Page 6 of 18
IM27.{5-6,8} | Tuberculosis Clinical Evaluation — SDL Guide (Part 2)
Generating a Prioritised Differential Diagnosis in Presumptive TB
A differential diagnosis is not a random list of conditions — it is a ranked probability distribution built from the clinical data acquired during the history and examination. The clinical skill of differential diagnosis generation (IM27.8) requires the physician to synthesise age, demographics, epidemiological risk factors, duration and pattern of symptoms, physical examination findings, and known disease prevalence into a hierarchy: most likely first, dangerous alternatives that must be excluded, and conditions whose management would fundamentally differ.
The clinical approach proceeds in three steps: first, construct the working diagnosis (the single most probable explanation for the entire clinical picture), supported by the evidence from the history and examination; second, generate alternative diagnoses (other conditions that could plausibly explain the same constellation, or conditions where missing the diagnosis would be harmful); and third, identify the distinguishing features that investigations will need to confirm or refute.
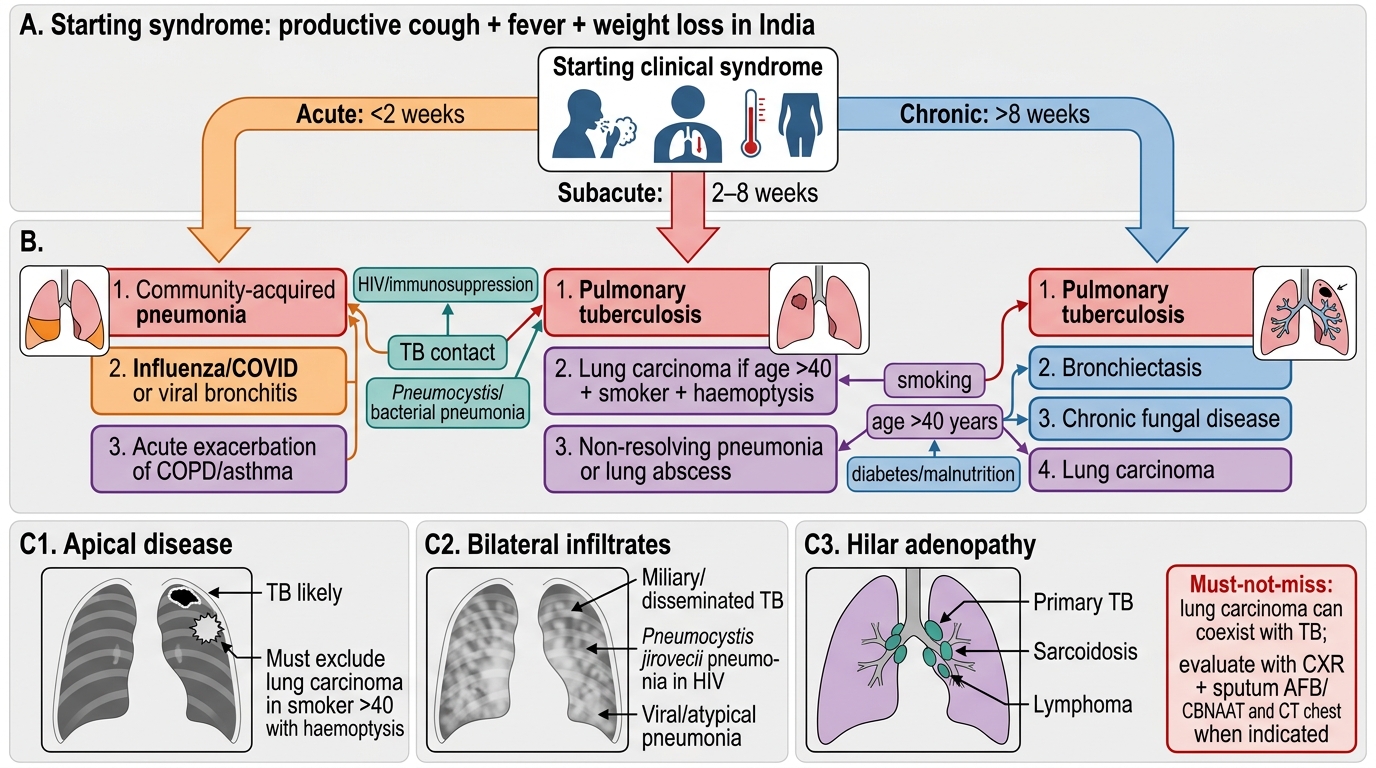
The master differential for the patient with productive cough + fever + weight loss in India:
Highest probability in the Indian context:
1. Pulmonary tuberculosis (drug-sensitive) — most likely given: ≥2–3 weeks cough, evening fever, night sweats, weight loss, and risk factors (contact, prior TB, diabetes, HIV, crowded living). Upper lobe signs on examination (apical dullness, post-tussive crepitations) massively increase probability.
