Page 14 of 22
IM28.{20,23-26} | Obstructive Airway Disease Prevention and Patient Context — SDL Guide
Learning Objectives
- Describe the impact of OAD on patient quality of life, wellbeing, work, family, and society
- Counsel patients appropriately on smoking cessation using the 5As framework
- Describe and discuss preventive measures to reduce OAD in workplaces
- Demonstrate understanding of patients' inability to change working, living, and environmental factors that influence progression of airway disease
- Demonstrate understanding of the difficulties faced by patients during smoking cessation
INSTRUCTIONS
Prevention and patient context form the human framework around OAD pharmacotherapy. This module covers the skill domains of smoking cessation counselling, occupational health prevention, and empathic patient-centred care — all competencies that are tested behaviourally in clinical assessments and applied every day in practice.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Tobacco and Nicotine Addiction, Occupational Lung Disease (textbook)
- API Textbook of Medicine, 10th ed. — COPD: Social and Occupational Dimensions (textbook)
- GOLD Report: Global Strategy for COPD Management, 2023 — Smoking Cessation chapter (guideline)
- WHO Framework Convention on Tobacco Control (FCTC) — Cessation guidelines (guideline)
- National Programme for Prevention and Control of Cancer, Diabetes, CVD and Stroke (NPCDCS) — Tobacco cessation resources, India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You see three patients in a single COPD clinic morning. The first is a 58-year-old cotton mill worker who developed occupational asthma after 25 years of exposure to cotton dust — he cannot leave his job because it is his only income source and he supports a family of six; his employer has no respiratory surveillance programme. The second is a 62-year-old woman with severe COPD who has smoked since age 15 — she has tried to stop four times but relapsed each time because her husband smokes at home, she lives in a single-room house where she cannot avoid passive smoke, and she uses bidi because that is what is culturally normal in her community. The third is a 45-year-old software engineer with mild asthma whose home is near an industrial corridor; he is being rehoused for highway construction and asks you if moving will help his asthma. Each of these patients needs pharmacological treatment — but what differentiates good care from excellent care is your ability to understand their context, counsel them meaningfully on what they can change, and advocate for them on what they cannot. This module is about that.
WHY THIS MATTERS
Prevention and context competencies in OAD are not ancillary — they are core to clinical practice, community health, and professional responsibility. In India, where biomass fuel use in rural households affects 700 million people and tobacco use (including bidi, smokeless tobacco, and hookah) is widespread and culturally embedded, the individual clinical encounter is simultaneously a public health intervention. Smoking cessation is the single most effective intervention for COPD — more effective than any bronchodilator or combination inhaler — and yet counselling skills are among the least practised by doctors. Occupational respiratory hazards affect millions of agricultural workers, construction workers, textile workers, miners, and healthcare staff — many of whom are inadequately protected. Competencies IM28.20–28.26 directly prepare you for these encounters.
RECALL
Recall the pathophysiological basis of tobacco damage before proceeding. Cigarette smoke delivers over 4,000 chemicals, including oxidants, aldehydes, and particulates, to airway epithelium. Repeated oxidative stress activates NF-κB, releasing IL-8 and TNF-α, which recruit neutrophils and macrophages. Neutrophil elastase and macrophage-released matrix metalloproteinases (MMPs) destroy alveolar walls — emphysema. Simultaneously, submucosal gland hypertrophy and goblet cell metaplasia increase mucus production, narrowing airways — chronic bronchitis. The combined effect is irreversible airflow obstruction. Smoking cessation does not reverse existing damage but substantially slows the accelerated rate of FEV1 decline from the normal ~30 mL/year to near-normal — the Lung Health Study demonstrated this clearly. Earlier cessation = more lung function preserved.
OAD Impact on Quality of Life, Work, Family, and Society
Understanding the full burden of obstructive airway disease on a patient's life — beyond spirometric values and exacerbation frequency — is the foundation of person-centred care and is competency IM28.23. Obstructive airway disease is not simply a disease of the lungs; it is a disease of the whole person, and its consequences permeate every domain of life.
