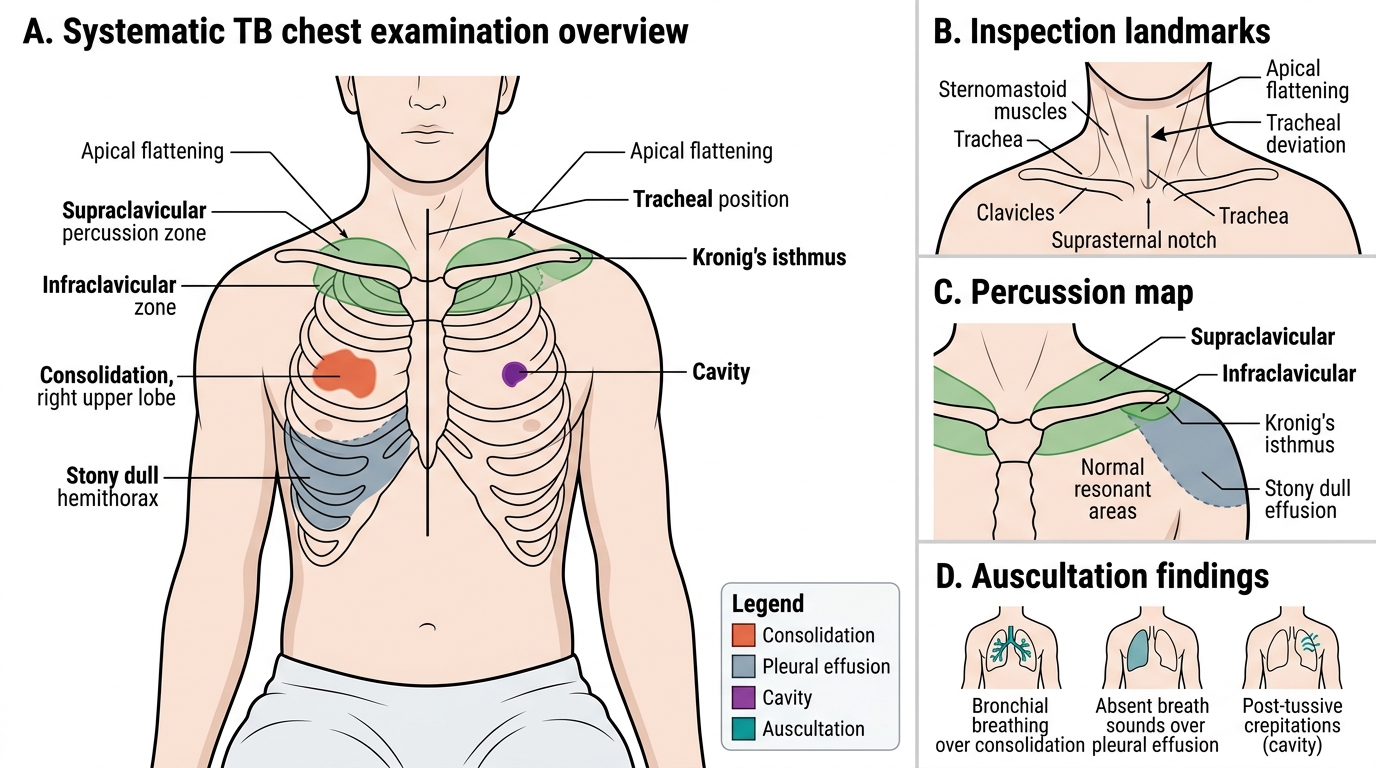
Systematic Chest Examination in Pulmonary Tuberculosis
Technique of Examination — Step-by-Step Procedure for TB Assessment
Knowing what to look for and knowing how to elicit it are two different skills. This section provides the procedural technique for each element of the TB clinical examination — the exact sequence of steps, hand positions, patient instructions, and discriminating manoeuvres that translate anatomical knowledge into reproducible clinical findings. Technique matters because examinations performed incorrectly generate false-negative and false-positive findings with equal reliability; a student who palpates lymph nodes with fingertips rather than the flat of the fingers will miss 30% of palpable nodes; a student who percusses without a firm pleximeter contact will report dullness over normal lung. The clinical accuracy of a TB examination is therefore a function of technique, not merely of knowledge.