2. Pulmonary TB with drug resistance (MDR/RR-TB) — same clinical picture, but suspect if: prior TB treatment (especially incomplete), treatment failure, or exposure to known drug-resistant contact.
Must-exclude alternatives:
3. Community-acquired pneumonia (CAP) — acute onset (<7–10 days), higher fever, productive purulent sputum, rigors, responds to antibiotics. Lobar consolidation on CXR. Distinguish: acuity of onset (TB is subacute by definition), productive character (pyogenic vs mucoid), response to antibiotics (CAP responds; TB does not).
4. Lung malignancy (squamous cell carcinoma, adenocarcinoma) — progressive weight loss, haemoptysis, and smoking history in an older patient (>40 years, male, heavy smoker). A mass on CXR rather than apical infiltrates. However, TB and lung cancer can co-exist (TB scar carcinoma). Must be excluded in any patient >40 with haemoptysis and asymmetric apical shadow on CXR.
5. HIV/AIDS with Pneumocystis jirovecii pneumonia (PCP) — bilateral perihilar infiltrates (not apical), progressive breathlessness more prominent than cough, CD4 typically <200, LDH elevated. Co-infection with TB is common.
6. Lymphoma — mediastinal widening on CXR, constitutional B symptoms (fever, night sweats, weight loss — identical to TB), lymphadenopathy. Distinguish by histology (lymph node biopsy, mediastinoscopy).
7. Fungal infections — histoplasmosis or cryptococcosis in immunocompromised patients; paracoccidioidomycosis in travellers from South America; not endemic in India, but cryptococcal meningitis in HIV patients mimics TB meningitis.
8. Sarcoidosis — bilateral hilar lymphadenopathy, non-caseating granulomas, usually no positive AFB, serum ACE elevated, typically young adult, non-toxic-looking. Distinguished from TB lymphadenitis histologically.
Context-specific alternatives (guide from history):
- In a patient with headache and meningism: bacterial meningitis (acute onset, CSF PMN-predominant) vs cryptococcal meningitis (India ink on CSF) vs TB meningitis (subacute, CSF lymphocytic, elevated ADA).
- In a patient with back pain: pyogenic vertebral osteomyelitis (Staphylococcus aureus — more acute, fever prominent, Brucella in animal handlers) vs Pott's disease (subacute, paravertebral cold abscess, disc space loss).
- In a patient with cervical lymphadenopathy: reactive lymphadenopathy (acute viral URTI — tender, bilateral, resolves in 2 weeks) vs TB lymphadenitis (firm, matted, >2 weeks, cold abscess formation) vs lymphoma (non-tender, rubbery, mediastinal involvement).
Constructing the documented differential:
In clinical documentation and oral presentation, the differential should be ranked with evidence cited for each entry. A well-structured differential for Sunita (the schoolteacher from the opening) would read:
1. Pulmonary TB (most likely): 3-week cough, evening fever, night sweats, 4 kg weight loss, household TB contact 2 years ago; upper lobe examination findings if present.
2. Atypical pneumonia (possible): 3-week cough with productive component, fever — distinguish by acuity, CXR pattern, antibiotic response.
3. Lung malignancy (must exclude): Progressive weight loss and haemoptysis; CXR is the discriminating investigation.
4. HIV-related pulmonary disease (consider): Bilateral infiltrates, CD4 not known — request HIV serology.
Differential Diagnosis of Productive Cough, Fever, and Weight Loss in India
SELF-CHECK
A 42-year-old male smoker presents with 5 weeks of productive cough, haemoptysis, and significant weight loss. He has no prior TB history and no known TB contacts. Examination shows dullness and decreased breath sounds at the right upper zone. What is the single MOST important diagnosis to rule out alongside TB?
