Page 16 of 22
IM28.{20,23-26} | Obstructive Airway Disease Prevention and Patient Context — SDL Guide (Part 3)
Applied Practice: Integrating Prevention and Context
The three patients from the opening hook return — now apply the competencies from this module to their care. This section illustrates how the principles of behaviour change, occupational health, empathic understanding of environmental constraints, and smoking cessation combine in real clinical scenarios.
Patient 1 — The cotton mill worker:
He cannot leave his job. Your applied practice responses: (1) Document the clear occupational relationship between cotton dust exposure and his airway disease in the medical record — this is the foundation of any future compensation or disability claim under the Employees' State Insurance (ESI) Act. (2) Counsel him on available in-plant protection: does his mill have LEV? If not, advise him in writing to request it from his employer (a medical recommendation carries weight in ESI inspection processes). (3) Prescribe an FFP2 respirator as a short-term protective measure and demonstrate proper fit. (4) Refer to an occupational medicine specialist for formal impairment assessment. (5) Do not advise him to 'change jobs' without exploring whether that is economically feasible — ask first, advise second. (6) Refer to an ESI social worker regarding disability benefit entitlement if lung function deterioration continues to impair work capacity.
Patient 2 — The woman with multiple quit failures:
The structural context: husband smokes at home, single-room dwelling (no smoke-free space), bidi is culturally normal, LPG unaffordable, low literacy. Applied responses: (1) Acknowledge the difficulty openly — 'Quitting when your husband smokes at home is genuinely very hard. That is not a character weakness — it is a real barrier.' (2) Assess Fagerström score — if first bidi within 5 minutes, high dependence; prescribe NRT combination (patch + gum) and explore CGHS/ESI coverage or generic NRT cost options; discuss Quitline 1800-11-2356 for free ongoing telephone support. (3) Explore whether the husband would consider a simultaneous quit attempt — couple-based cessation has higher success rates. (4) Assess feasibility of PMUY LPG connection and refer if not already enrolled. (5) Explore whether there is any part of the house or outdoor space where she spends time away from smoke — even partial smoke-free windows are protective.
Patient 3 — The engineer near an industrial corridor:
He is asking a rational clinical question: will moving help? Applied responses: (1) Answer honestly using the evidence: ambient air pollution is a documented exacerbation trigger and long-term risk modifier for asthma; if his move takes him significantly away from the industrial corridor, it is likely to be beneficial; there is real evidence supporting this. (2) In the interim, provide practical harm-reduction advice: SAFAR app for real-time air quality index, avoid outdoor exercise on high-pollution days, N95 mask for outdoor exposure on high-pollution episodes, ensure his home has adequate ventilation with air change when outdoor AQI is acceptable. (3) Recommend that his employer's relocation package include a letter documenting the health basis of the move — this may be relevant to negotiation with housing support.
What unites all three cases:
Each patient required you to ask before advising, to understand before prescribing, and to calibrate clinical guidance to what is actually achievable in the patient's reality. This integration of clinical knowledge with contextual empathy and social sensitivity is what transforms a technically competent doctor into a clinically excellent one.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
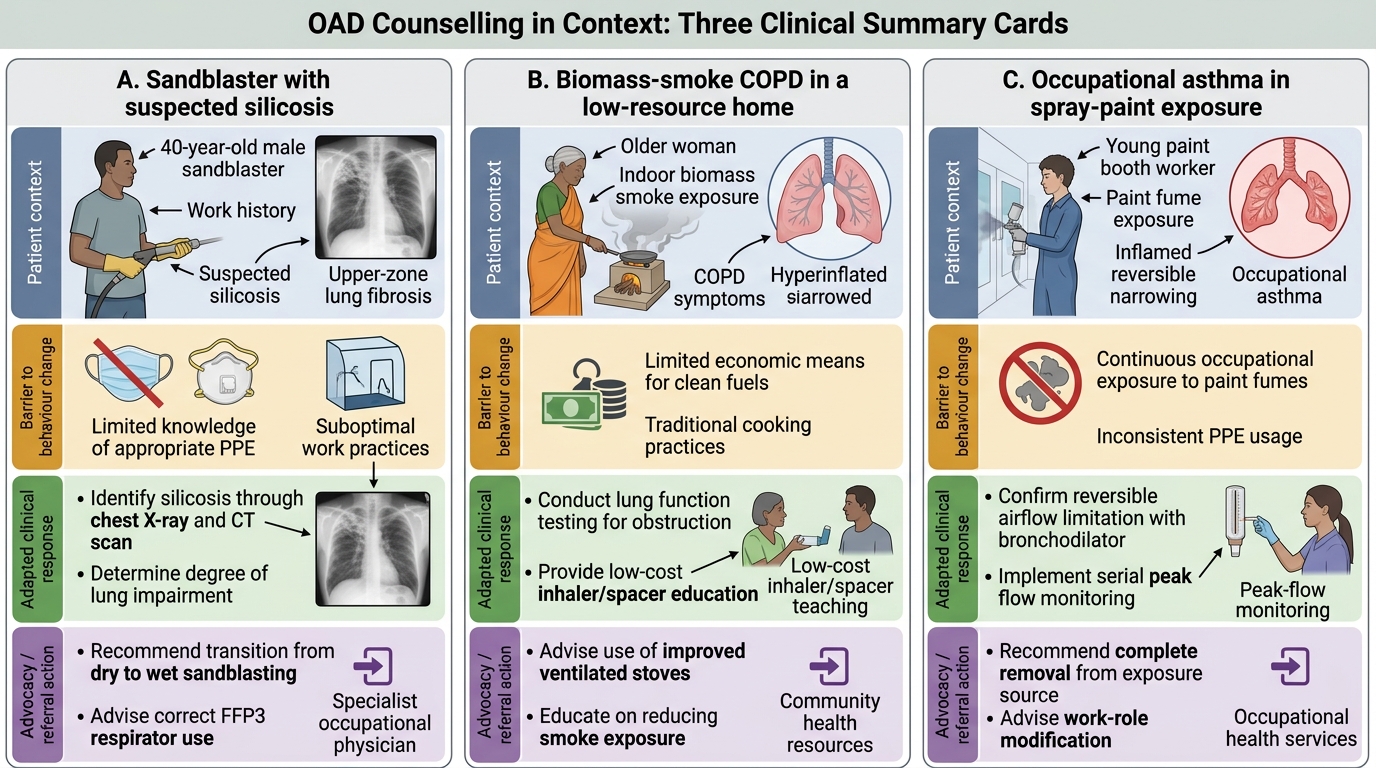
Context-Based OAD Counselling Summary Cards
Self-Assessment: Prevention and Context Scenarios
Apply the prevention and patient-context competencies from this module to the following clinical scenarios. For each, identify the correct clinical response and its rationale.