Impact on quality of life and daily functioning:
Breathlessness — the cardinal symptom of COPD and severe asthma — is profoundly disabling. The Medical Research Council (MRC) dyspnoea scale quantifies functional limitation: Grade 4 patients stop for breath after walking 100 metres on level ground, and Grade 5 patients are too breathless to leave the house or dress themselves. For an active working adult, this represents a catastrophic loss of independence. Standard QoL instruments (SGRQ — St George's Respiratory Questionnaire; CAT — COPD Assessment Test; Mini-AQLQ for asthma) consistently show that COPD patients have QoL scores comparable to those with severe heart failure and worse than many cancers. Dyspnoea drives anxiety and depression — approximately 40% of moderate-to-severe COPD patients have clinically significant anxiety or depression, which themselves worsen adherence, increase exacerbation frequency, and reduce survival. Sleep disturbance is universal in moderate-severe COPD due to nocturnal desaturation, recumbent worsening of dyspnoea, and frequent arousals. Exercise intolerance creates a vicious cycle: breathlessness on exertion → avoidance of activity → deconditioning → worsening dyspnoea on less exertion.
Impact on work and employment:
In India, a large proportion of COPD and occupational asthma patients are manual labourers — agricultural workers, construction workers, miners, weavers — whose work is physically demanding and whose livelihood depends directly on their physical capacity. COPD at GOLD 2–3 commonly leads to reduced work capacity, sick days, and ultimately early retirement or disability. Studies from Indian tertiary centres show that 60–70% of working-age COPD patients have reduced work output and many face termination or demotion. In the informal sector, there is no sick leave, no disability benefit, and no occupational health protection — a patient with severe COPD who can no longer work has no social safety net. Beyond physical incapacity, stigma of lung disease in communities with high tobacco prevalence creates additional employment barriers.
Impact on family:
COPD and asthma impose a substantial burden on family caregivers — particularly spouses and adult children — who provide day-to-day support with mobility, medication management, and emergency responses during exacerbations. Financial burden is severe: in India, out-of-pocket healthcare expenditure accounts for 65–70% of total health expenditure, and a single hospitalisation for AECOPD can consume several months of household income in low-income families. Caregiver burnout and family stress are common but rarely addressed in the outpatient consultation. Children in households with a smoking COPD patient are exposed to passive smoke, increasing their own risk of developing asthma.
Societal impact:
The economic burden of OAD in India is enormous — direct costs (hospitalisation, medication, investigations) plus indirect costs (lost productivity, premature death). COPD is projected to be the third leading cause of death globally by 2030, with India bearing a disproportionate share due to biomass fuel dependence, tobacco use, and aging population. The environmental burden — biomass fuel combustion in 700 million rural households producing particulate matter and carbon monoxide directly inhaled by women cooking over chulhas — is a structural determinant of OAD that transcends individual behaviour change.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