A. Community-acquired pneumonia
B. Pleural effusion from congestive heart failure
C. Lung carcinoma
D. Sarcoidosis
Reveal Answer
Answer: C. Lung carcinoma
In a smoker aged >40 years with haemoptysis, weight loss, and a focal right upper zone opacity, lung carcinoma must be excluded — it is a 'must-not-miss' diagnosis. TB and lung cancer are not mutually exclusive (a TB scar can undergo malignant transformation — so-called scar carcinoma). The clinical profile (male, smoker, >40, haemoptysis, weight loss) increases the pre-test probability of malignancy to a level that cannot be dismissed. The approach: perform CXR and sputum for AFB smear/CBNAAT simultaneously with CT chest. If the CXR shows a spiculated mass rather than classic apical infiltrate/cavitation, malignancy moves to the top of the differential. Community-acquired pneumonia would present more acutely. Heart failure effusion would not explain productive cough or weight loss. Sarcoidosis is less likely in a male smoker of this age.
Applied Practice — Integrating Clinical Evaluation in the TB Encounter
Competency in TB clinical evaluation is not achieved by memorising signs — it is built through the deliberate integration of history, examination, and differential diagnosis reasoning into a coherent clinical encounter. The following applied framework describes how the skilled clinician organises the 30-minute TB evaluation, what documentation standards apply, and what the most common errors are at each step.
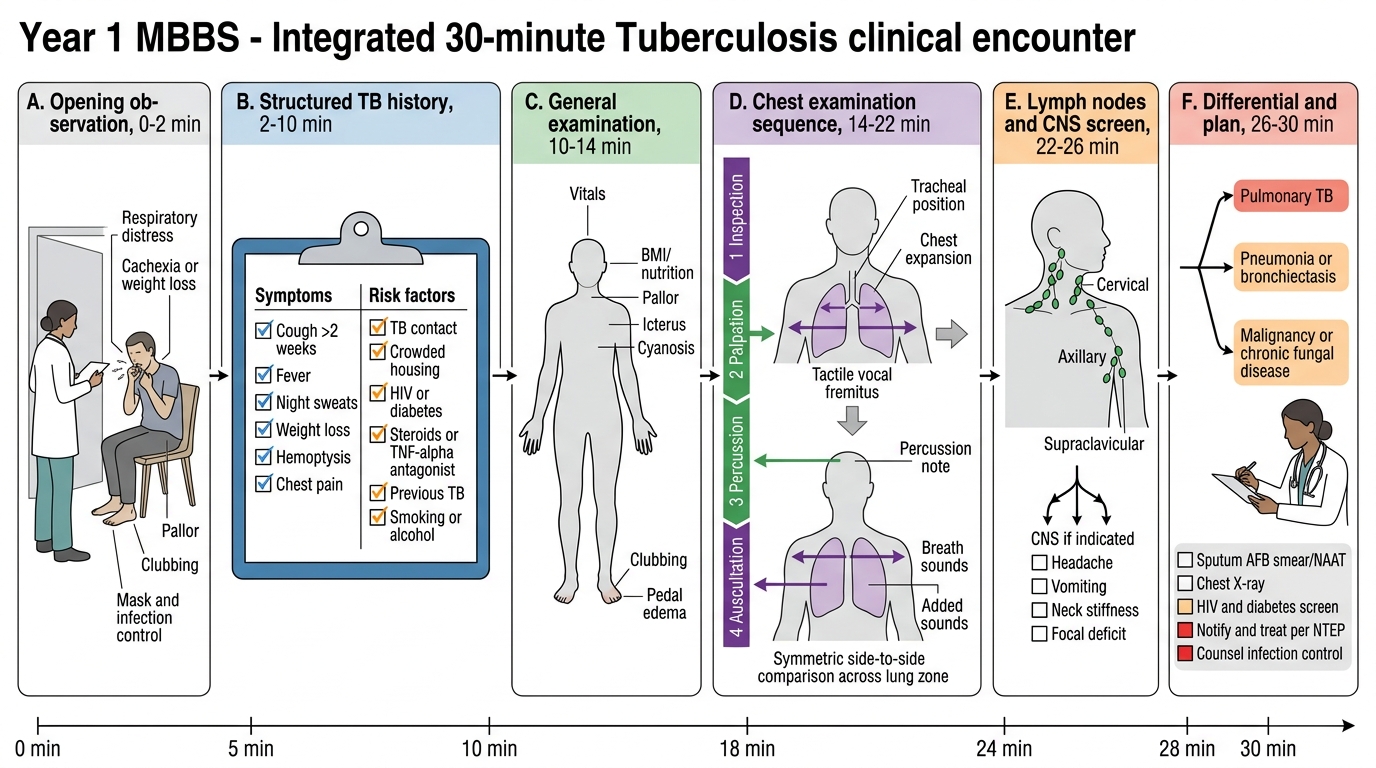
The integrated 30-minute TB clinical encounter:
Opening (2–3 minutes): Introduce, gain consent, ask the patient to describe their main complaint in their own words. Note the initial impression from across the room — respiratory rate, cough during the conversation, nutritional state, pallor. This passive observation begins the examination before you have touched the patient.
