Page 12 of 18
IM27.13-18 | Tuberculosis Treatment and National Program — SDL Guide (Part 2)
Drug-Resistant TB: Recognition, Regimens, and Cure Criteria
Drug-resistant tuberculosis (DR-TB) encompasses a spectrum of resistance patterns that require fundamentally different, longer, and more toxic treatment regimens than drug-sensitive TB. Recognising the features that should trigger a DR-TB work-up is a core clinical competency; delaying DR-TB diagnosis by treating empirically with standard DS-TB drugs drives further resistance selection and worsens outcomes.
The clinical features and risk factors that should prompt DR-TB evaluation are: (1) prior ATT treatment of ≥1 month (the most important risk factor — previously treated patients have a 5- to 10-fold higher rate of MDR-TB than new cases); (2) close contact with a confirmed MDR-TB case; (3) failure of standard treatment (sputum smear positive at month 5 or later); (4) default (lost to follow-up for ≥2 months) followed by return with active disease; (5) HIV co-infection with poor treatment response. In any of these situations, CBNAAT is the first-line investigation; if rifampicin resistance is detected, a Line Probe Assay (LPA) is sent for rapid detection of mutations in rpoB, katG, inhA, and fluoroquinolone resistance genes (gyrA, gyrB).
MDR-TB (resistant to both isoniazid and rifampicin, with or without resistance to other drugs) is treated with a standardised shorter MDR-TB regimen under NTEP, now based on the WHO 2022 operational research programme. The current NTEP MDR-TB regimen consists of:
- Bedaquiline (B), levofloxacin (Lfx), linezolid (Lzd), clofazimine (Cfz), and cycloserine (Cs) — this 5-drug regimen (BPaLCS or BLLfxCfzCs variant) for a duration of 18–20 months depending on culture conversion. Injection-based regimens (containing amikacin/kanamycin) are now largely replaced by the all-oral regimens.
- BPaL regimen (Bedaquiline + Pretomanid + Linezolid): A 26-week (6-month) regimen for treatment of XDR-TB and treatment-intolerant or non-responsive MDR-TB — a paradigm shift in outcomes with WHO 2022 endorsement. India has begun implementing BPaL under programmatic conditions.
Critical ADR monitoring in DR-TB regimens:
- Bedaquiline: QT prolongation — baseline and monthly ECG mandatory. Drug interaction with moxifloxacin (additive QT effect — avoid the combination). Hepatotoxicity.
- Linezolid: Myelosuppression (CBC monthly), peripheral neuropathy, optic neuritis — monthly blood counts and ophthalmological review.
- Fluoroquinolones (levofloxacin, moxifloxacin): QT prolongation, tendinopathy (rare), photosensitivity.
- Cycloserine: Neuropsychiatric adverse effects (depression, psychosis, seizures) — pyridoxine 200 mg/day co-prescribed; contraindicated in established epilepsy without specialist input.
