Page 15 of 22
IM28.{20,23-26} | Obstructive Airway Disease Prevention and Patient Context — SDL Guide (Part 2)
Workplace Preventive Measures for Occupational OAD
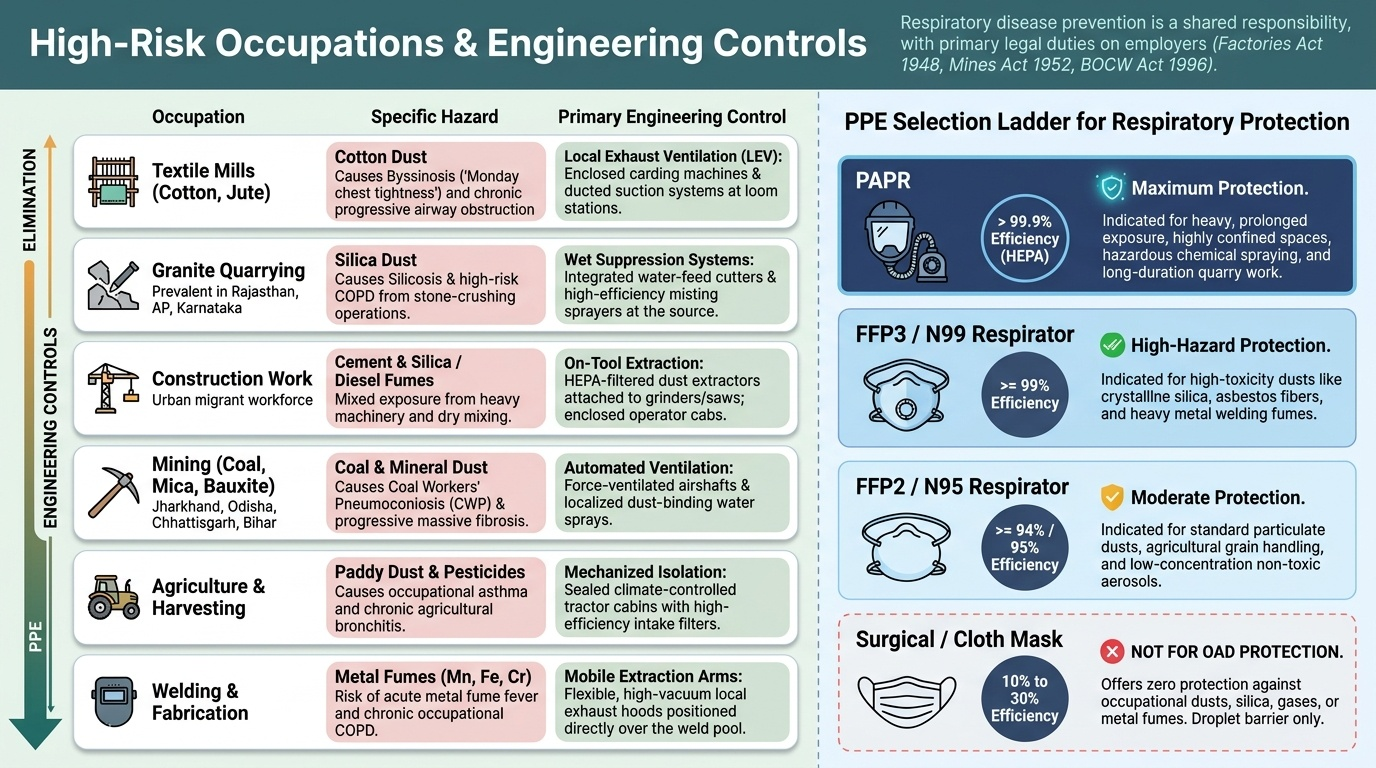
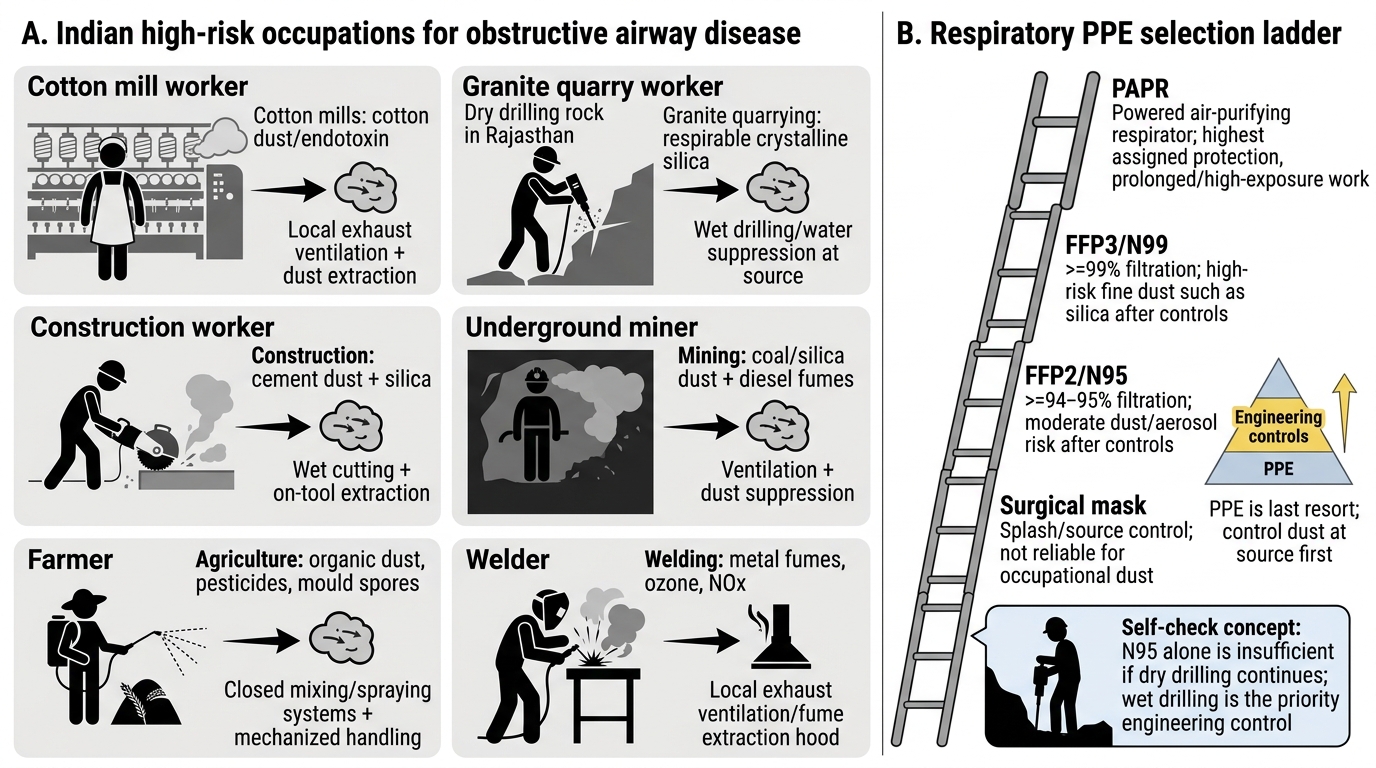
Occupational exposure to dusts, gases, and fumes is a major cause and exacerbator of both asthma and COPD in India — competency IM28.24. As a physician, you will encounter patients whose respiratory disease is occupationally caused or aggravated, and you will advise individual patients, employers, and public health authorities on preventive measures. Understanding the landscape of workplace OAD risk and the hierarchy of controls enables evidence-based occupational health advice that goes beyond the reflex of prescribing a mask. The fundamental principle is that respiratory disease prevention in the workplace is a shared responsibility between employer and employee — and that the legal framework (Factories Act 1948, Mines Act 1952, Building and Other Construction Workers Act 1996) places the primary duty on the employer to provide a safe working environment, not on the worker to protect themselves with personal equipment alone.
