Page 11 of 18
IM27.13-18 | Tuberculosis Treatment and National Program — SDL Guide
Learning Objectives
- Describe the pharmacology, indications, contraindications, and adverse effects of the four first-line anti-tuberculosis drugs (isoniazid, rifampicin, pyrazinamide, ethambutol)
- Prescribe the correct NTEP weight-band FDC regimen for drug-sensitive pulmonary TB and common extrapulmonary sites
- Recognise the clinical features, risk factors, and diagnostic approach for drug-resistant TB, and describe the current NTEP DR-TB treatment pathway
- Define the NTEP cure criteria for DS-TB and MDR-TB and identify the outcomes of treatment failure and lost-to-follow-up
- Describe the indications, agents, and duration for contact chemoprophylaxis under NTEP
- Explain the structure and five components of the DOTS strategy and the role of Ni-kshay notification
- Communicate the diagnosis, treatment plan, and infection control advice to a patient with TB in an empathetic and clear manner
INSTRUCTIONS
This module covers the treatment and programmatic management of tuberculosis under India's National Tuberculosis Elimination Programme (NTEP). By the end, you will be able to prescribe the correct daily FDC regimen by weight band, manage drug adverse reactions, recognise and initiate work-up for drug-resistant TB, apply contact chemoprophylaxis, and communicate the diagnosis and treatment plan to a patient with the empathy and clarity that adherence demands.
References
- NTEP Technical and Operational Guidelines for Tuberculosis Control in India 2019 (Revised), Ministry of Health and Family Welfare (guideline)
- WHO Global TB Report 2023 (guideline)
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 177 — Tuberculosis (textbook)
- API Textbook of Medicine, 10th ed., Section on Infectious Diseases — Tuberculosis (textbook)
- NACO/NTEP Guidelines for Management of TB-HIV Co-infection in India, 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Ravi, a 28-year-old daily-wage labourer in Chennai, is brought to the medicine OPD by his wife after two months of productive cough, evening fever, and weight loss of six kilograms. His sputum CBNAAT returns Mycobacterium tuberculosis detected, rifampicin sensitive. You write the first prescription: two tablets of HRZE fixed-dose combination (weight band 45–54 kg), daily, directly observed. Two weeks later his wife calls the NTEP helpline — she says Ravi is increasingly yellow, refusing to eat, and has dark urine. You suspect drug-induced hepatotoxicity from isoniazid or pyrazinamide. You stop all ATT, check liver enzymes (ALT >5× upper limit of normal), and sequentially reintroduce. Three months later a new patient arrives — Sunita, 32 years old, with CBNAAT positive, rifampicin resistant. She is frightened: she has heard that drug-resistant TB is untreatable. Your job is to counsel her, arrange an LPA (line probe assay), enrol her in the NTEP DR-TB pathway, and explain the regimen — all while maintaining her trust and adherence. TB is not merely a disease you diagnose and treat. It is a public health programme you manage, a pharmacological challenge you navigate, and a human conversation you must conduct with skill.
WHY THIS MATTERS
India carries the largest burden of TB in the world — approximately 28% of global TB cases and more than 75,000 cases of multidrug-resistant TB (MDR-TB) annually (WHO Global TB Report 2023). In this context, every physician graduating from an Indian medical college will encounter TB in general practice, chest medicine, internal medicine, paediatrics, and surgery — not as a rare imported case but as a routine, high-stakes patient interaction. The National Tuberculosis Elimination Programme (NTEP), formerly known as RNTCP, governs all TB care in India: standardised weight-band–based fixed-dose combination (FDC) regimens, mandatory Ni-kshay notification within 24 hours of diagnosis, patient adherence support through direct benefit transfer, and a dedicated DR-TB treatment pathway. A final-year MBBS student must be able to prescribe the correct NTEP regimen for drug-sensitive TB and DR-TB, recognise and manage adverse drug reactions, implement contact chemoprophylaxis, apply cure criteria, and educate patients and healthcare workers in a way that is empathetic, accurate, and nationally aligned.