- Clofazimine: Skin and conjunctival hyperpigmentation (reversible over months to years after stopping), ichthyosis.
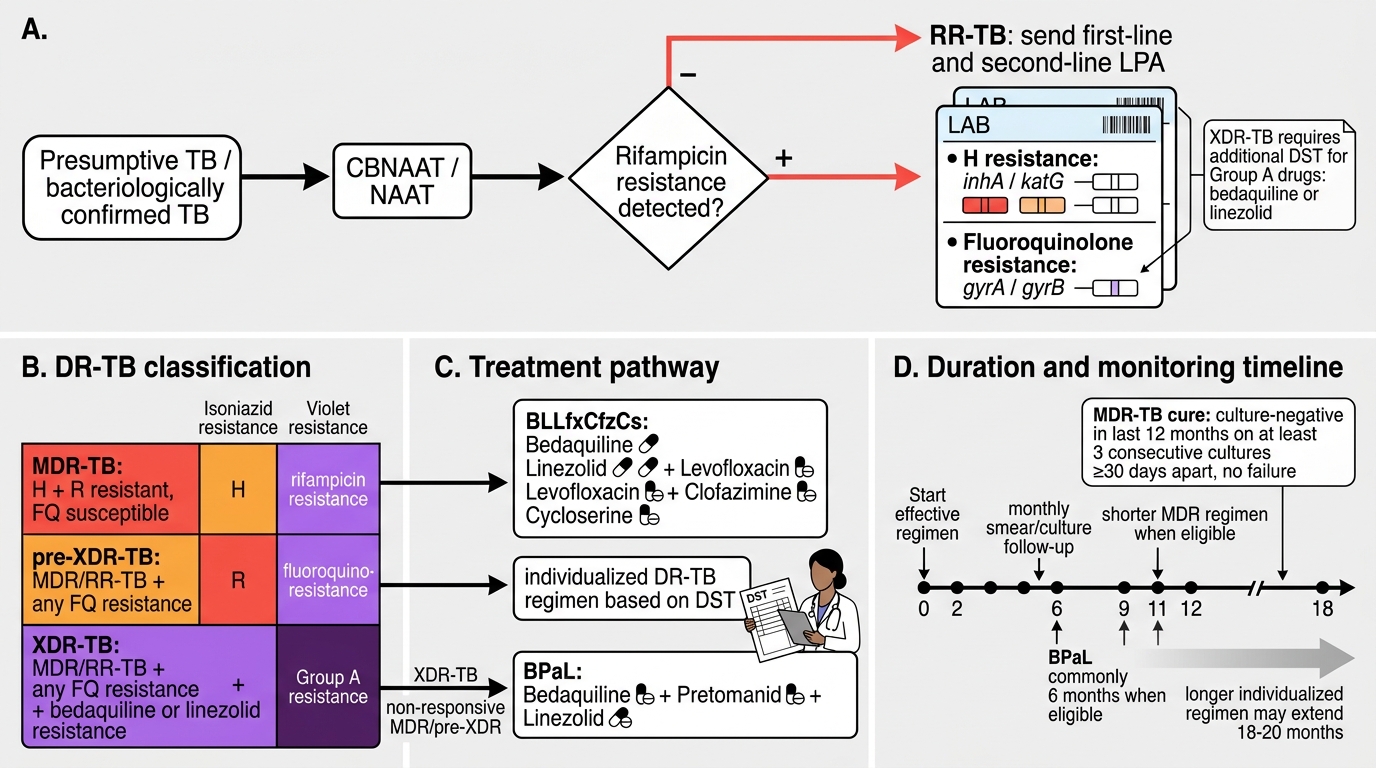
DR-TB Classification and Treatment Pathway
Cure criteria under NTEP are defined as follows:
- DS-TB cure: A bacteriologically confirmed patient who completes treatment and has negative sputum smear results at the end of the intensive phase and at end of treatment (month 6). A patient who completes treatment but has no bacteriological evidence of failure (smear not done) is classified as treatment completed, which is a distinct outcome.
- MDR-TB cure: Culture-negative in the last 12 months of treatment on at least 3 consecutive occasions taken ≥30 days apart, with no evidence of failure.
- Treatment failure (DS-TB): Sputum smear positive at month 5 or later during treatment. This mandates CBNAAT and DST; the patient is reclassified as DR-TB if resistance is detected.
- Lost to follow-up (LTFU): Interrupted treatment for ≥2 consecutive months. LTFU in MDR-TB is a particularly serious outcome — patients returning after LTFU from DR-TB treatment require fresh DST before re-treatment, since resistance amplification may have occurred.
Contact screening and chemoprophylaxis:
All household contacts and close contacts of index TB cases must be evaluated. The NTEP algorithm for contact management is:
1. All contacts: symptom screen (cough >2 weeks, fever, weight loss, night sweats, haemoptysis). Symptomatic contacts → chest X-ray → sputum examination if X-ray abnormal or symptoms persist.
2. Children <5 years who are household contacts of DS-TB cases and who have no active TB after evaluation: isoniazid preventive therapy (IPT) — isoniazid 10 mg/kg/day (max 300 mg/day) for 6 months. This is the standard paediatric contact chemoprophylaxis under NTEP.
3. PLHIV (people living with HIV) regardless of age who are contacts of TB cases and who screen negative for active TB: 6H (isoniazid preventive therapy for 6 months) is recommended by NACO/NTEP for all PLHIV without active TB in India — not just contacts — as part of the routine HIV care package.
4. Healthcare workers (HCWs) with occupational TB exposure: annual TB symptom screening, TST/IGRA testing for new converters, and IPT for those with latent TB infection who have not previously received preventive therapy. HCWs are a priority population under TB infection control guidelines.
Infection control in healthcare settings requires administrative controls (prompt isolation of infectious TB patients, early diagnosis, adequate room ventilation), environmental controls (natural or mechanical ventilation, UV germicidal irradiation), and respiratory protection (N95 respirators for HCWs in high-risk settings).