Provided image
High-risk occupations in India:
- Textile mills (cotton, jute, synthetic fibres): cotton dust causes byssinosis (Monday chest tightness); chronic occupational asthma with progressive obstruction; affects millions of loom operators
- Granite quarrying and stone cutting: silica dust inhalation causes silicosis + increased COPD risk; one of the highest-exposure occupations in India; prevalent in Rajasthan, Andhra Pradesh, Karnataka
- Construction work: cement dust, silica, diesel fumes from heavy machinery; major burden in urban migrant workers
- Agriculture: paddy dust, pesticide spray, harvesting biomass; agricultural workers in India have high rates of chronic bronchitis, often unrecognised
- Welding and metal fabrication: metal fumes (manganese, iron, chromium); risk of metal fume fever (acute) and siderosis/COPD (chronic)
- Mining (coal, mica, bauxite): coal workers' pneumoconiosis + COPD; coal mines in Jharkhand, Odisha, Chhattisgarh; mica mines in Bihar
- Bakeries and food processing: flour dust occupational asthma is one of the commonest occupational asthmas in food service workers
Engineering controls — the evidence base:
Engineering controls are more effective and more durable than administrative or PPE approaches because they remove or reduce the hazard at source. Key examples:
- Local exhaust ventilation (LEV): ducted systems placed close to the dust/fume-generating process capture particles before they disperse into the breathing zone; standard in well-run metalworking shops but rare in small-scale Indian workplaces
- Wet dust suppression: wet drilling (water injected at the drill bit) and water sprays at quarry faces reduce silica dust generation by 80–90% compared to dry operations
- Enclosed processes: fully enclosed cutting or grinding operations with exhaust ventilation; applicable in large-scale manufacturing
- General dilution ventilation: air changes per hour to dilute airborne contaminants; less effective than LEV but applicable when spot controls are not feasible
Administrative controls:
- Job rotation: limits duration of individual exposure by rotating workers between high-exposure and low-exposure tasks
- Work practice guidelines: standard operating procedures that minimise dust generation (using vacuum cleaners rather than dry sweeping, avoiding blowing compressed air over dusty surfaces)
- Exposure monitoring: periodic industrial hygiene surveys to measure airborne contaminant concentrations and verify that engineering controls are effective; mandatory under Indian Factories Act 1948 and Mines Act 1952 in regulated industries
Respiratory Protective Equipment (RPE):
As the last resort in the control hierarchy, RPE protects the individual worker when hazard controls are incomplete or not feasible. Types:
- Disposable particulate respirators (FFP2, FFP3): N95/FFP2 = minimum 94% filtration efficiency for particles ≥0.3 mcm; FFP3 = 99.9%; appropriate for silica, cotton dust, grain dust
- Half-face respirators with combination cartridges: for gas + particle mixtures (organic vapours + particulates in spray painting, pesticide application)
- Powered air-purifying respirators (PAPR): motorised blower draws air through a HEPA filter; positive pressure — no fit-seal dependency; suitable for high-exposure intermittent tasks
- Limitations of RPE in Indian workplaces: incorrect selection (surgical masks used for silica — completely ineffective); poor fit (beards, improper sizing); heat discomfort in tropical working conditions leading to removal; lack of employer provision; no training on proper donning, doffing, or seal-checking
Occupational health surveillance:
Pre-employment spirometry establishes a baseline; periodic spirometry (annually for high-risk workers, biannually for moderate-risk) enables early detection of occupational lung disease before progression to irreversible obstruction. Health screening should include symptom questionnaires (MRC dyspnoea, work-related wheeze) and chest radiograph where appropriate. Workers diagnosed with occupational asthma should be considered for redeployment away from the causative exposure — continuing exposure after diagnosis of occupational asthma causes progressive irreversible obstruction.
Occupational OAD: Hazards, Engineering Controls, and Respiratory PPE
SELF-CHECK
A 45-year-old granite quarry worker in Rajasthan presents with progressive breathlessness and reduced FEV1. He has never smoked. He has worked in dry drilling operations for 18 years without any respiratory protection. His employer now proposes to give all workers N95 masks. From an occupational health perspective, what is the most important limitation of this approach?