RECALL
Before proceeding, activate your prior knowledge from earlier in this cluster. The causative organism is Mycobacterium tuberculosis, an obligate aerobic, slow-growing mycobacterium with a waxy cell wall rich in mycolic acids that confers intrinsic resistance to many antibiotics. The natural history of pulmonary TB involves a primary complex, latency in granulomata, and reactivation when host immunity wanes — a cycle shaped by HIV co-infection, diabetes mellitus, malnutrition, and overcrowding. Drug resistance in M. tuberculosis arises from spontaneous chromosomal mutations — not plasmid transfer — and is selected by inadequate therapy (incomplete courses, sub-therapeutic doses, poor quality drugs, or suboptimal drug combinations). You should also recall from microbiology that the CBNAAT/NAAT platform (Xpert MTB/RIF) simultaneously detects M. tuberculosis DNA and rifampicin resistance mutations in the rpoB gene; a positive rifampicin-resistance result from CBNAAT triggers the DR-TB pathway even before formal culture results are available. The pharmacological targets of the first-line agents — isoniazid, rifampicin, pyrazinamide, ethambutol — and their primary mechanisms of action should now guide your understanding of why combination therapy for a minimum duration is mandatory.
Clinical Context for Treatment Decisions
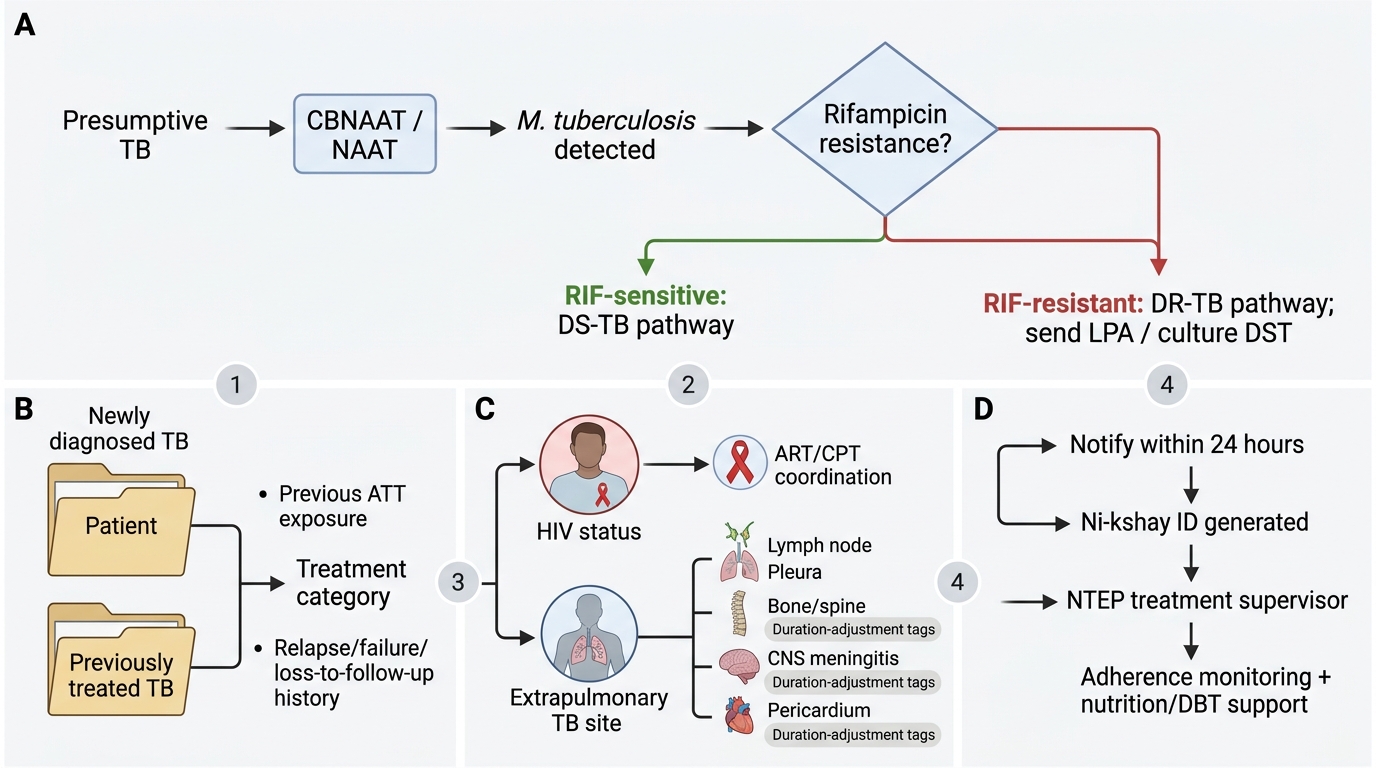
The decision to initiate anti-tuberculosis therapy (ATT) is driven by two converging clinical inputs: the bacteriological confirmation (or strong clinical probability where bacteriological confirmation is not yet available) and the patient's clinical category, which determines regimen selection, monitoring intensity, and the likelihood of drug resistance. Understanding this clinical entry point is the foundation for everything that follows in this module. Treatment is not a reflex after a positive test — it requires the clinician to categorise the patient correctly and to anticipate the challenges that will shape the therapeutic course: drug toxicity, adherence barriers, co-morbid conditions such as HIV and diabetes, and the risk of drug resistance.