SELF-CHECK
A 4-year-old child is the household contact of her father, who was recently diagnosed with pulmonary DS-TB (sputum smear positive). The child undergoes a thorough evaluation — chest X-ray is normal, Mantoux test is 8 mm, and she has no symptoms of active TB. What is the appropriate NTEP management?
A. No intervention needed; she has a negative Mantoux test and is asymptomatic
B. Full 2HRZE + 4HRE treatment since she is a high-risk contact
C. Isoniazid 10 mg/kg/day (max 300 mg/day) for 6 months as chemoprophylaxis
D. Rifampicin + isoniazid for 3 months as preventive therapy
Reveal Answer
Answer: C. Isoniazid 10 mg/kg/day (max 300 mg/day) for 6 months as chemoprophylaxis
Under current NTEP guidelines, children under 5 years who are household contacts of DS-TB patients and who have been evaluated and have NO active TB are given isoniazid preventive therapy (IPT): isoniazid 10 mg/kg/day (maximum 300 mg/day) for 6 months. This is the standard chemoprophylaxis. Option A is incorrect — children <5 years are at high risk of rapid progression to severe TB (miliary, meningitis) and prophylaxis is mandatory regardless of Mantoux result in this age group. Option B (full treatment) would only be given if active TB were confirmed. Option D (RH 3 months) is not the standard NTEP chemoprophylaxis protocol for contacts.
NTEP Programme Structure, DOTS, and Patient Communication
The National Tuberculosis Elimination Programme (NTEP) is India's national TB control infrastructure, operating under the Ministry of Health and Family Welfare. Its goal — TB elimination by 2025, defined as fewer than 1 case per 100,000 population — is among the most ambitious public health targets globally, set 25 years ahead of the WHO Global Strategy. Understanding the programme structure is not merely academic; as a physician you are a participant in NTEP, and your actions — notification, regimen prescription, adherence monitoring, and contact tracing — directly determine whether the programme achieves its targets.
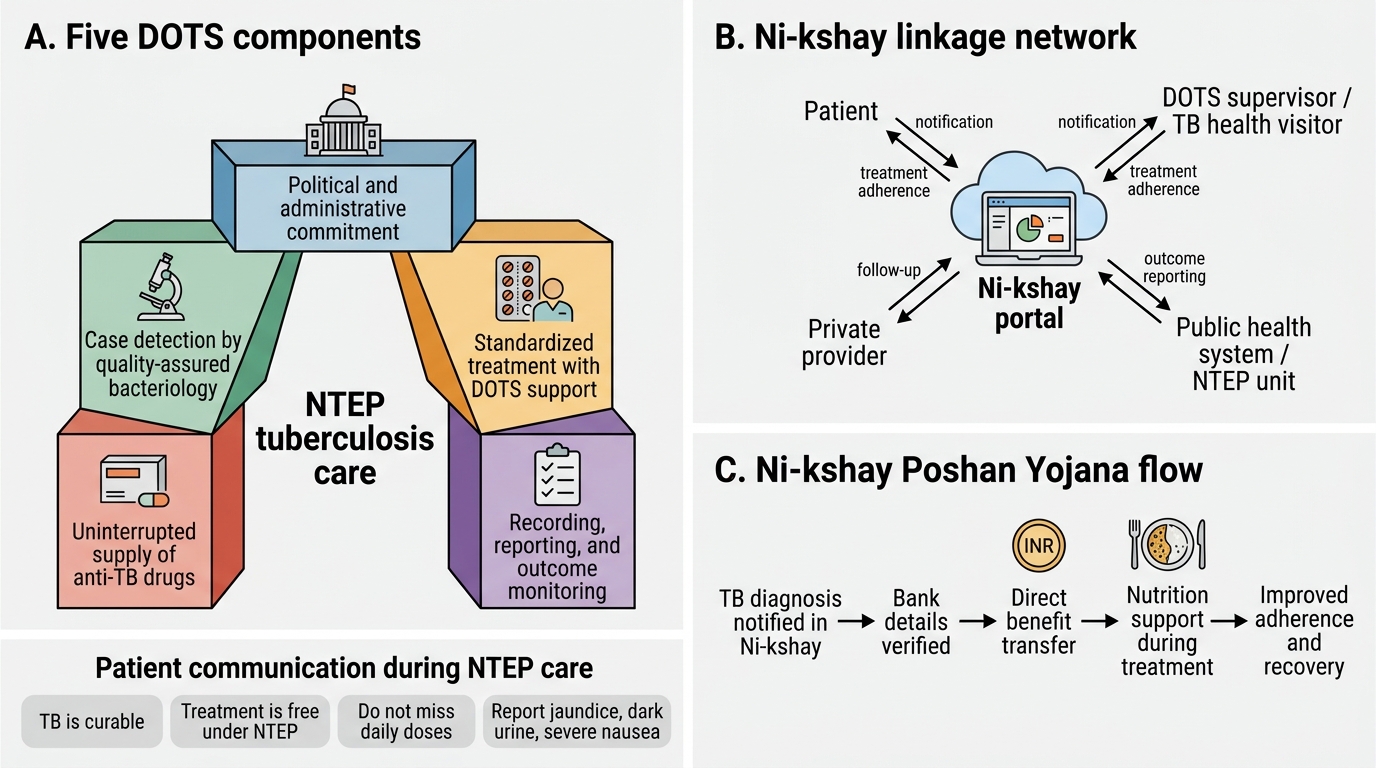
The DOTS (Directly Observed Treatment, Short-course) strategy is the operational core of NTEP. The five DOTS components, as defined by the WHO/NTEP framework, are: (1) political commitment with increased and sustained financing; (2) case detection through quality bacteriological services (CBNAAT as first-line, smear microscopy, culture and DST); (3) standardised treatment with supervision and patient support; (4) effective drug supply and management systems (FDC tablets, uninterrupted supply chain); and (5) monitoring and evaluation system to measure outcomes and programme performance. The DOTS treatment supporter — a community volunteer, ASHA worker, or healthcare worker at a DOTS centre — observes each dose ingestion directly and records it in the Ni-kshay system. Under the updated patient-centred DOTS, video-observed treatment (VOT) via mobile applications is now an accepted alternative for patients who cannot physically attend daily.