A. N95 masks are ineffective against crystalline silica particles — FFP3 masks must be used instead
B. PPE is the last resort in the hierarchy of controls; the employer should first implement wet drilling (engineering control) to suppress dust at source before relying on personal protective equipment
C. Respiratory protection is unnecessary if workers are physically healthy and have no respiratory symptoms
D. Administrative controls such as job rotation are more effective than any form of respiratory protection
Reveal Answer
Answer: B. PPE is the last resort in the hierarchy of controls; the employer should first implement wet drilling (engineering control) to suppress dust at source before relying on personal protective equipment
This question tests the hierarchy of hazard controls. While N95/FFP2 respirators provide adequate filtration for crystalline silica particles, the fundamental problem is that the employer is applying PPE — the last resort in the control hierarchy — rather than first implementing engineering controls. Wet drilling (injecting water at the drill bit to wet the crystalline silica as it is released) is an established engineering control that reduces airborne silica concentrations by 80–90%. Engineering controls protect all workers simultaneously and do not depend on individual compliance, mask fit, or heat-related removal. PPE should be used as an adjunct to — not a substitute for — engineering and administrative controls. Under the Mines Act 1952, silica-dust-exposed workers in Indian mines are legally entitled to periodic health surveillance including spirometry.
Understanding Patients' Environmental Constraints
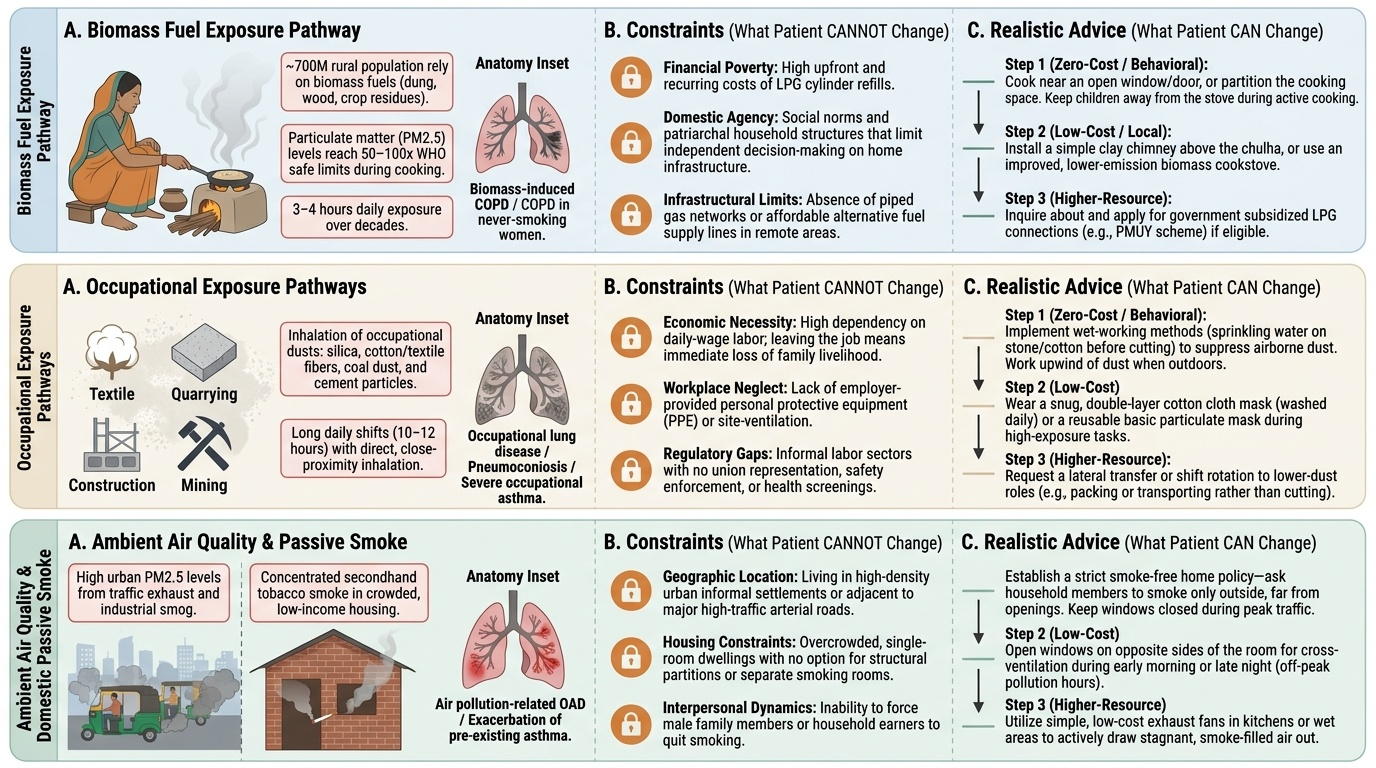
One of the most important clinical skills in managing OAD is the ability to read the patient's situation with accuracy and empathy — to understand what they can realistically change and what they genuinely cannot, and to avoid the trap of prescribing behaviour change advice that is technically correct but practically impossible given the patient's circumstances. This is competency IM28.25 — and it is tested not just by what you say to a patient but by the quality of your understanding.