Under NTEP, every newly diagnosed TB patient is classified according to bacteriological confirmation status and drug sensitivity status at the time of treatment initiation. The most important clinical categories are:
- Drug-sensitive TB (DS-TB): M. tuberculosis sensitive to at least rifampicin on CBNAAT or DST (drug susceptibility testing). This is the category for the standard 2HRZE + 4HRE regimen.
- Drug-resistant TB (DR-TB): Resistance to one or more first-line drugs. Subcategories include MDR-TB (resistant to both isoniazid and rifampicin), pre-XDR-TB (MDR-TB plus resistance to any fluoroquinolone), and XDR-TB (MDR-TB plus resistance to any fluoroquinolone and at least one of bedaquiline or linezolid — WHO 2021 revised definition).
- Previously treated TB: A patient who has received ≥1 month of ATT in the past. This history increases the prior probability of acquired drug resistance and mandates DST before re-treatment.
A critical clinical task at the time of presentation is the assessment of extrapulmonary involvement — tuberculous lymphadenitis, pleural TB, spinal TB (Pott's disease), CNS TB (tubercular meningitis), abdominal TB, and miliary TB all require the same bacteriological workup but may need longer treatment durations (CNS TB: 9–12 months; pericardial TB: 6 months with adjunctive steroids). The HIV status must be established at diagnosis in all TB patients — co-infected patients need ART and have specific drug interaction considerations, particularly with rifampicin.
Treatment Category Assignment in Tuberculosis
The Ni-kshay portal is the mandatory national web-based notification and patient management system. Every TB patient diagnosed in India — public or private sector — must be notified within 24 hours of diagnosis. Ni-kshay generates a unique patient identification number and triggers the patient support ecosystem: Ni-kshay Poshan Yojana (nutritional support transfer of ₹500/month to patients), direct benefit transfer for transport, and adherence monitoring by the designated NTEP treatment supervisor. Failure to notify is not merely a regulatory lapse — it deprives the patient of support and contributes to incomplete data for the national elimination programme.
Pharmacology of Anti-Tuberculosis Drugs
The pharmacological basis of ATT is inseparable from treatment rationale. The four first-line drugs — isoniazid (H), rifampicin (R), pyrazinamide (Z), and ethambutol (E) — are combined because each targets a different metabolic pathway in M. tuberculosis, acting at different stages of bacterial replication and in different physiological environments. This combination strategy is not arbitrary: it prevents the selection of pre-existing spontaneous mutants (which arise in any large bacterial population), accelerates sputum conversion, and allows a shorter, more reliably curative course than any single agent could achieve alone. Understanding each drug's mechanism, spectrum of activity, and adverse effect profile allows the clinician to recognise toxicity early, make informed substitutions when needed, and counsel patients effectively on what to expect.
Isoniazid (H) inhibits mycolic acid synthesis by targeting the InhA and KatG–mediated enoyl-ACP reductase pathway, which is unique to mycobacteria — this selectivity is the basis for isoniazid's potent bactericidal activity against actively replicating M. tuberculosis with a low toxic profile in humans. Isoniazid is a prodrug activated by the bacterial catalase-peroxidase enzyme KatG; mutations in katG or inhA are the predominant mechanisms of isoniazid resistance. Its key adverse effects are peripheral neuropathy (due to pyridoxine/vitamin B6 depletion — particularly important in pregnant patients, malnourished individuals, diabetics, and alcoholics — prevented by pyridoxine 10–25 mg/day supplementation), drug-induced liver injury (DILI) (especially in slow acetylators and those with pre-existing liver disease), and rarely, drug-induced lupus syndrome. Isoniazid is a potent inhibitor of CYP2C19, raising phenytoin and carbamazepine levels.