Ni-kshay notification is mandatory within 24 hours of diagnosis for ALL TB patients (pulmonary and extrapulmonary; bacteriologically confirmed and clinically diagnosed; public and private sector). Key information recorded includes patient demographics, case type, site of disease, HIV status, diabetes status, and treatment category. Failure to notify carries legal consequences under the Notifiable Diseases Act. Ni-kshay also triggers:
- Ni-kshay Poshan Yojana: Nutritional support of ₹500/month to the patient directly transferred to their bank account for the duration of treatment — addressing the chronic undernutrition that both predisposes to and results from TB.
- Patient tracking: if a patient misses doses, the system alerts the treatment supervisor for immediate follow-up.
NTEP, DOTS, Ni-kshay, and Patient Support
Communicating with patients about TB diagnosis and treatment is a competency (IM27.18) that requires specific skills beyond clinical knowledge. TB carries a powerful social stigma in India — it is associated with poverty, malnutrition, crowding, and in some communities with moral failure. Many patients conceal their diagnosis from employers and extended family out of fear of social exclusion, job loss, or abandonment. HIV co-infection adds a second layer of stigma. An effective patient consultation must:
- Deliver the diagnosis clearly and honestly: use plain language without jargon, explain that TB is a curable disease, and explicitly state that the standard treatment is free under NTEP.
- Explain the treatment: describe the duration (6 months minimum, 18–20 months for MDR-TB), the daily nature of DOTS, the importance of not missing doses, and what side effects to watch for — particularly the harmless orange-red urine from rifampicin (warn proactively to prevent panic-driven discontinuation), and the warning signs of hepatotoxicity (jaundice, dark urine, nausea) that require immediate medical review.
- Address fears and misconceptions directly: reassure the patient that TB is treatable, that most patients are non-infectious within 2–3 weeks of starting treatment, and that family members will be evaluated and given prophylaxis if needed.
- Respect autonomy and confidentiality: a patient's TB status should not be disclosed to employers or community members without explicit consent; the exception is public health notification (Ni-kshay), which is legally mandated and should be explained to the patient.
- Facilitate adherence: identify and problem-solve adherence barriers — working hours, distance to DOTS centre, disclosure concerns, side effects. VOT may be a practical solution for employed patients who cannot attend daily.
- Counsel contacts: explain to the patient that household contacts — particularly children under 5 and elderly individuals — must be evaluated, and that preventive treatment will be offered if needed. This is a collaborative, not a coercive, process.
CLINICAL PEARL
Three high-yield pearls for NTEP TB treatment:
1. Never cite the thrice-weekly intermittent regimen. The RNTCP-era thrice-weekly DOTS regimen has been completely replaced by daily FDC dosing under NTEP. Any prescription of alternate-day or three-times-weekly ATT is now incorrect under the national programme. The shift to daily FDC improved pharmacokinetics, reduced resistance amplification on missed doses, and simplified regimen labelling.