Structured history (10–12 minutes): Work through the symptom constellation (cough, fever, night sweats, weight loss, haemoptysis, breathlessness), then the risk factor assessment (contact, prior TB, HIV, DM, occupation, housing). Use direct questions for risk factors — patients frequently do not volunteer that a household member was treated for TB or that they are HIV-positive. Quantify: "How many weeks has the cough lasted? How much weight have you lost?"
General examination (5 minutes): Temperature, respiratory rate, BMI, pallor (conjunctivae), clubbing, lymphadenopathy (palpate all chains systematically), oral cavity, neck stiffness if indicated.
Chest examination (10 minutes): Full inspection → palpation (expansion, TVF) → percussion (anterior + posterior, including apices) → auscultation (anterior + posterior). Document each finding specifically, not as a vague global description.
Closing (2–3 minutes): Summarise the clinical findings and immediately formulate the differential diagnosis while still in front of the patient. Communicate the plan: "I need to arrange a chest X-ray and sputum test today."
Common errors in clinical TB evaluation:
- Omitting examination of the posterior chest (most TB cavities are in the upper lobes posteriorly — the supraclavicular area and posterior upper zones are the highest-yield examination sites for TB).
- Failing to palpate the cervical and supraclavicular lymph nodes — TB lymphadenitis is the most common form of extrapulmonary TB and is physically present on examination.
- Recording TVF as "normal" without testing — TVF must be elicited actively, not assumed.
- Attributing a 3-week cough to GORD or viral illness without systematic risk-factor assessment — in India, the default assumption for persistent cough must be TB until excluded.
- Missing meningeal signs because CNS examination is reserved for "neurology cases" — TB meningitis kills within days; it must be sought in any febrile TB patient with headache.
Documentation standards for the TB clinical evaluation: The NTEP treatment card (Nikshay) requires formal documentation of: presenting symptoms (duration and severity), contact history, HIV status, past TB history, examination findings including weight and temperature, and the working diagnosis with smear-positivity status. A clinical entry that omits these elements is an incomplete entry.
Integrated 30-Minute TB Clinical Encounter
Self-Assessment: Applying TB Clinical Evaluation Skills
The scenarios below test your ability to integrate the three clinical skills covered in this module — history-taking, examination, and differential diagnosis — into a coherent clinical action. For each case, apply the frameworks built in the preceding content blocks before reading the analysis.
Scenario A — Completing the risk-factor history: You are seeing a 35-year-old man with 4 weeks of cough and weight loss. He says he has no health problems and takes no medications. On direct questioning about contact history, he admits his brother-in-law was treated for TB "about 8 months ago" and that they share a small one-room house. He also mentions he was started on a medication for joint pain six months ago by a private specialist. What TWO pieces of information do you urgently need to clarify, and why?
Analysis: (1) What medication was prescribed for joint pain? If it is a TNF-α antagonist (etanercept, adalimumab, infliximab — increasingly used for rheumatoid arthritis in private practice in India), this is a powerful immunosuppressant that markedly elevates TB risk, and LTBI screening before starting it should have been performed. His TB risk is now very high. (2) Was the brother-in-law's TB drug-sensitive or drug-resistant? If the contact had MDR-TB, this patient is at risk for primary MDR-TB and will need DST results before treatment initiation. Both omissions from the initial history could have led to an incorrect treatment decision.