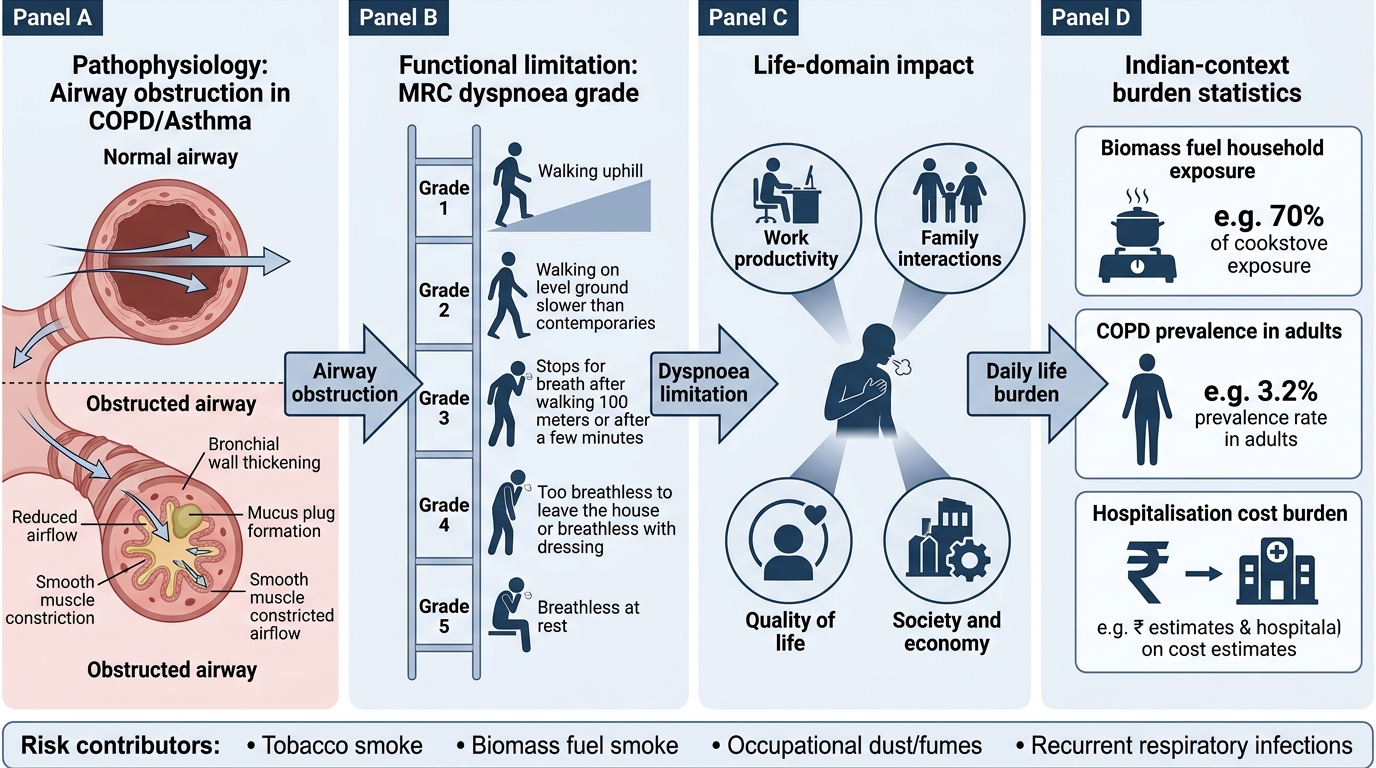
Obstructive Airway Disease Burden Cascade
Governing Principles of Behaviour Change and Occupational Health
Effective smoking cessation counselling and occupational health intervention both rest on sound theoretical and practical principles that shape the clinical approach. Understanding these principles — before applying the specific techniques — enables you to adapt your approach to the individual patient and the specific workplace, rather than applying a scripted protocol that fails to account for context.
Principles of behaviour change in tobacco cessation:
Nicotine dependence has two distinct but interlocking components: physical dependence (nicotine withdrawal syndrome — irritability, anxiety, restlessness, difficulty concentrating, increased appetite, craving — driven by upregulation of nicotinic acetylcholine receptors and decreased dopamine release during abstinence) and psychological/behavioural dependence (automatic cues — morning tea, post-meal smoking, stress-smoking, social smoking — where specific stimuli trigger the urge to smoke through conditioned reinforcement).
Effective cessation addresses both components simultaneously:
- Pharmacotherapy addresses the physical withdrawal: nicotine replacement therapy (NRT — patch, gum, lozenge, inhaler), varenicline (partial nicotinic agonist — reduces craving AND reduces reward of smoking if relapsed), bupropion (dopamine-noradrenaline reuptake inhibitor — reduces withdrawal symptoms and craving). Pharmacotherapy more than doubles the success rate of unaided cessation.
- Behavioural support addresses the psychological component: identifying and managing triggers, developing coping strategies, building self-efficacy, and providing social support. Brief advice from a physician (even 3 minutes) doubles the rate of cessation attempts. Intensive behavioural counselling (≥4 sessions) further improves outcomes.
- Motivational interviewing (MI) is the evidence-based communication approach for smoking cessation: non-confrontational, empathic, exploring the patient's ambivalence rather than issuing directives; reflective listening; rolling with resistance rather than arguing; exploring discrepancies between the patient's stated values ('I want to see my grandchildren grow up') and current behaviour ('I am still smoking'). MI is MORE effective than didactic advice, especially in pre-contemplative patients.
- Readiness to change (Transtheoretical Model): patients are at different stages — precontemplation (no intention to quit), contemplation (considering it), preparation (planning to quit within 30 days), action (actively quitting), maintenance (sustained abstinence). Counselling should be matched to stage; providing a cessation plan to a precontemplative patient is ineffective and may entrench resistance.
