Page 1 of 22
IM28.1-7 | Obstructive Airway Disease Foundations — SDL Guide
Learning Objectives
- Define and classify obstructive airway diseases including asthma and COPD
- Describe the epidemiology, risk factors and natural history of obstructive airway disease
- Enumerate the causes of acute exacerbations in obstructive airway disease
- Discuss the physiology and pathophysiology of hypoxia and hypercapnia in obstructive airway disease
- Explain the genetics of alpha-1 antitrypsin deficiency and its role in emphysema
- Describe the role of environmental and occupational factors in causing and exacerbating obstructive airway disease
- Distinguish allergic from non-allergic precipitants of obstructive airway disease
INSTRUCTIONS
Obstructive airway disease — encompassing asthma and chronic obstructive pulmonary disease (COPD) — is among the most prevalent and burden-generating respiratory conditions worldwide, and is of particular importance in the Indian clinical context. This foundational module establishes the definitional, epidemiological, pathophysiological, genetic, and environmental framework on which all subsequent clinical and management learning depends. Master the distinctions between asthma and COPD early; they share obstruction as a physiological hallmark but differ profoundly in reversibility, mechanism, and natural history.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 281–282 — Asthma and COPD (textbook)
- API Textbook of Medicine, 10th ed., Ch. — Obstructive Lung Diseases (textbook)
- GINA Report: Global Strategy for Asthma Management and Prevention, 2023 (guideline)
- GOLD Report: Global Strategy for Diagnosis, Management and Prevention of COPD, 2023 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan is a 58-year-old retired textile mill worker from Coimbatore. For the past three years he has noticed progressive breathlessness on exertion — initially only on climbing stairs, now even when walking to the kitchen. He has a 35-pack-year smoking history. His morning cough produces grey sputum daily, and he has been admitted twice in the last year with worsening breathlessness and purulent sputum, treated as 'chest infection'. His son, who lives in the same house, is 22 years old and has had repeated episodes of nocturnal cough, chest tightness, and wheezing since childhood — triggered by dust, cold air, and exercise, all of which fully resolve with a salbutamol inhaler. Two people in the same household — same symptom of breathlessness — but entirely different diseases. Understanding the foundations of obstructive airway disease means understanding precisely why Rajan and his son, despite sharing the word 'obstruction' as their physiological problem, have arrived at that obstruction by completely different pathways, will respond differently to treatment, and face very different prognoses.
WHY THIS MATTERS
India carries one of the largest burdens of obstructive airway disease in the world. The Global Burden of Disease study estimates approximately 37 million people in India have COPD, accounting for over 10% of global COPD deaths. Asthma prevalence in India is estimated at 17–18 million, with urban and peri-urban populations showing rising rates linked to air pollution, indoor biomass fuel combustion, and changing allergen exposure. As a final-year MBBS graduate, you will encounter breathless patients daily — in the emergency department with acute exacerbations, in the outpatient clinic requiring step-up of therapy, and on the ward with respiratory failure requiring oxygen decisions. Competency IM28.1–28.7 requires you to define these diseases, classify their severity, understand their mechanisms, recognise their precipitants, and explain their environmental and genetic underpinnings — the bedrock of rational clinical management.