Scenario B — Interpreting examination findings: You examine a 22-year-old woman with 5 weeks of cough, fever, and weight loss. On posterior chest percussion, you find dullness at the right apex and an absence of Kronig's isthmus resonance on the right. Post-tussive crepitations are heard in the right upper zone. The rest of the chest is resonant with normal vesicular breath sounds. What is the localised pathology, and what is the most likely diagnosis given the clinical context?
Analysis: Dullness + absent Kronig's isthmus resonance on the right = right upper lobe disease (consolidation, thickening, or early fibrosis). Post-tussive crepitations in the right upper zone = highly specific for TB cavitation. Together these clinical signs constitute the classic examination picture of post-primary (reactivation) pulmonary TB. The differential at this point is narrowly TB vs lung carcinoma; age 22 and the absence of smoking history makes carcinoma far less likely, making TB the working diagnosis. Proceed to: sputum CBNAAT, CXR PA view.
Scenario C — Formulating the differential: A 48-year-old male auto-mechanic presents with 8 weeks of cough, weight loss, and bilateral cervical lymphadenopathy. He is a current smoker (30 pack-years). Examination shows matted cervical nodes bilaterally, no respiratory signs on chest examination, and a palpably enlarged liver. Chest X-ray shows bilateral hilar enlargement with no parenchymal infiltrates. What is the differential diagnosis, and which feature most distinguishes TB lymphadenitis from the most dangerous alternative?
Analysis: Differential: (1) TB (cervical + hilar adenopathy, systemic symptoms, Indian epidemiology); (2) Lymphoma (bilateral lymphadenopathy, hepatomegaly, mediastinal/hilar nodes, constitutional symptoms indistinguishable from TB — this is the must-exclude diagnosis); (3) Sarcoidosis (bilateral hilar adenopathy, typically young adults, non-caseating on biopsy). The most dangerous alternative is lymphoma — missing it delays potentially curative chemotherapy. The distinguishing feature is histology: TB lymph node biopsy shows caseating granuloma with AFB; lymphoma shows Reed-Sternberg cells (Hodgkin's) or lymphoid malignancy (NHL). FNAC of a cervical node is the correct next step, with simultaneous AFB smear/culture and histopathological examination.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
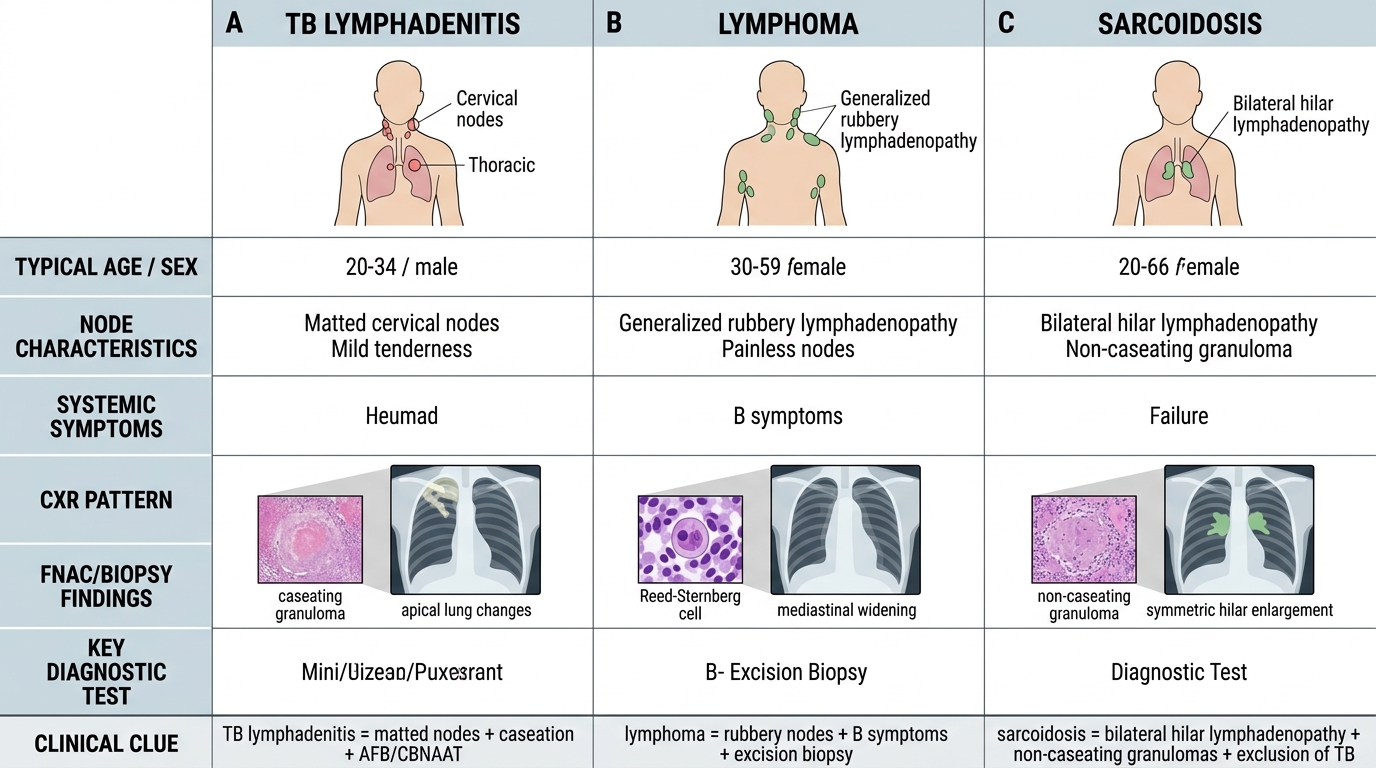
TB Lymphadenitis vs Lymphoma vs Sarcoidosis
SELF-CHECK