Rifampicin (R) inhibits bacterial DNA-dependent RNA polymerase (the rpoB-encoded beta subunit), blocking transcription initiation. It is the cornerstone sterilising agent — it kills both actively replicating bacilli and semi-dormant persisters within macrophages and necrotic foci, which is why its inclusion in the regimen is what allows the 6-month course to be reliably curative. Rifampicin is a potent inducer of cytochrome P450 enzymes (CYP3A4, CYP2C9) — this interaction critically lowers plasma levels of oral contraceptives, antiretroviral drugs (particularly protease inhibitors and NNRTIs), warfarin, corticosteroids, cyclosporine, and many other drugs. In HIV-co-infected patients on ART, efavirenz-based regimens (efavirenz 600 mg/day) are preferred because efavirenz retains therapeutic levels in the presence of rifampicin; nevirapine levels are reduced to sub-therapeutic concentrations and should NOT be used. Rifampicin causes harmless orange-red discolouration of urine, tears, sweat, and sputum — patients must be warned prospectively to avoid panic or premature discontinuation.
Pyrazinamide (Z) is active specifically in the acidic environment of caseating granulomata and within macrophage phagolysosomes, where the other drugs have limited penetration. It is converted by bacterial pyrazinamidase to pyrazinoic acid, which disrupts the mycobacterial membrane potential and interferes with coenzyme A metabolism. Pyrazinamide is responsible for the sterilising activity of the 2-month intensive phase — without it, the treatment duration would need to be extended. Adverse effects include hepatotoxicity (the most common serious adverse effect in combination therapy), hyperuricaemia (inhibits renal tubular secretion of urate — may precipitate gout in susceptible individuals), arthralgia (distinct from gout — a direct drug effect, managed with analgesics without stopping PZA), and photosensitivity.
Ethambutol (E) inhibits arabinosyl transferase, an enzyme involved in arabinogalactan synthesis in the mycobacterial cell wall. It is primarily bacteriostatic (not bactericidal) and its main role in combination therapy is to prevent the emergence of resistance to the other agents, particularly during the continuation phase. The critical adverse effect is optic neuritis — manifesting as reduced visual acuity, impaired colour vision (particularly red-green discrimination), and central scotomata — which is dose-dependent and largely reversible if caught early. Monthly visual acuity and colour vision testing is mandatory in patients on ethambutol. Ethambutol must be used with caution in patients with pre-existing optic nerve disease and should generally be avoided in children too young to reliably report visual symptoms.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