RECALL
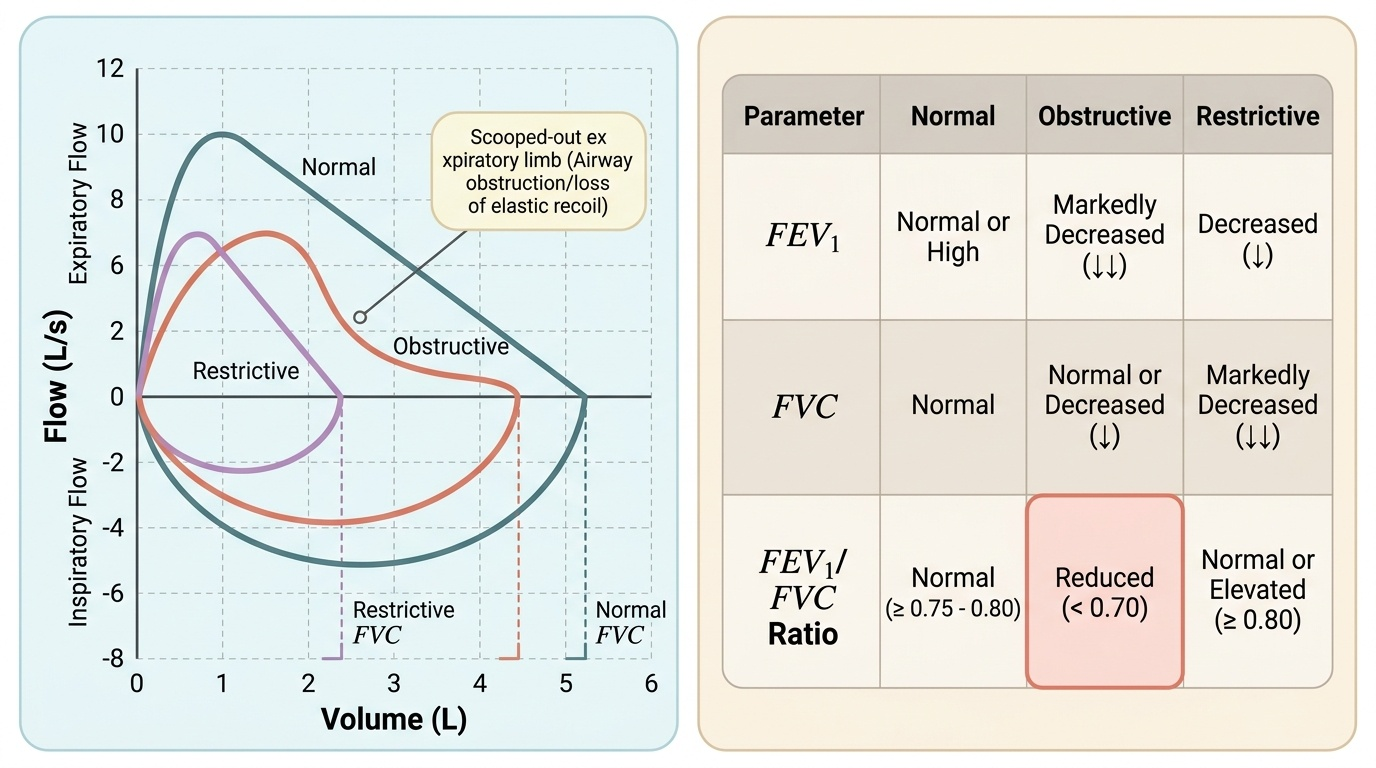
Reactivate your knowledge of respiratory physiology before proceeding. The forced expiratory volume in 1 second (FEV1) is the volume of air that can be forcibly exhaled in the first second of a maximal exhalation from full inspiration; it reflects large- and medium-airway calibre. The forced vital capacity (FVC) is the total volume forcibly exhaled from full inspiration to complete expiration. In health, the FEV1/FVC ratio is ≥0.70–0.75. Airway obstruction is defined as a reduction in this ratio — meaning the patient cannot empty the lungs as quickly as expected for their lung volume, because something is narrowing or collapsing the airways. Recall also the basic anatomy: bronchi divide to bronchioles, which terminate in respiratory bronchioles and alveoli; goblet cells and submucosal glands secrete mucus; mast cells and eosinophils reside in the airway wall and are activated in allergic inflammation; smooth muscle surrounds the conducting airways and its contraction — bronchospasm — is immediately reversible with bronchodilators. These structural elements are the targets of obstructive disease.
Definition and Classification of Obstructive Airway Disease
Obstructive airway disease (OAD) is a broad term encompassing any condition characterised by airflow limitation due to narrowing, inflammation, or dynamic collapse of the airways. The unifying physiological criterion is a reduced FEV1/FVC ratio — the hallmark of obstruction on spirometry — though the degree, reversibility, and anatomical distribution of obstruction differ substantially between the major diseases grouped under this umbrella. Understanding the definitional distinctions between asthma and COPD is not a semantic exercise; it is the basis for choosing the correct investigation strategy, treatment paradigm, and prognostic framework.
Provided image
Asthma is defined by the Global Initiative for Asthma (GINA) as a heterogeneous disease characterised by chronic airway inflammation, with a history of respiratory symptoms such as wheeze, shortness of breath, chest tightness, and cough that vary over time and in intensity, together with variable expiratory airflow limitation. Three features are definitionally central: the airway inflammation is chronic and predominantly eosinophilic or mast-cell-driven (in allergic asthma); the airflow limitation is variable and largely reversible — either spontaneously or with bronchodilator therapy; and the symptoms display a pattern (worse at night or early morning, triggered by identifiable stimuli, often with symptom-free intervals). The reversibility criterion is defined spirometrically as an increase in FEV1 of ≥12% and ≥200 mL from baseline after inhalation of a short-acting bronchodilator (e.g., salbutamol 400 mcg). This reversibility distinguishes asthma from COPD at the physiological level.