Technique: Lymph node palpation:
Position the patient seated or supine with the neck slightly flexed toward the side being examined (relaxes sternomastoid, allowing posterior triangle access). Use the flat of 2–4 fingers, not fingertips. Palpate in a systematic sequence: submental → submandibular → anterior cervical chain (along sternomastoid) → posterior cervical triangle → supraclavicular fossae (from behind, hook fingers over the clavicle) → axillae (with arm slightly abducted, advance fingers into the axillary dome). For each palpable node, report: maximum diameter in cm, consistency, tenderness (present/absent), fixity (mobile vs matted vs fixed to skin or deep structures), overlying skin changes (sinus, discharge).
Technique: Tracheal palpation:
Stand facing the patient. Place the index finger of the right hand gently in the suprasternal notch, between the two heads of sternomastoid. Assess whether the trachea touches the finger centrally (midline) or is displaced. Even mild deviation (1 cm) is clinically significant. Warn the patient beforehand — this palpation is mildly uncomfortable.
Technique: Chest expansion:
Posterior technique: wrap both hands around the lower chest, thumbs pointing toward each other and resting lightly on the spine (not pressing). Ask the patient to take a deep breath. The thumbs should move apart equally — asymmetric movement indicates reduced expansion on the restricted side. Anterior technique (less sensitive): place hands on the anterior chest with thumbs meeting at the midline.
Technique: Percussion of the apices (critical in TB):
Percuss the supraclavicular fossae by placing the pleximeter finger in the fossa, parallel to the clavicle. Percuss with 2–3 crisp wrist-flick strikes, comparing both sides. Next, percuss Kronig's isthmus — the band over the trapezius muscle, from the lateral neck to the shoulder. In normal lung, this area is resonant; dullness here indicates upper-lobe disease. This is the most specific percussion area for apical TB and should never be omitted.
Technique: Eliciting post-tussive crepitations:
Auscultate the right and left upper zones both anteriorly (infraclavicular) and posteriorly (suprascapular area) with the stethoscope's diaphragm. First listen at rest. Then ask the patient to produce two sharp coughs. Immediately re-apply the stethoscope to the same zone. Crepitations appearing or increasing sharply after the cough = post-tussive crepitations. This sign requires active elicitation — it will not be present at rest in many TB cavities.
Technique: Meningeal signs:
For neck stiffness: with the patient supine, gently support the head and attempt passive neck flexion (chin toward chest). Resistance before the chin reaches the chest = nuchal rigidity. For Kernig's sign: flex the hip to 90°, then attempt to extend the knee. Pain and muscle resistance before full extension = positive Kernig. For Brudzinski's sign: as you flex the neck, watch the hips and knees — spontaneous flexion = positive Brudzinski.