During auscultation of a patient's chest, you hear breath sounds that are louder than normal, with an equal inspiratory and expiratory component and a distinct pause between them, best heard over the right infraclavicular area. These breath sounds are most consistent with which underlying pathology?
A. Right upper lobe pleural effusion
B. Right upper lobe consolidation (e.g., TB pneumonia)
C. Right-sided pneumothorax
D. Normal right upper lobe vesicular breath sounds
Reveal Answer
Answer: B. Right upper lobe consolidation (e.g., TB pneumonia)
Bronchial breathing — louder, with equal inspiratory and expiratory phases and a distinctive gap between them — is heard when aeration is maintained but the lung is consolidated, producing enhanced sound transmission from the central airways to the chest wall. It is the auscultatory equivalent of an air bronchogram on CXR. The right infraclavicular area corresponds to the right upper lobe — a classic location for TB pneumonia and consolidation. Pleural effusion gives absent/diminished breath sounds (fluid blocks transmission). Pneumothorax gives absent breath sounds with absent TVF and hyper-resonance. Normal vesicular breathing is soft and predominantly inspiratory without a gap. The key associated findings in consolidation: dull (not stony dull) percussion, increased TVF, whispered pectoriloquy, and bronchophony.
CLINICAL PEARL
The single most commonly missed physical sign in TB clinical evaluation is post-tussive crepitations. Students routinely auscultate the lungs in a resting patient, hear nothing abnormal, and conclude the chest is clear. Ask the patient to cough twice, then immediately place the stethoscope over the upper lobe — crepitations that appear or increase sharply after the cough indicate secretions or fluid in a cavity that has been redistributed by the cough. This finding is considered highly specific for TB cavitation and should be sought in every patient with presumptive pulmonary TB, especially when the resting auscultation appears normal.
A second pearl for the differential diagnosis: in India, any patient with unexplained constitutional symptoms (fever, weight loss, night sweats) lasting more than 2 weeks must be considered to have TB until proven otherwise — this is the foundation of the NTEP four-symptom screen. The danger lies in assuming a non-TB cause (viral illness, functional) and not pursuing investigation. Lymphoma is the most dangerous alternative that mimics TB's constitutional symptoms; always ensure that lymphadenopathy is biopsied and not merely attributed to "reactive" causes in the absence of confirmed microbiological diagnosis.