Chronic obstructive pulmonary disease (COPD) is defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD) as a heterogeneous lung condition characterised by chronic respiratory symptoms (dyspnoea, cough, sputum production, exacerbations) due to airway (bronchitis, bronchiolitis) and/or alveolar (emphysema) abnormalities that cause persistent, progressive airflow limitation that is not fully reversible. The GOLD diagnostic spirometric criterion is post-bronchodilator FEV1/FVC < 0.70 (fixed ratio). The persistence and only partial reversibility of the airflow limitation is the defining physiological contrast with asthma. COPD encompasses two pathologically distinct but often co-existing entities: chronic bronchitis (defined clinically as productive cough for ≥3 months per year for ≥2 consecutive years, in the absence of other explanatory cause) and emphysema (defined anatomically as permanent abnormal enlargement of the air spaces distal to the terminal bronchiole, with destruction of alveolar walls, without obvious fibrosis).
GOLD classification of COPD severity is based on post-bronchodilator FEV1 as a percentage of predicted:
- GOLD 1 (Mild): FEV1 ≥80% predicted
- GOLD 2 (Moderate): 50% ≤ FEV1 < 80% predicted
- GOLD 3 (Severe): 30% ≤ FEV1 < 50% predicted
- GOLD 4 (Very Severe): FEV1 <30% predicted
Note that the updated GOLD 2023 report has moved toward an ABE assessment framework (A = low symptom/low risk, B = high symptom/low risk, E = exacerbation risk) as a clinical management complement to the spirometric grading — but for the purposes of NMC examination, the GOLD 1–4 spirometric grades remain the core classification.
GINA asthma severity classification (before treatment initiation) is based on symptom frequency and the treatment step required to achieve control:
- Intermittent: daytime symptoms ≤2 days/week, no night awakening, SABA use ≤2 days/week, normal between attacks
- Mild persistent, Moderate persistent, Severe persistent — based on increasing frequency of symptoms and more severe spirometric impairment.
A key differential between asthma and COPD in clinical practice:
| Feature | Asthma | COPD |
|---|---|---|
| Age of onset | Often childhood/young adult | Typically >40 years |
| Smoking history | Not required | Major cause (>90%) |
| Airflow obstruction | Reversible (≥12%+200 mL) | Persistent (FEV1/FVC <0.70 post-BD) |
| Predominant cells | Eosinophils, mast cells | Neutrophils, macrophages |
| Atopy | Common | Less common |
| Diurnal variation | Marked | Less prominent |
| Disease progression | Episodic, may remit | Steadily progressive |
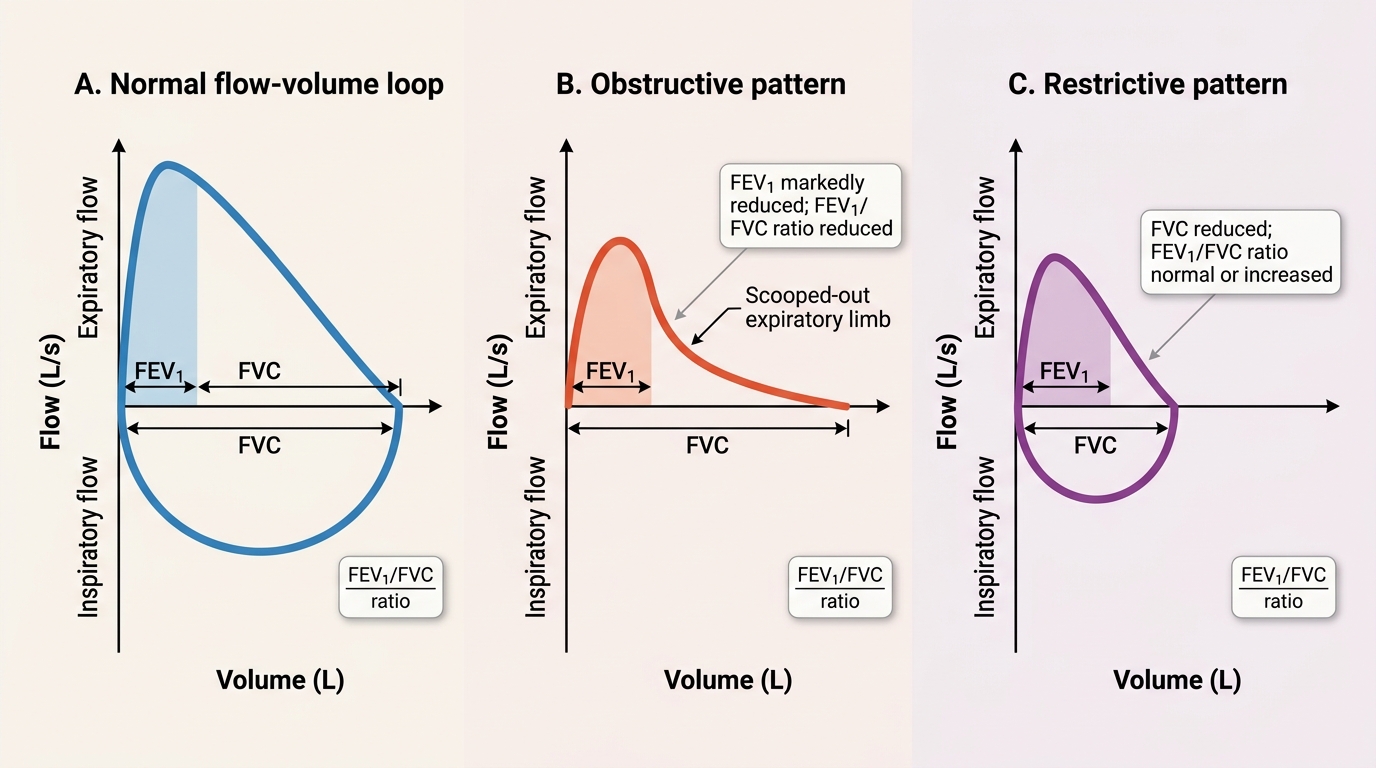
Spirometry Flow-Volume Loop Patterns
Epidemiology, Risk Factors, and Natural History
The global and Indian epidemiological burden of obstructive airway disease is substantial and rising, driven by urbanisation, ageing populations, persistent tobacco use, and indoor and outdoor air pollution. Appreciating the scale of this burden is not merely academic — it underpins public health policy, resource allocation, and the urgency with which you must apply preventive counselling in every clinical encounter.