Principles of occupational health for OAD prevention:
Occupational lung diseases are caused by inhalation of hazardous dusts, gases, fumes, or vapours in the workplace. Prevention follows a hierarchy of hazard controls (descending effectiveness):
1. Elimination — remove the hazard from the workplace entirely (most effective; replace a hazardous substance with a safe one)
2. Substitution — replace a hazardous process with a less hazardous alternative
3. Engineering controls — physical changes to isolate the hazard (enclosed processes, local exhaust ventilation, dust suppression systems — wet drilling, water sprays in quarries)
4. Administrative controls — work practice changes (rotation of workers to limit individual exposure duration, standard operating procedures, job rotation)
5. Personal protective equipment (PPE) — respiratory protective equipment (RPE) such as particulate masks (FFP2/FFP3), powered air-purifying respirators (PAPR) for high-exposure tasks
PPE is the last resort in the hierarchy — the least effective because it relies entirely on individual compliance and proper fit. Engineering controls are preferred because they protect all workers regardless of individual behaviour. In practice in India, PPE is often the first (and only) control applied, which is a systematic inadequacy. Occupational health surveillance — regular spirometry and symptom screening of exposed workers — enables early detection of occupational asthma or COPD before irreversible damage occurs.
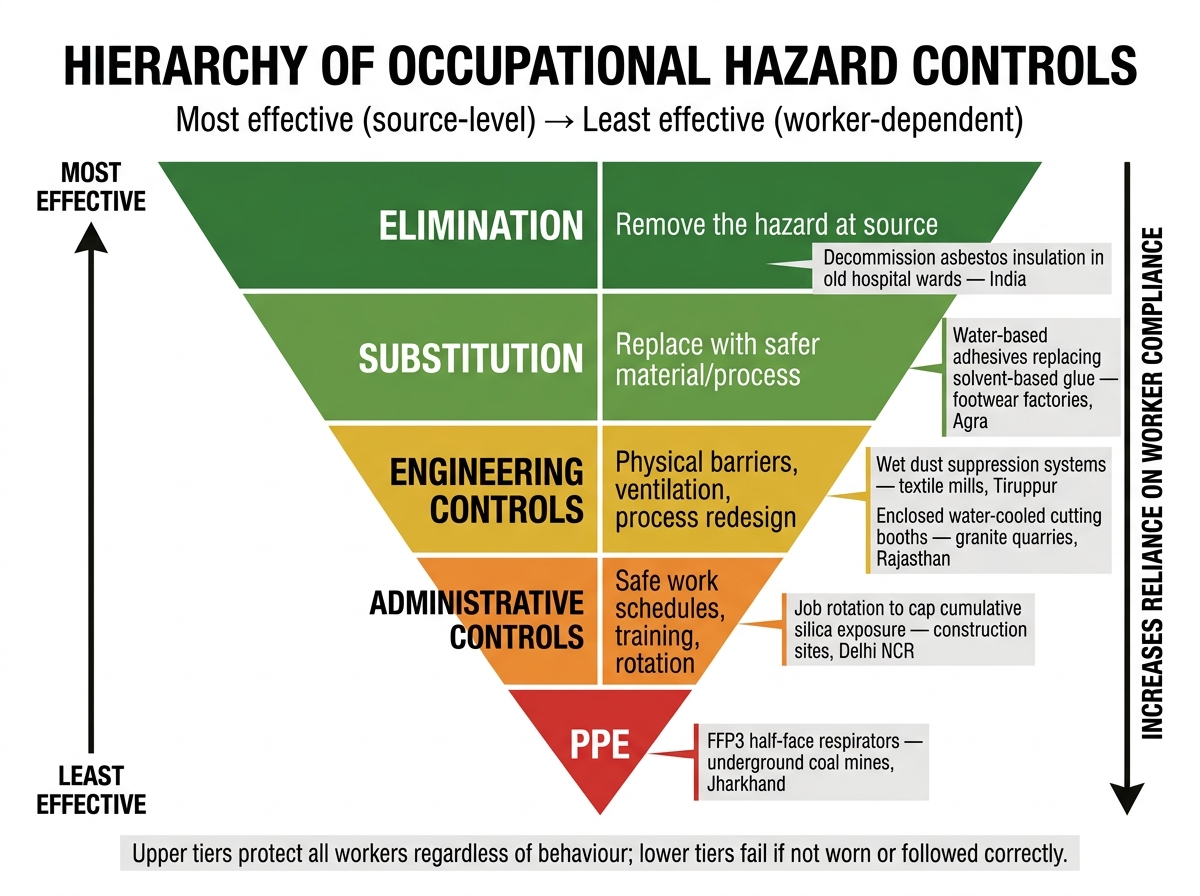
Hierarchy of Occupational Hazard Controls — Indian Workplace Examples
SELF-CHECK
A 50-year-old COPD patient who has smoked for 30 years tells you: 'I know I should quit but I enjoy it and I'm not sure I want to.' He has no current quit date and has never seriously attempted cessation. Which stage of the Transtheoretical Model is he in, and what is the most appropriate counselling approach?