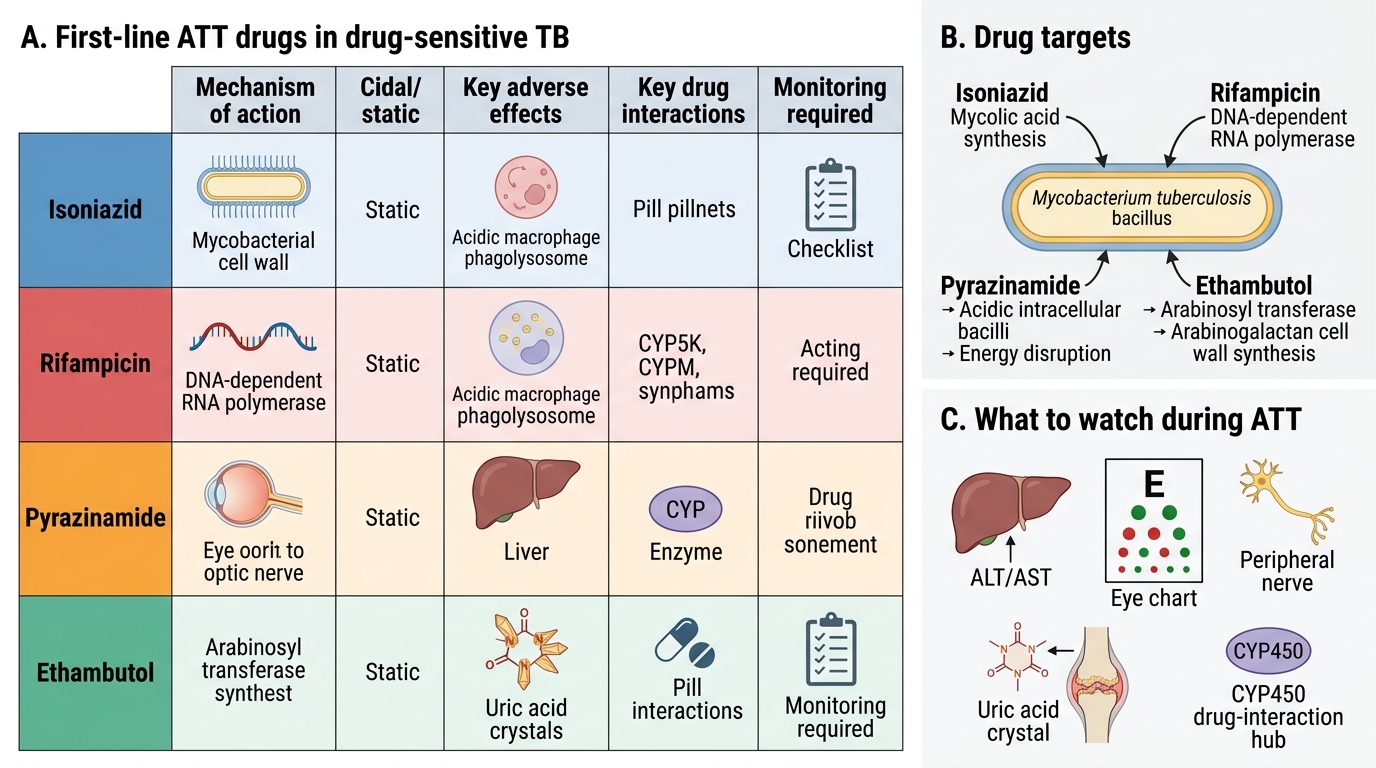
First-line ATT Drugs: Mechanisms, Toxicities, and Monitoring
Among second-line agents relevant to DR-TB, the most important classes include: fluoroquinolones (levofloxacin, moxifloxacin — DNA gyrase inhibition, key components of MDR-TB regimens; risk QT prolongation), injectable agents (amikacin, streptomycin — aminoglycosides targeting the 30S ribosomal subunit; risk ototoxicity and nephrotoxicity), bedaquiline (inhibits mycobacterial ATP synthase — first new anti-TB drug class in 40 years; key risk QT prolongation), linezolid (inhibits 50S ribosomal subunit protein synthesis; key risks myelosuppression and peripheral neuropathy), delamanid (nitroimidazole, inhibits mycolic acid synthesis), and clofazimine (membrane disruption, anti-inflammatory). The BPaL regimen (Bedaquiline + Pretomanid + Linezolid) has transformed outcomes in XDR-TB and treatment-intolerant/non-responsive MDR-TB.
SELF-CHECK
A 35-year-old patient newly diagnosed with pulmonary DS-TB is started on NTEP first-line FDC therapy. Three weeks later she reports yellow eyes, nausea, and dark urine. Liver enzymes show ALT 8× upper limit of normal. Which drug is most likely responsible and what is the FIRST step?
A. Ethambutol — stop ethambutol and continue the other three drugs
B. Rifampicin — switch to rifabutin as it is less hepatotoxic
C. Isoniazid or pyrazinamide — stop ALL four ATT drugs immediately and monitor LFTs
D. Isoniazid only — continue rifampicin, pyrazinamide, and ethambutol at the same doses
Reveal Answer
Answer: C. Isoniazid or pyrazinamide — stop ALL four ATT drugs immediately and monitor LFTs
Drug-induced liver injury (DILI) with ALT >5× ULN during ATT requires stopping ALL first-line drugs (isoniazid, rifampicin, pyrazinamide are all potentially hepatotoxic; ethambutol is generally not). The protocol is to stop all ATT, allow liver enzymes to normalise, then sequentially reintroduce: rifampicin first (least likely sole cause at standard doses), then isoniazid, then pyrazinamide — with LFT monitoring between each reintroduction. If LFTs rise on re-challenge with a specific drug, that drug is implicated and should be permanently excluded. Rifabutin substitution is relevant for rifampicin-induced drug interactions (e.g., HIV ART), not for DILI management.