Global epidemiology: COPD affects approximately 391 million people worldwide, with a prevalence of approximately 10–15% in adults over 40 years. Asthma affects approximately 300 million people globally. Together, obstructive airway diseases are the third leading cause of death worldwide. The 2019 GBD study estimated COPD mortality at 3.23 million deaths globally, with India contributing disproportionately — accounting for approximately 32% of all COPD deaths worldwide. India's high COPD burden is attributable to the confluence of tobacco smoking (both cigarette and bidi, which delivers higher tar concentrations per unit smoked), biomass fuel combustion (wood, crop residue, and dung used for cooking in an estimated 50–70% of rural households), occupational dust exposures (textile, mining, construction, agricultural sectors), and historical under-treatment. Asthma prevalence in India is approximately 2–3% of the adult population, with higher rates in urban children (up to 10–15%) due to increasing allergen sensitisation and air pollution.
Risk factors for COPD can be organised into host and environmental categories:
- Host factors: genetic susceptibility (alpha-1 antitrypsin deficiency — discussed below), airway hyperresponsiveness, lung growth abnormalities in utero or early childhood (low birth weight, prematurity, childhood respiratory infections — the 'early life origins' of COPD), and sex (historically male-predominant, but female risk is increasing as more women smoke and use biomass fuels)
- Environmental factors: tobacco smoking (greatest modifiable risk; dose–response relationship — risk rises with pack-years; risk at 20 pack-years is substantial; 80–90% of COPD in high-income countries is attributable to smoking); biomass fuel smoke (major cause in Indian women — indoor burning of wood, cow dung, crop residue); occupational dust and chemical exposure (cadmium, silica, coal dust, isocyanates, grain dust); outdoor air pollution (PM2.5 and ozone); recurrent lower respiratory infections in childhood
Risk factors for asthma similarly span host and environmental domains:
- Host: atopy (genetic predisposition to IgE-mediated sensitisation — strongest single risk factor for allergic asthma); family history; obesity (independently associated with non-atopic asthma through mechanical and inflammatory mechanisms)
- Environmental: early allergen sensitisation (house dust mite, cockroach, animal dander, Alternaria mould — the 'sensitisers'); respiratory viral infections in early childhood (RSV, rhinovirus — the 'promoters' of the asthmatic phenotype in genetically susceptible individuals); the hygiene hypothesis proposes that reduced childhood microbial exposure in urban, hygienic environments shifts immune responses toward Th2 (allergic) pathways; outdoor air pollution (traffic-related ozone and NO₂); tobacco smoke exposure (particularly in utero and in early childhood)
Natural history of COPD: Fletcher and Peto's classic longitudinal data established that FEV1 declines by approximately 30 mL/year in healthy non-smokers after age 25, but the rate accelerates to 50–80 mL/year or more in susceptible smokers. Not all smokers develop COPD — approximately 15–20% of smokers develop clinically significant disease — suggesting a genetic-environmental interaction in disease susceptibility. Smoking cessation at any stage reduces but does not reverse the rate of FEV1 decline. Exacerbations accelerate FEV1 decline and are associated with increased mortality. The natural history of COPD involves a transition from asymptomatic airflow limitation through exertional dyspnoea to severe limitation with hypoxic respiratory failure and cor pulmonale in advanced disease.