Provided image
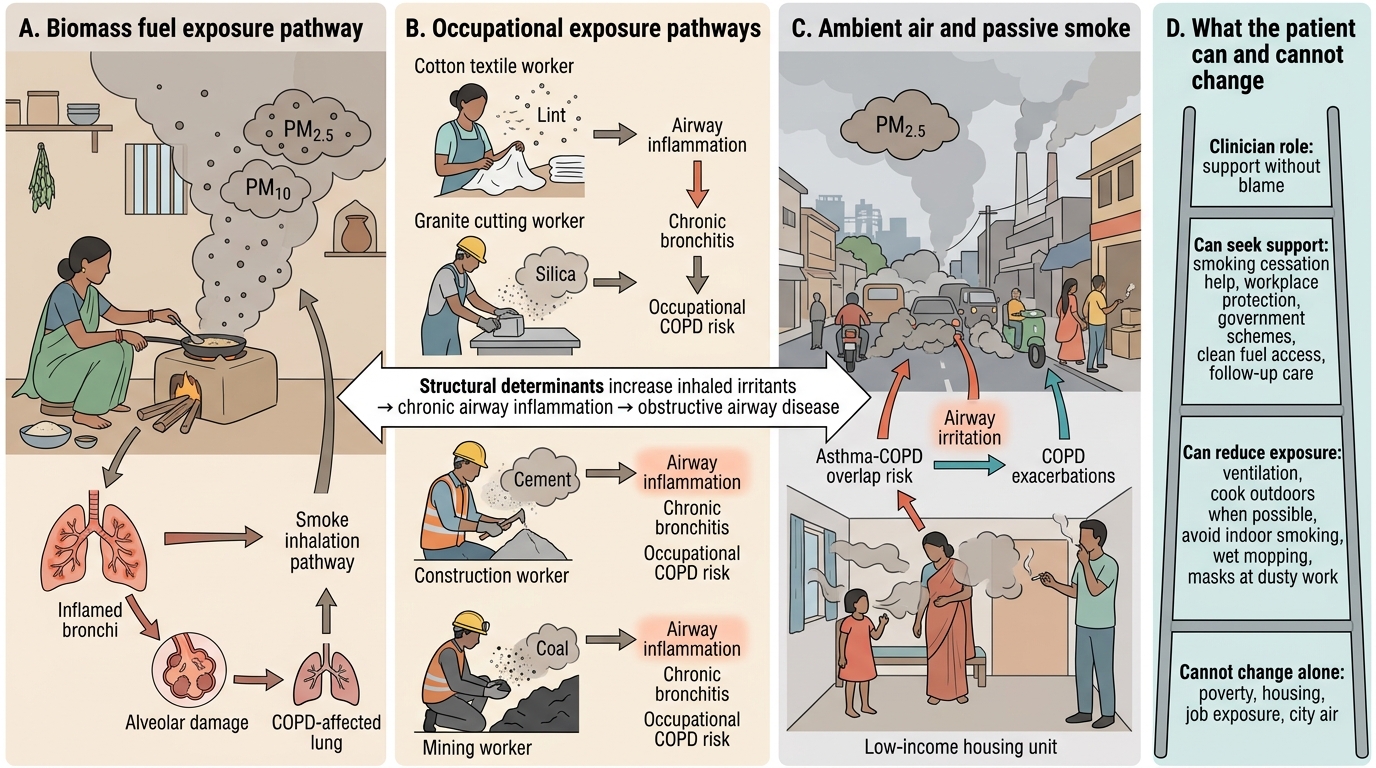
The structural determinants of indoor air pollution:
Approximately 700 million people in rural India use biomass fuels (wood, crop residues, cow dung) as their primary cooking fuel. The women who cook over traditional chulhas (cooking stoves) are exposed to particulate matter concentrations 50–100 times WHO safe limits, for 3–4 hours per day. This exposure causes chronic bronchitis, COPD, and lung cancer — even in never-smokers. The NMC term 'biomass fuel COPD' or 'COPD in never-smoking women' specifically refers to this pathway.