NTEP Drug-Sensitive TB Regimen
The current NTEP regimen for drug-sensitive pulmonary and extrapulmonary TB (excluding CNS TB and miliary TB) is the daily, weight-band–based, fixed-dose combination (FDC) regimen: 2HRZE + 4HRE. This means an intensive phase of two months using all four drugs (isoniazid, rifampicin, pyrazinamide, ethambutol combined in a single tablet) followed by a continuation phase of four months using three drugs (isoniazid, rifampicin, ethambutol combined). The regimen is taken daily — the previously used thrice-weekly intermittent regimen under RNTCP has been completely discontinued by NTEP; it must not be prescribed. All doses are administered under direct observation by a trained NTEP treatment supporter (the DOTS strategy), though the 2019 NTEP operational guidelines now permit video-observed treatment (VOT) where feasible as an alternative to in-person observation.
The single most important practical application is weight-band dosing. FDC tablets are formulated in two strengths to ensure appropriate drug exposures across the weight range, since underdosing (particularly of isoniazid and rifampicin) promotes resistance selection. The current NTEP weight bands are:
| Weight band | Intensive phase tablets (HRZE FDC) | Continuation phase tablets (HRE FDC) |
|---|---|---|
| <55 kg | 3 tablets HRZE daily | 3 tablets HRE daily |
| 55–69 kg | 4 tablets HRZE daily | 4 tablets HRE daily |
| ≥70 kg | 5 tablets HRZE daily | 5 tablets HRE daily |
Patients should take FDC tablets on an empty stomach (30–60 minutes before a meal) to maximise rifampicin absorption, which is reduced by food. However, if gastric intolerance is a problem, the tablets may be taken with a light meal. Pyridoxine 10–25 mg/day should be co-prescribed for all patients to prevent isoniazid-induced peripheral neuropathy — this is especially important in pregnant patients, malnourished individuals, diabetics, the elderly, and alcoholics.
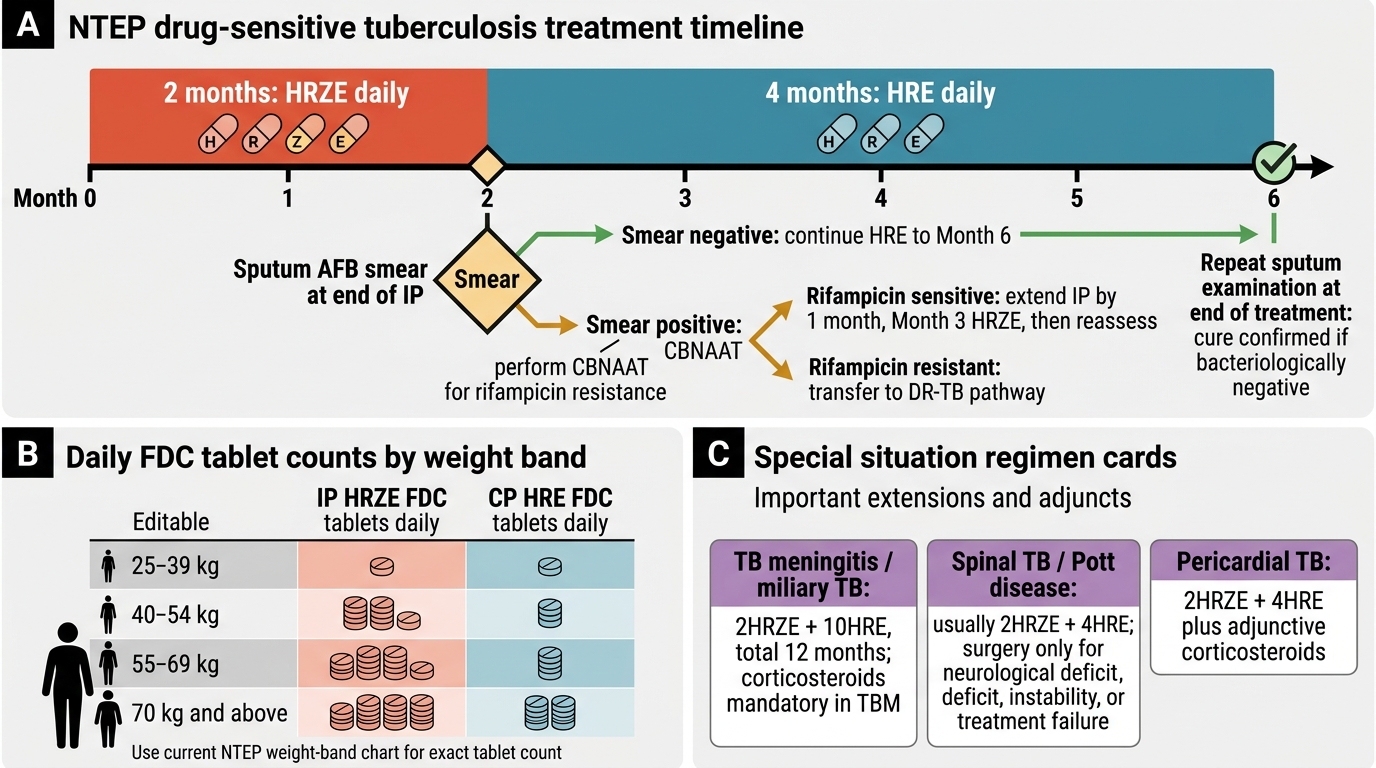
NTEP DS-TB Treatment Timeline and Month 2 Decision Point
A sputum AFB smear must be performed at the end of the intensive phase (month 2). If the smear is still positive at month 2, a CBNAAT is performed to check for rifampicin resistance (since smear positivity at month 2 is a risk factor for DR-TB). If CBNAAT confirms rifampicin sensitivity, the patient is an extended intensive phase case — the intensive phase is extended by one more month (month 3 HRZE), followed by reassessment. If CBNAAT detects rifampicin resistance, the patient is transferred to the DR-TB pathway. Sputum examination is then repeated at end of treatment (month 6) to confirm cure.