Natural history of asthma: allergic asthma often begins in childhood, may undergo clinical remission in adolescence and early adulthood (but airway hyperresponsiveness may persist), and can recur in adulthood. Severe or undertreated asthma can lead to irreversible airway remodelling — a process of structural change (basement membrane thickening, subepithelial fibrosis, smooth muscle hypertrophy) that progressively reduces the reversibility component and makes the disease COPD-like.
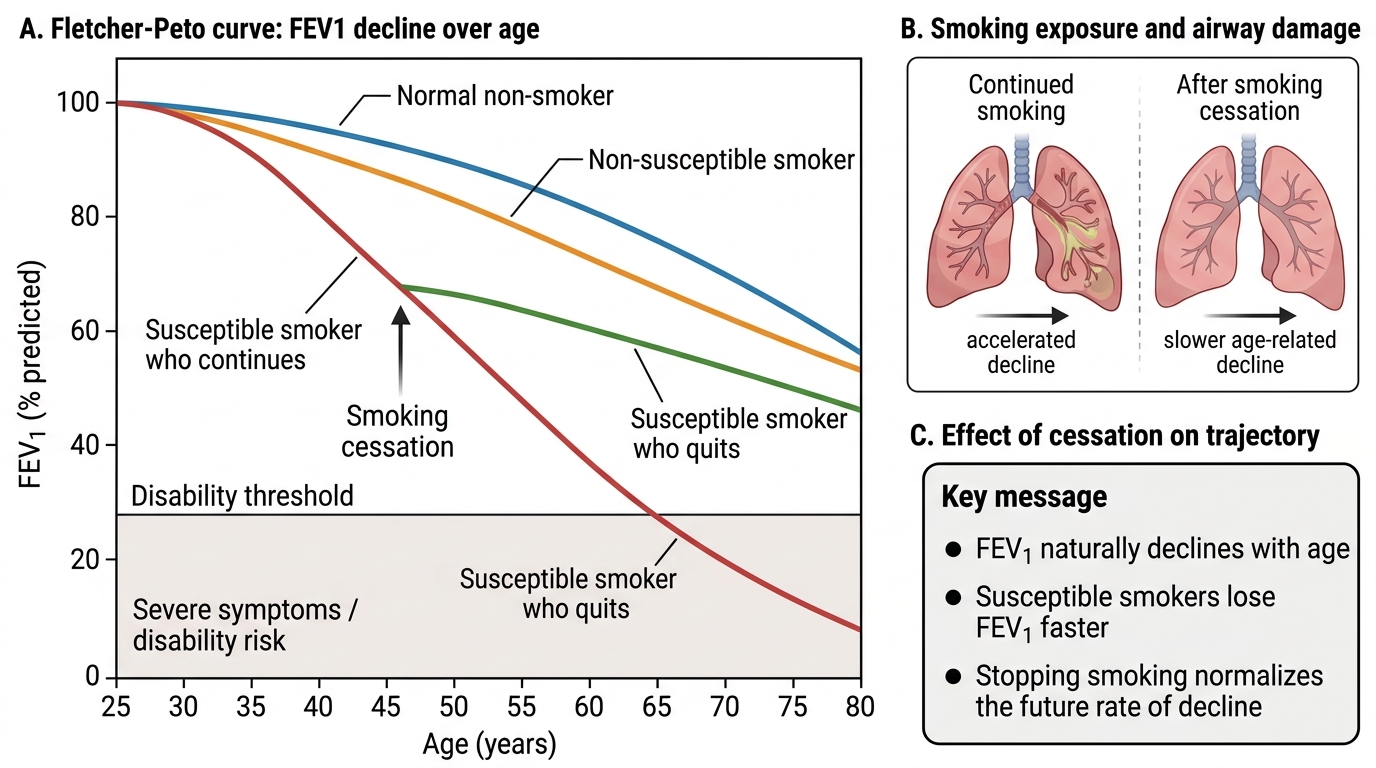
Fletcher-Peto Curve and Effect of Smoking Cessation
SELF-CHECK
A 55-year-old male smoker presents with progressive breathlessness. Post-bronchodilator spirometry shows FEV1/FVC of 0.62. Which of the following best defines his diagnosis according to GOLD criteria?