2. Rifampicin's drug interactions are clinically significant and frequently missed. The most important in Indian practice: (a) oral contraceptives — rifampicin induces CYP3A4 and reduces OCP efficacy to sub-therapeutic levels; women on ATT must be switched to barrier contraception or an intrauterine device; (b) ART in HIV co-infected patients — rifampicin reduces efavirenz levels by ~30% but remains the preferred combination (efavirenz dose adjusted to 800 mg in patients >60 kg if below target levels; nevirapine should NOT be used); (c) warfarin — INR will drop dramatically on starting rifampicin; frequent INR monitoring and dose increase is required.
3. Sputum smear positive at month 2 does NOT automatically mean treatment failure. A patient may remain smear-positive at month 2 due to non-viable dead bacilli being cleared slowly — this is not necessarily treatment failure. The correct response is to perform CBNAAT: if rifampicin sensitive, extend the intensive phase by one month (3HRZE intensive phase total); only if CBNAAT shows rifampicin resistance or smear remains positive at month 5+ is treatment failure declared.
Self-Assessment: Applying NTEP Treatment Principles
The following scenarios are designed to consolidate your application of NTEP treatment protocols, pharmacological knowledge, and patient communication skills. Each scenario reflects the kinds of judgements you will be expected to make in the OPD, ward, and public health context. Work through the clinical information, apply the principles from earlier sections, and reach a management decision before reading the analysis. These scenarios cover the NMC competencies IM27.13–IM27.18 at the level expected for a final-year student: not only knowing the regimen, but understanding why, recognising when to modify it, and communicating the plan to the patient. The competencies span pharmacology (IM27.13), prescribing (IM27.14), chemoprophylaxis (IM27.15), cure criteria and DR-TB (IM27.16), DOTS programme education (IM27.17), and patient communication (IM27.18) — each of these is represented in the scenarios below. Before working through the cases, use the reference summary table below to anchor the key regimens and outcomes in memory.
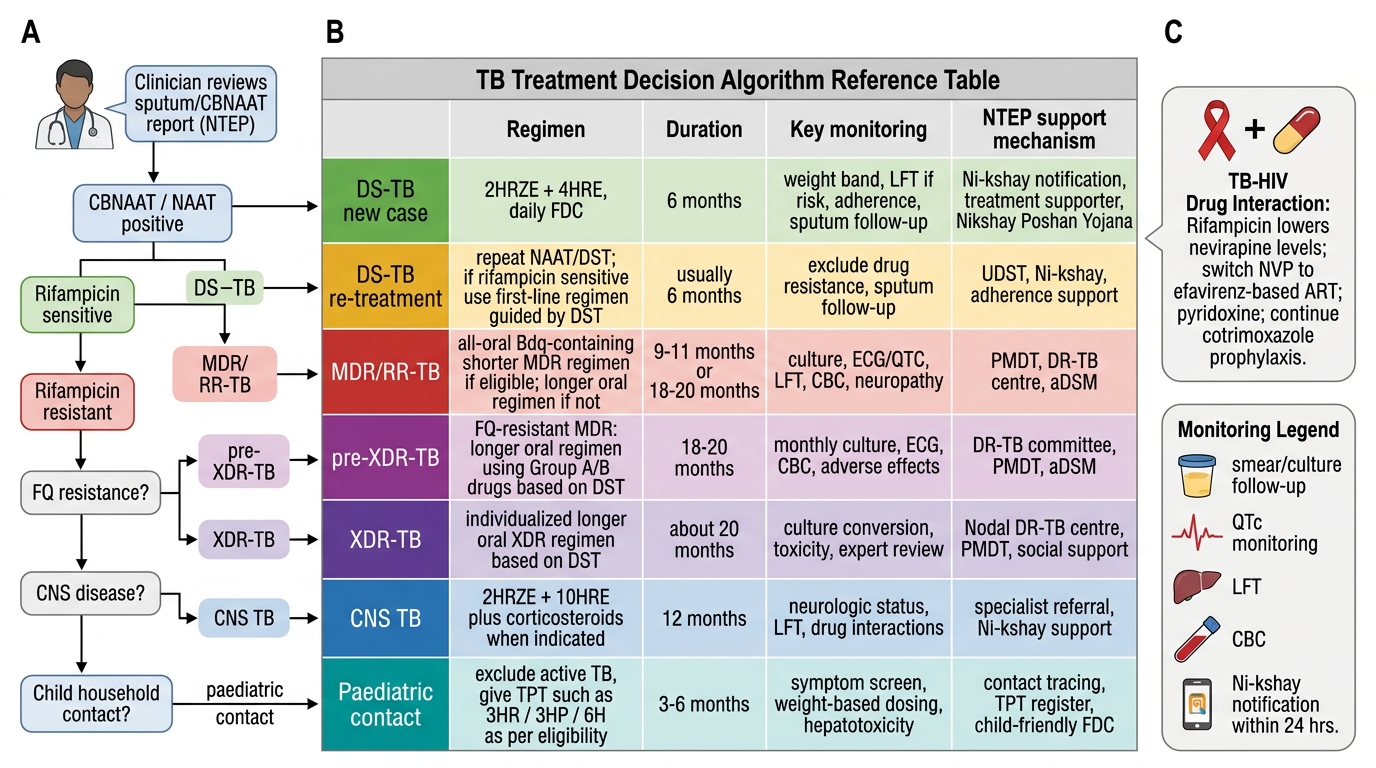
NTEP-Based TB Treatment Decision Reference
Scenario A: Mohan, 38 years old (weight 52 kg), newly diagnosed pulmonary TB (CBNAAT positive, rifampicin sensitive). He is also known to be HIV-positive and is currently on an ART regimen containing nevirapine. What regimen do you prescribe, and what modification do you make to his ART?