A. Action stage — prescribe varenicline and schedule a quit date within the next 2 weeks
B. Contemplation stage — use motivational interviewing to explore ambivalence and the reasons he might consider quitting
C. Preparation stage — provide a full cessation plan with NRT and behavioural support
D. Maintenance stage — focus on relapse prevention strategies
Reveal Answer
Answer: B. Contemplation stage — use motivational interviewing to explore ambivalence and the reasons he might consider quitting
This patient is in the CONTEMPLATION stage — he has some awareness ('I know I should quit') but is ambivalent and has no plan to act ('I'm not sure I want to'). The Transtheoretical Model classifies patients based on intention to change. Contemplators are considering change but are not ready to commit. The appropriate approach is motivational interviewing (MI) — a non-confrontational, patient-centred technique that explores the patient's own ambivalence and values to elicit internally generated motivation. Prescribing NRT or varenicline to a non-ready patient is premature and leads to poor uptake and immediate abandonment. Aggressive directives ('you must stop smoking') cause reactance and entrench resistance. MI is the evidence-based communication strategy for this stage.
Smoking Cessation Counselling: The 5As Framework
The 5As framework (Ask, Advise, Assess, Assist, Arrange) is the evidence-based, guideline-recommended structured approach to smoking cessation counselling in clinical practice — competency IM28.20. It is designed for time-constrained clinical encounters: even the first two steps ('Ask' and 'Advise') alone — a brief 30-second intervention — double the rate of cessation attempts. The full 5-step framework takes 5–10 minutes and significantly further improves outcomes.
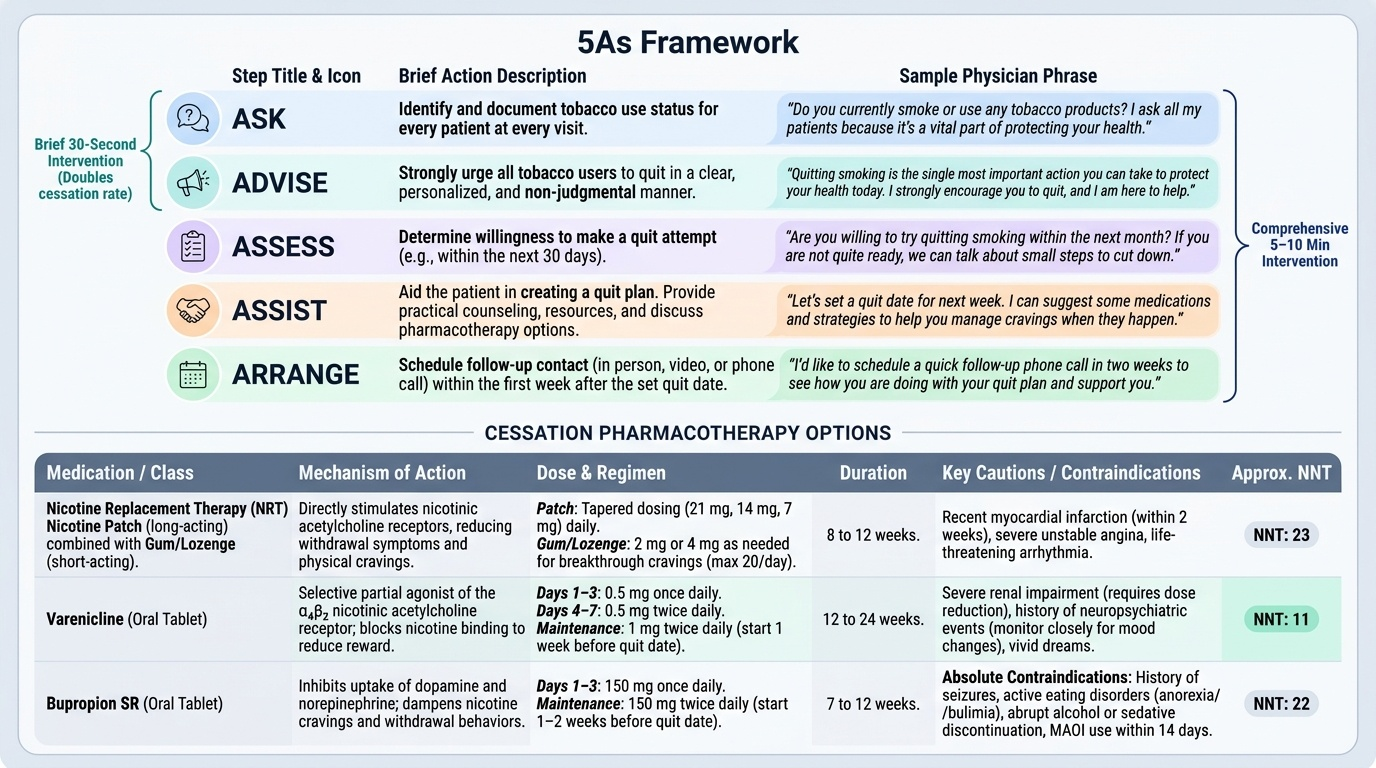
Provided image
Step 1 — Ask: At every patient encounter, systematically ask every patient about current tobacco use. In India, tobacco use extends beyond cigarettes to bidi (which delivers 3–5× more tar and nicotine than cigarettes and accounts for the majority of tobacco-related COPD in India), smokeless tobacco (khaini, gutkha, paan masala — associated with oral cancer, hypertension, and nicotine dependence), and hookah (particularly among young adults, often misperceived as safe). Document tobacco status in the medical record at every visit — 'smoker', 'ex-smoker (year quit)', or 'never smoker' — and update it.