A. Asthma — because there is airflow obstruction
B. COPD — post-bronchodilator FEV1/FVC < 0.70 with appropriate clinical context
C. Restrictive lung disease — FEV1 is below predicted
D. Asthma-COPD overlap — because smoking and airflow obstruction coexist
Reveal Answer
Answer: B. COPD — post-bronchodilator FEV1/FVC < 0.70 with appropriate clinical context
GOLD defines COPD as persistent airflow limitation with post-bronchodilator FEV1/FVC < 0.70 in the presence of appropriate exposure history (smoking, biomass fuel, occupational exposure) and symptoms (cough, dyspnoea). The ratio of 0.62 is below the GOLD threshold of 0.70. A low FEV1/FVC does not indicate restriction — that requires a reduced FVC with preserved ratio. Asthma is characterised by reversible obstruction (≥12% and ≥200 mL improvement); if this is absent, COPD is the diagnosis. ACOS (asthma-COPD overlap) has specific features of both and is not a default label for any smoker with obstruction.
Causes of Acute Exacerbations
An acute exacerbation of obstructive airway disease represents a clinically significant, time-limited worsening of respiratory symptoms beyond the patient's usual day-to-day variation, sufficient to warrant a change in treatment. Recognising and enumerating the causes of acute episodes is critical because prompt identification and treatment of the precipitant is integral to the management strategy — treating the exacerbation without addressing the trigger leads to an incomplete response and rapid recurrence. Acute exacerbations are also the major driver of hospitalisation, emergency visits, healthcare cost, accelerated lung function decline, and mortality, particularly in COPD. An important concept is that exacerbation frequency itself predicts future exacerbation risk — patients who have experienced two or more exacerbations in the previous year are classified as 'frequent exacerbators' and require intensified preventive therapy. In asthma, each exacerbation represents an opportunity to review adherence, inhaler technique, trigger identification, and the adequacy of controller therapy. Understanding the breadth of potential precipitants — from viral pathogens and bacterial colonisers to environmental pollutants, pharmacological agents, and physiological stressors — allows the clinician to counsel patients proactively about avoidance strategies and to make targeted therapeutic adjustments rather than treating every exacerbation identically.
Provided image
Infectious precipitants (most common cause — 70–80% of COPD exacerbations):
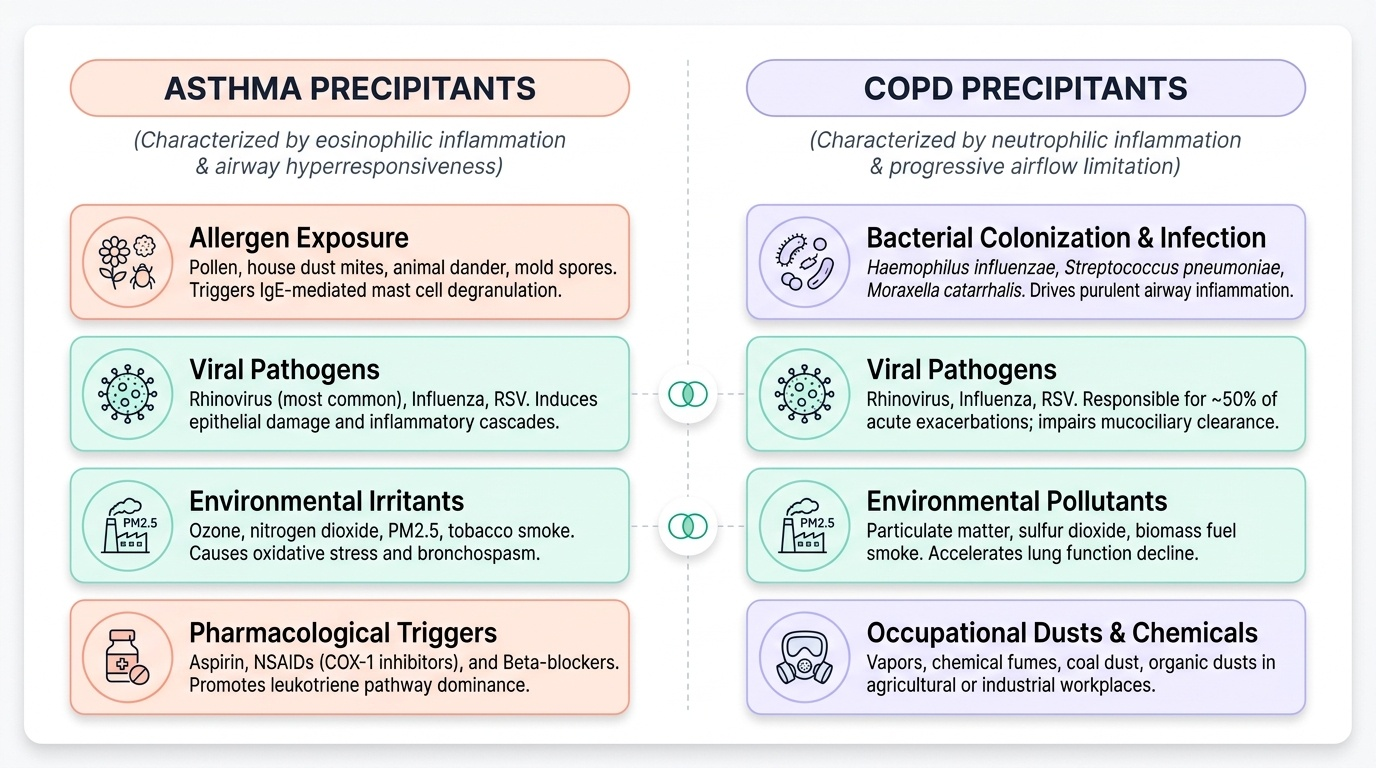
- Respiratory viral infections — responsible for approximately 50% of exacerbations; rhinovirus (the commonest), influenza A and B, respiratory syncytial virus (RSV), parainfluenza, coronavirus, adenovirus. Viral infections trigger inflammatory cascades, impair mucociliary clearance, and allow bacterial colonisation — often precipitating a combined viral-bacterial exacerbation