Special situations:
- Tubercular meningitis (TBM) and miliary TB: Extended regimen of 2HRZE + 10HRE (total 12 months); high-dose corticosteroids (dexamethasone or prednisolone) are mandatory as adjunctive therapy in TBM to reduce mortality and neurological sequelae; ethambutol has poor CNS penetration, and some guidelines substitute ethionamide or streptomycin for E in TBM.
- Spinal TB (Pott's disease): 2HRZE + 4HRE is standard; surgical decompression only for progressive neurological deficit, spinal instability, or failure of medical therapy.
- Pericardial TB: 2HRZE + 4HRE plus adjunctive corticosteroids to reduce constrictive pericarditis risk.
- Renal TB: Avoid aminoglycosides (nephrotoxic); adjust doses for eGFR; pyrazinamide requires caution in severe renal impairment.
- Pregnancy: 2HRZ + 4HR is standard (ethambutol can be included; streptomycin is contraindicated — ototoxic to the fetus); pyridoxine supplementation essential; breastfeeding is permitted.
SELF-CHECK
A 48-year-old man weighing 60 kg is newly diagnosed with pulmonary DS-TB (sputum CBNAAT positive, rifampicin sensitive). What is the correct NTEP regimen and number of FDC tablets per day?
A. 2HRZE + 4HR; 4 tablets of HRZE FDC daily in intensive phase; 3 tablets HRE daily in continuation phase
B. 2HRZE + 4HRE; 4 tablets of HRZE FDC daily in intensive phase; 4 tablets HRE daily in continuation phase
C. 2HRZE + 4HRE; 3 tablets of HRZE FDC daily in intensive phase; 3 tablets HRE daily in continuation phase
D. 2HRZ + 4HR; 4 tablets of HRZE FDC daily in intensive phase; no ethambutol in continuation phase
Reveal Answer
Answer: B. 2HRZE + 4HRE; 4 tablets of HRZE FDC daily in intensive phase; 4 tablets HRE daily in continuation phase
The correct current NTEP DS-TB regimen is 2HRZE + 4HRE (not 2HRZ+4HR). For a 60 kg patient (weight band 55–69 kg), the dose is 4 tablets of the HRZE FDC daily in the intensive phase and 4 tablets of the HRE FDC daily in the continuation phase. Option A incorrectly omits ethambutol from the continuation phase (the current NTEP regimen retains E in the continuation phase as HRE). Option C uses the <55 kg dose (3 tablets). Option D uses the older 2HRZ+4HR regimen without ethambutol.