Step 2 — Advise: Provide clear, strong, personalised non-judgmental advice to all current users. The word 'strong' and 'personalised' are key: advice that is generic ('smoking is bad for you') is less effective than advice that is specific to the patient's clinical situation ('The main reason your FEV1 has fallen by 200 mL in the past year is your smoking. Stopping now will slow this deterioration significantly'). Keep the tone non-judgmental — shame and blame are counterproductive and reduce likelihood of future engagement.
Step 3 — Assess: Assess willingness and readiness to quit. Use open questions: 'Have you thought about quitting smoking?' 'On a scale of 1 to 10, how ready do you feel to make a quit attempt in the next month?' Assess degree of physical dependence — Fagerström Test for Nicotine Dependence (FTND): time to first cigarette of the day is the single most reliable predictor of dependence level (within 5 minutes = very high dependence); and how many cigarettes per day. High dependence (FTND ≥6, first cigarette within 5 minutes) = requires pharmacotherapy, not just willpower alone.
Step 4 — Assist: For patients willing to make a quit attempt: set a quit date (within 2 weeks — more specific and proximate quit dates have higher success rates than vague intentions); provide counselling; prescribe pharmacotherapy:
- Nicotine Replacement Therapy (NRT): patch (16 or 24 hour; size graded to cigarette consumption), gum/lozenge (short-acting, used for breakthrough cravings), combination patch + gum recommended for high dependence. Safe in CVD patients (nicotine dose from NRT is lower than from smoking, without the CO and oxidants). Safe in asthma. Use for minimum 8–12 weeks.
- Varenicline (Champix/Chantix): partial agonist at α4β2 nicotinic receptors; reduces cravings, attenuates withdrawal symptoms, and reduces reward from breakthrough smoking. Most effective pharmacotherapy for cessation (NNT approximately 5). Start 1 week before quit date; dose-titrated over first week (0.5 mg OD → 0.5 mg BD → 1 mg BD). Contraindicated in severe renal impairment. Monitor for neuropsychiatric side effects (the FDA black-box warning was removed in 2016 after EAGLES trial showed comparable risk to NRT; still document baseline mental health status).
- Bupropion SR: dopamine-noradrenaline reuptake inhibitor, originally an antidepressant; reduces withdrawal symptoms and craving; particularly useful in patients with co-existing depression or ADHD; start 1–2 weeks before quit date; 150 mg OD for 3 days then 150 mg BD; avoid in seizure disorders, anorexia, bulimia, MAOIs.