- Bacterial infections — the most common bacteria isolated in COPD exacerbations are Haemophilus influenzae (non-typeable), Streptococcus pneumoniae, and Moraxella catarrhalis. Pseudomonas aeruginosa is important in severe COPD (GOLD 3–4) and in patients with bronchiectasis. Bacterial exacerbations are identified clinically by the presence of purulent sputum (Anthonisen criteria — increased dyspnoea, increased sputum volume, purulent sputum; a type-1 exacerbation has all three and has the highest likelihood of bacterial aetiology)
Environmental and physical precipitants:
- Air pollution — outdoor pollution events (high PM2.5, ozone, NO₂, SO₂ days) are well-established triggers of both asthma and COPD exacerbations; the relationship is dose-dependent and affects the entire population but disproportionately those with pre-existing lung disease. In India, Diwali fire-cracker pollution and crop-residue burning (particularly in the Punjab-Haryana belt in October–November) annually precipitate a surge in respiratory admissions
- Indoor allergen exposure (for asthma) — house dust mite, cockroach allergen (high concentrations in urban Indian homes), pet dander, Alternaria mould spores in damp housing; these trigger IgE-mediated mast cell degranulation with immediate bronchospasm (early-phase) followed by eosinophilic inflammation (late-phase)
- Occupational exposures — flour dust (bakers), textile dusts (cotton byssinosis), isocyanates (paint sprayers, polyurethane workers), wood and grain dust, welding fumes — any of these can precipitate work-related asthma exacerbations; symptoms often improve on weekends and holidays and worsen on return to work
- Cold air and exercise — exercise-induced bronchoconstriction (EIB) is mediated by airway cooling and drying during high-minute-ventilation exercise; cold air alone without exercise can trigger bronchospasm via airway osmolarity and thermal changes
- Aspirin and NSAIDs — in aspirin-exacerbated respiratory disease (AERD, Samter's triad): aspirin and NSAIDs block COX-1, redirecting arachidonic acid metabolism toward 5-lipoxygenase and excess leukotriene synthesis, causing severe bronchospasm; associated with nasal polyps and chronic eosinophilic sinusitis
- Gastro-oesophageal reflux disease (GORD) — micro-aspiration of acid and direct vagal nerve stimulation from oesophageal acidification can trigger bronchospasm; GORD is commoner in COPD patients due to diaphragm flattening and reduced lower oesophageal sphincter tone
- Beta-blockers — non-selective beta-blockers (propranolol, atenolol in higher doses) cause bronchospasm by blocking airway β₂-adrenoreceptors; cardioselective β₁-blockers (bisoprolol, metoprolol) have substantially reduced risk but should still be used with caution in moderate-severe asthma
Non-compliance and under-treatment: inadequate adherence to maintenance inhaler therapy (a common and underdiagnosed contributor in real-world practice), incorrect inhaler technique (a major problem — surveys show >70% of patients use inhalers incorrectly), and failure to titrate therapy with disease severity all contribute to episodes that appear to be exacerbations but are fundamentally management failures.