Asking a rural woman cooking on a chulha to 'improve your kitchen ventilation' or 'switch to LPG' is only clinically appropriate if she has the financial means and social agency to do so. LPG cylinder connections cost money that households below the poverty line do not have; improved chulhas reduce but do not eliminate exposure; social norms may restrict women's ability to make domestic infrastructure decisions independently. When you advise a patient on indoor air pollution reduction, you must first understand their household situation before issuing advice. Questions to ask: 'What fuel do you cook with?' 'Do you have a ventilation window or chimney?' 'Is LPG available and affordable in your area?' This information shapes advice that is actually actionable.
Occupational environmental constraints:
As illustrated with the cotton mill worker in the opening hook — a patient with occupational asthma caused by cotton dust cannot simply stop the exposure by 'changing jobs'. For many patients, their occupation IS their only livelihood, they have no transferable skills, their family depends entirely on their income, and informal sector work has no disability protection. Redeployment advice, though clinically correct, requires the patient to have an alternative — otherwise it condemns them to economic ruin to prevent respiratory deterioration. The physician's role here is: (a) document the occupational relationship clearly in the medical record (important for future disability assessment); (b) counsel on available protection within the current workplace (PPE, spacing from the worst exposure sources); (c) refer to an occupational medicine specialist or a social worker when feasible; (d) be honest with the patient that continuing exposure carries a known health cost, without hectoring or moralising.
Housing and ambient air quality:
Urban patients near industrial zones, highways, or brick kilns cannot easily 'move away'. Housing tenure in India is deeply constrained by affordability, lease agreements, and family ties. Acknowledging this reality — 'I understand that moving is not a simple option' — builds trust and opens a productive conversation about what modifications are feasible (closing windows during peak pollution hours, using exhaust fans, N95 masks during commuting during high-pollution episodes). Air quality index apps (SAFAR in India) can be recommended so patients can time outdoor exertion for lower-pollution windows.
The clinical attitude required:
Competency IM28.25 requires 'understanding' — not just knowing the facts about environmental constraints, but demonstrating empathy and avoidance of judgement. The critical clinical shift is from the default medical posture ('you should change your environment') to a contextual posture ('let us work with what is actually possible in your situation'). This means:
- Asking about living and working conditions before making environmental recommendations
- Calibrating advice to what is genuinely feasible
- Acknowledging barriers explicitly — 'I know switching to LPG is not straightforward'
- Focusing on what the health system CAN provide: better medication, written action plans, vaccinations, early exacerbation recognition
- Advocating for systems change — referring to social services, writing occupational health reports, supporting PMUY (Pradhan Mantri Ujjwala Yojana — government LPG scheme for BPL households) referrals
Structural Determinants of Obstructive Airway Disease in India
Understanding Difficulties in Smoking Cessation
Competency IM28.26 asks you to 'demonstrate an understanding for the difficulties faced by patients during smoking cessation' — this is not a pharmacology question. It is a question about professional compassion, realistic clinical expectations, and the skill of supporting patients through repeated attempts without shifting blame onto them. Smoking cessation is one of the most difficult behaviour changes a person can make, and understanding WHY it is difficult — biologically, psychologically, and socially — transforms the clinical encounter from a compliance lecture into a therapeutic partnership.