- Combination pharmacotherapy (varenicline + NRT patch) produces the highest quit rates in severe dependence.
Step 5 — Arrange follow-up: Schedule a follow-up appointment within 1–2 weeks after the quit date — this is the highest-risk period for relapse. Subsequent contacts at 1 month and 3 months. Brief relapse counselling: 'A relapse does not mean you have failed — most successful quitters take several attempts. What we can learn from each attempt is what triggers caused the relapse, and we can prepare better strategies for those specific triggers next time.'
Referral: Refer to a tobacco cessation clinic for high-dependence patients or those with multiple failed attempts. iQUITIN is India's national tobacco cessation app (government-supported); National Tobacco Quitline 1800-11-2356 is a free toll-free service.
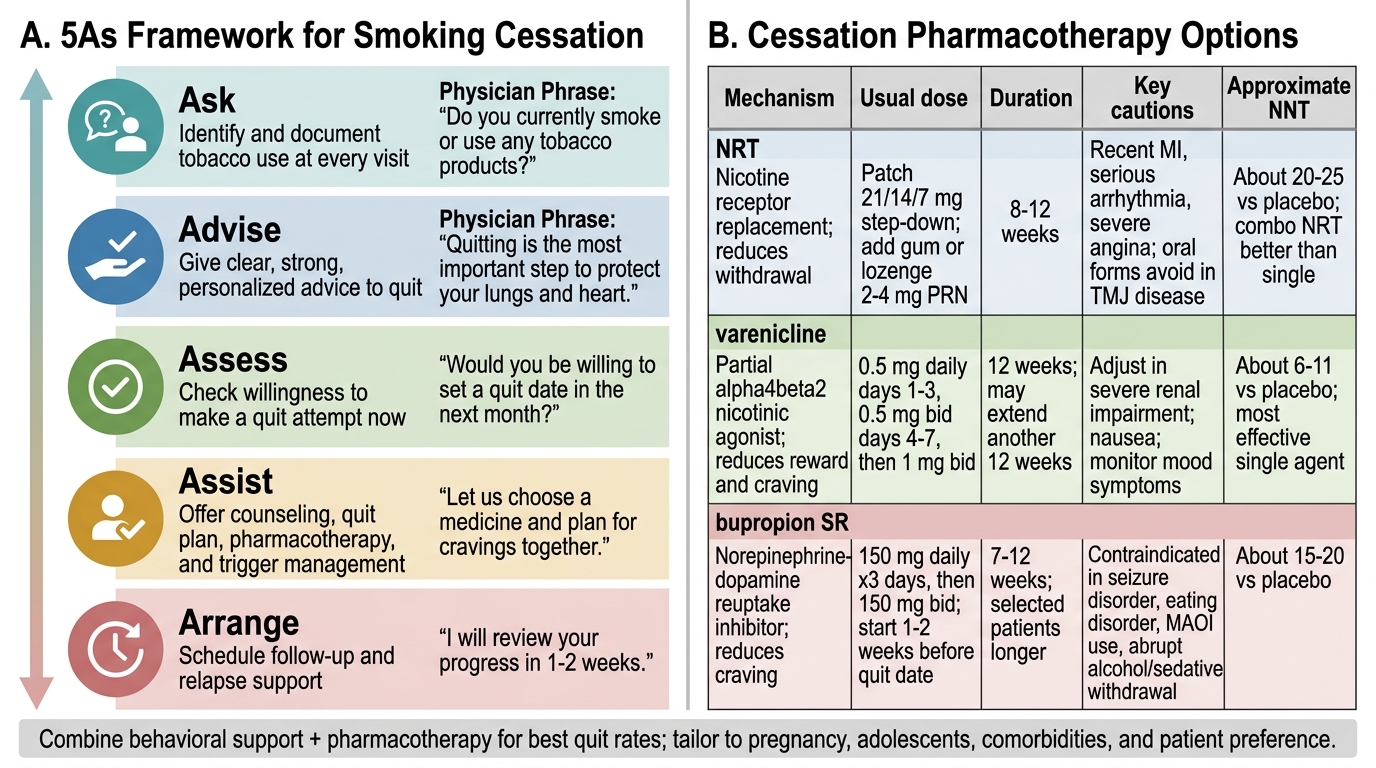
Smoking Cessation: 5As Framework and Pharmacotherapy