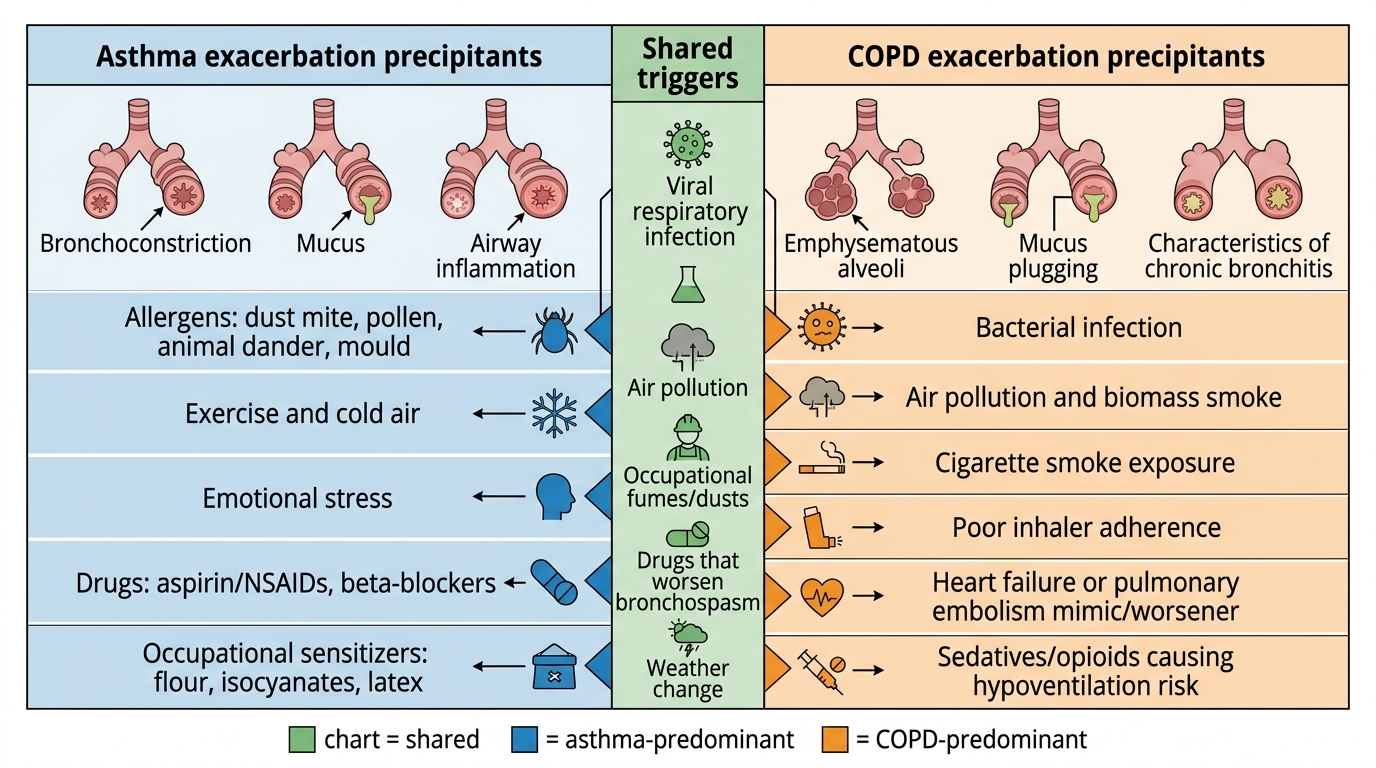
Precipitants of Acute Exacerbations in Asthma and COPD