The neurobiology of nicotine addiction:
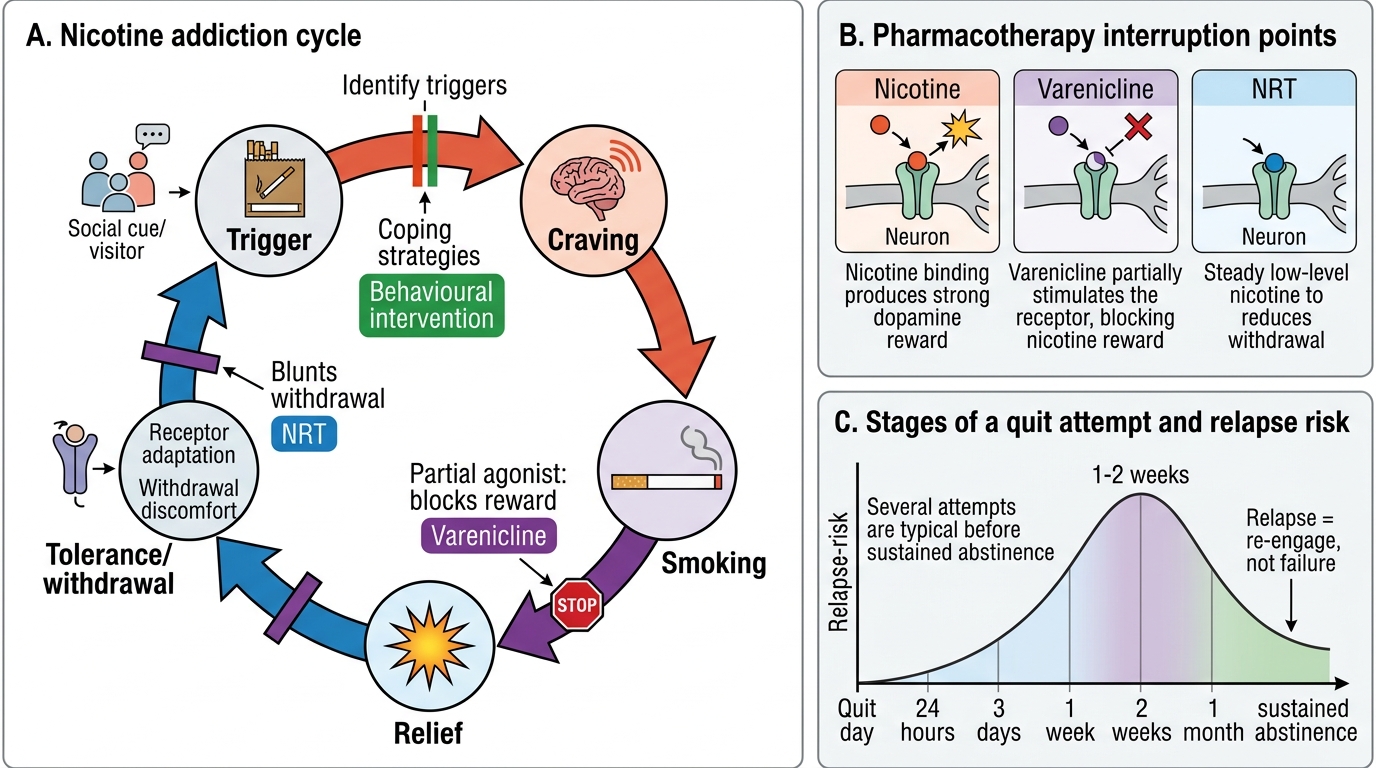
Nicotine reaches the brain within 10 seconds of inhalation — faster than any intravenous drug — and binds α4β2 nicotinic acetylcholine receptors in the nucleus accumbens, triggering dopamine release and producing a brief but intense rewarding effect. With repeated exposure, the brain upregulates the number of nicotinic receptors to compensate — meaning progressively more nicotine is needed to maintain normal dopamine signalling, and absence of nicotine leads to an acute dopamine deficit (withdrawal syndrome). The Fagerström criteria capture two key markers of severe dependence: lighting the first cigarette within 5 minutes of waking (reflecting overnight withdrawal and morning dopamine craving) and smoking more than 20–30 cigarettes per day. From a purely neurobiological standpoint, nicotine addiction is as powerful as opioid dependence in terms of the difficulty of withdrawal — telling a patient with FTND ≥7 to 'just stop' is analogous to asking an opioid-dependent patient to stop without substitution therapy.