Analysis: Standard DS-TB regimen: 2HRZE + 4HRE, daily, weight band <55 kg = 3 tablets of HRZE FDC daily in intensive phase; 3 tablets HRE FDC daily in continuation phase. Notify on Ni-kshay within 24 hours. Pyridoxine 10–25 mg/day (particularly important with HIV-related neuropathy risk). ART modification: Rifampicin induces CYP3A4 and reduces nevirapine levels to sub-therapeutic concentrations. Switch ART from nevirapine to efavirenz 600 mg/day (efavirenz is the preferred NNRTI in rifampicin-based ATT). Continue ATT without delay; ART should be initiated as soon as possible if not already started (within 2 weeks for TB patients with CD4 <50, within 8 weeks for CD4 ≥50 — WHO/NACO TB-HIV guidelines). Cotrimoxazole prophylaxis must also be maintained.
Scenario B: Priya, 29 years old, was treated for pulmonary TB 14 months ago (completed treatment, declared cured). She now presents with recurrent cough, haemoptysis, and weight loss for 3 months. CBNAAT is positive for M. tuberculosis but rifampicin susceptibility is indeterminate on first test. What do you do?
Analysis: This is a previously treated TB case with recurrence. Previously treated cases have substantially higher rates of acquired drug resistance. Do NOT start empirical DS-TB treatment. Repeat CBNAAT on a fresh sputum sample. Send sputum for culture and conventional DST (Löwenstein-Jensen medium) and for Line Probe Assay (LPA) for rapid detection of rifampicin and isoniazid resistance. Await DST results. If CBNAAT on the second sample confirms rifampicin susceptibility (and isoniazid sensitivity on LPA), treat with DS-TB re-treatment regimen; if rifampicin resistance is confirmed, enrol in the MDR-TB pathway. Do not delay notification while awaiting full DST.
Scenario C: Sunita, 32 years old, is diagnosed with MDR-TB (CBNAAT rifampicin resistant; LPA confirms isoniazid resistance; no fluoroquinolone resistance detected). She is frightened and says, "I have heard MDR-TB has a very low cure rate and I don't want to take so many medicines. I would rather just rest at home." How do you respond?
Analysis: This is a patient communication challenge (IM27.18). The response should be empathetic, clear, and honest without being coercive. Key points to convey: (1) With the current NTEP MDR-TB regimen (all-oral, bedaquiline-based), treatment success rates for MDR-TB without fluoroquinolone resistance have improved significantly — approximately 55–70% success globally, with better outcomes in younger patients without significant comorbidities. (2) Acknowledging her fears is essential: she is right that MDR-TB treatment is harder and longer (18–20 months) than standard TB. (3) Explain that treatment is free under NTEP and that a dedicated MDR-TB team will support her. (4) Discuss the consequences of not treating — MDR-TB is fatal if untreated and she will remain infectious, placing her family at risk. (5) Respect autonomy — ask what specifically frightens her (side effects? Duration? Social disclosure?) and address each concern directly. Arrange a counselling session with the district NTEP MDR-TB counsellor. Enrol in Ni-kshay and initiate Ni-kshay Poshan support.