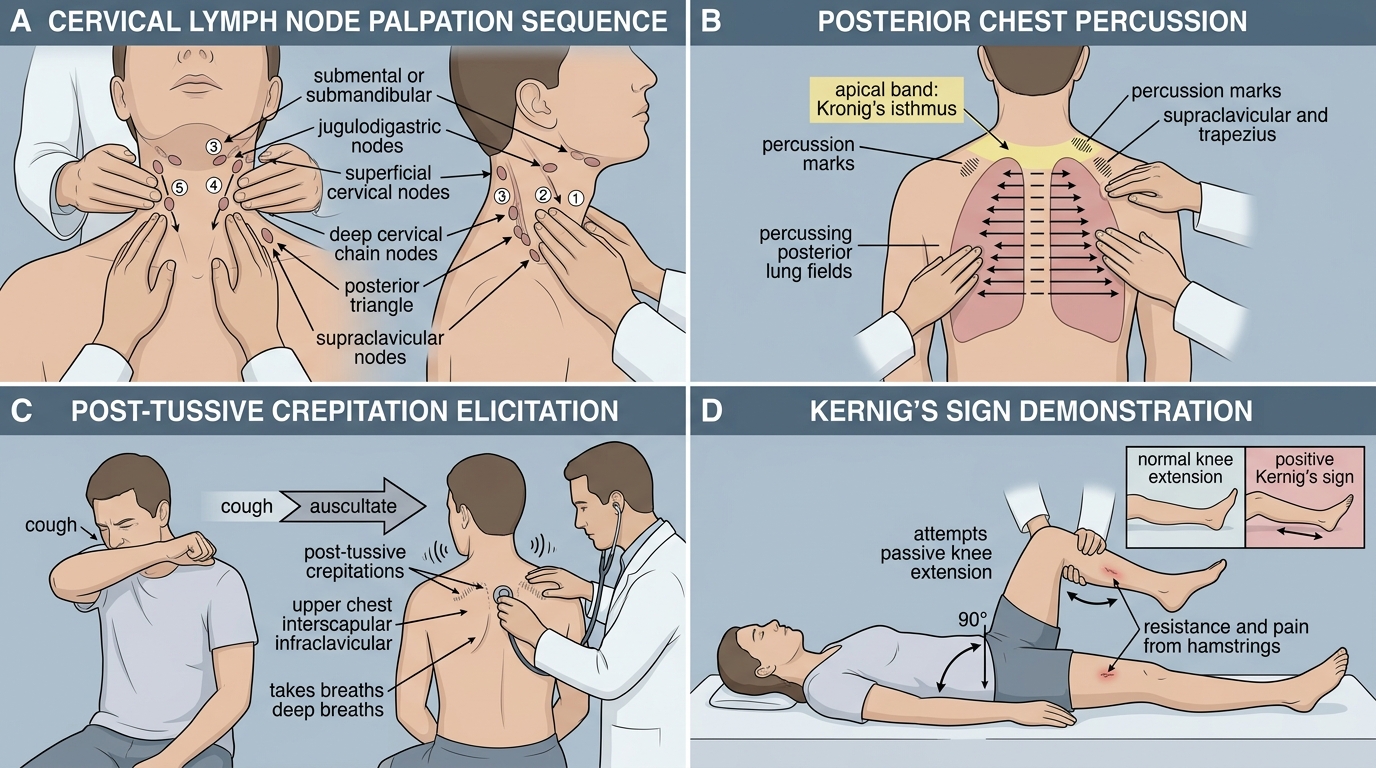
Step-by-Step TB Clinical Examination Techniques
SELF-CHECK
On percussion of a patient's right lower chest, you elicit a stony dull note from the right 5th intercostal space downward to the base. Tactile vocal fremitus is absent in the same area. Breath sounds are diminished. What is the most likely underlying pathological process?
A. Right lower lobe consolidation (TB pneumonia)
B. Right-sided pleural effusion
C. Right lower lobe collapse
D. Right-sided pneumothorax
Reveal Answer
Answer: B. Right-sided pleural effusion
The triad of stony dullness + absent TVF + absent/diminished breath sounds is the classic clinical signature of a pleural effusion. Stony dullness (the dullest percussion note in clinical medicine) is caused by fluid attenuating the percussion wave; absent TVF reflects fluid blocking sound conduction from the underlying lung to the chest wall; diminished breath sounds result from the fluid barrier. Consolidation gives dull (not stony dull) percussion with increased TVF and bronchial breathing. Collapse gives dullness with absent TVF and reduced sounds, but without the stony quality. Pneumothorax gives hyper-resonance and absent sounds. Pleural TB (typically an exudative unilateral effusion with elevated ADA >40 IU/L in pleural fluid) is a common cause of right-sided exudative effusion in India.