Psychological and behavioural barriers:
Smoking is deeply conditioned into daily routines — the morning cigarette with tea, the post-meal smoke, the cigarette during a work break, the bidi shared among colleagues at a construction site. Each of these is a conditioned stimulus-response association built over decades. Cigarettes are also a coping mechanism for stress, anxiety, and emotional distress — many patients report that smoking is the only reliable strategy they have for managing difficult moments. Removing this coping tool without replacing it creates acute psychological discomfort that drives relapse within days of the quit date. Relapse most commonly occurs in the first 1–2 weeks and is triggered by stress, social exposure to other smokers, and negative affect.
Social and cultural barriers:
In communities where bidi smoking is culturally normal — shared during social interactions, offered as hospitality, embedded in occupational culture (farm workers, construction workers, fishermen sharing bidis during rest breaks) — quitting smoking means stepping outside a deeply embedded social practice. There is often significant peer pressure to continue smoking; ex-smokers who relapse describe the social comfort of returning as a powerful factor. For women who smoke or use smokeless tobacco — still stigmatised in many communities, making disclosure to the doctor difficult — there are additional barriers of shame and social disapproval. In households where the spouse continues to smoke, maintaining abstinence is genuinely very difficult: studies show that a non-smoking partner (or household smoke-free policy) is one of the strongest predictors of long-term cessation.
Economic barriers:
In India, bidi is far cheaper than cigarettes, and smokeless tobacco (khaini, gutkha) is extremely inexpensive and widely available. For patients in poverty, tobacco expenditure is a relatively affordable pleasure or stress-relief in an otherwise austere life — and NRT, though subsidised, still costs more than their daily tobacco expenditure. Varenicline is expensive for most patients in India (approximately ₹60–80 per tablet, total course ₹5,000–8,000). Cost of therapy is a real and recognised barrier to pharmacotherapy-assisted cessation.
The clinical implication — responding to relapse without blame:
Studies show that most smokers require an average of 8–10 quit attempts before achieving sustained 12-month abstinence. Each relapse is therefore not a failure of the patient's character but a predictable step in a typically iterative process. The clinical response that damages the therapeutic alliance is moralising: 'I told you to stop smoking — why did you start again?' The response that supports future attempts is exploratory and forward-looking: 'Tell me what happened — what triggered the relapse this time? Let us think about what we can prepare differently for your next attempt.' This shift from judgement to collaboration is the practical expression of competency IM28.26.
Nicotine Addiction Cycle and Cessation Support
SELF-CHECK
A 55-year-old man with GOLD 2 COPD made his sixth quit attempt 2 weeks ago with NRT patch alone. He has relapsed after his brother visited and they shared bidis. He looks ashamed and says, 'I'm hopeless. I can never stop.' What is the most therapeutically appropriate response?
A. Reinforce his pessimism: 'Six attempts is a lot — perhaps cessation is not realistic for you. Focus on your inhaler compliance instead.'
B. Express frustration: 'You know how important it is to stop — why do you keep starting again?'
C. Normalise relapse and re-engage: 'Most people need several attempts — this was actually a 2-week success. Tell me what triggered the relapse, and we will address that specifically for the next attempt, this time adding varenicline for better support.'
D. Discharge from cessation counselling and refer to a psychiatrist for addiction management
Reveal Answer
Answer: C. Normalise relapse and re-engage: 'Most people need several attempts — this was actually a 2-week success. Tell me what triggered the relapse, and we will address that specifically for the next attempt, this time adding varenicline for better support.'
Competency IM28.26 requires understanding of smoking cessation difficulties and appropriate empathic clinical response. The correct response normalises relapse (the average smoker requires 8–10 attempts before sustained abstinence), reframes the 2-week abstinence as success rather than failure, explores the specific relapse trigger non-judgementally, and offers a concrete improvement for the next attempt (adding varenicline — the most effective pharmacotherapy). Expressing frustration or pessimism damages the therapeutic relationship and reduces likelihood of future engagement. Referring to psychiatry is inappropriate for a patient with nicotine dependence who has not been trialled on first-line cessation pharmacotherapy. The 'hopeless' attribution the patient expresses is self-blame driven by shame — it is clinically counterproductive and should be gently corrected.