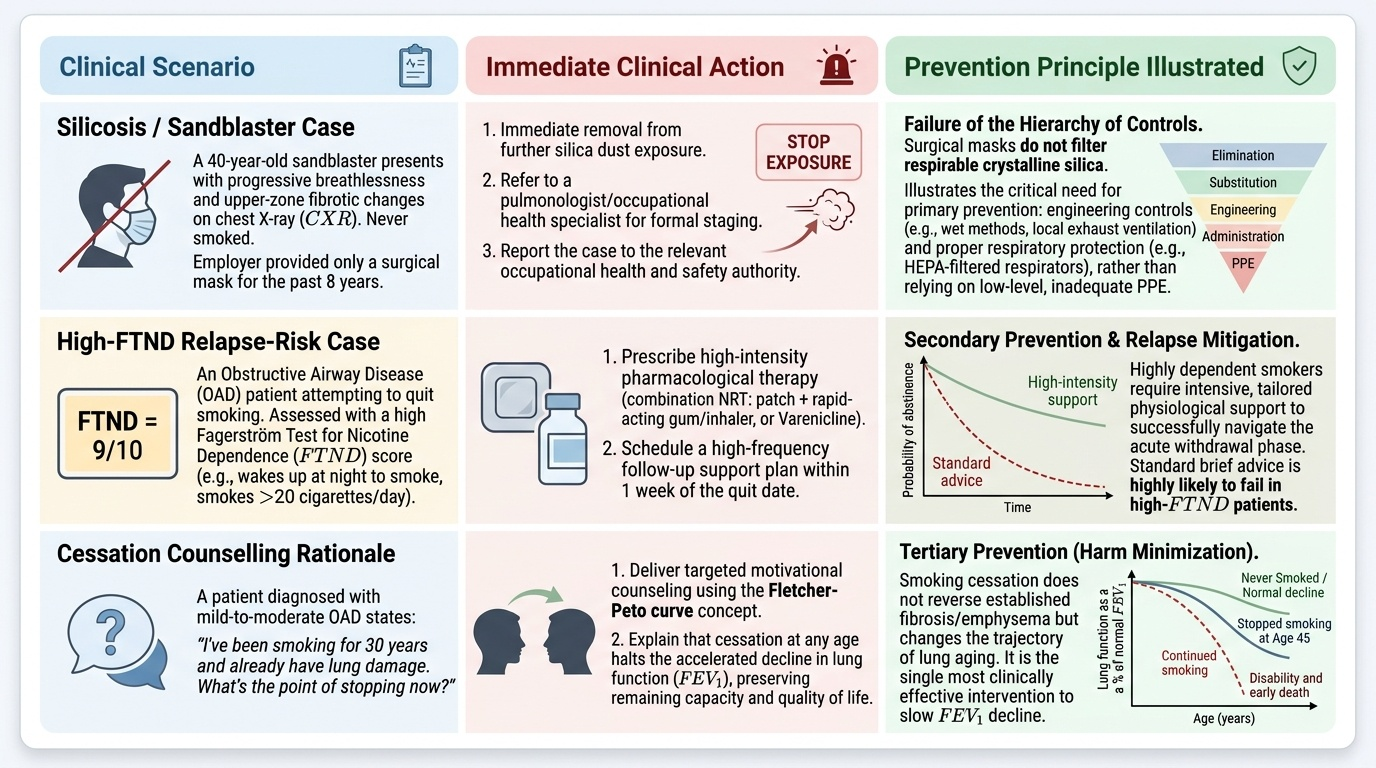
Provided image
Scenario A: A 40-year-old sandblaster presents with progressive breathlessness and upper-zone fibrotic changes on CXR. He has never smoked. His employer provided a surgical mask for the past 8 years. What is the most important clinical and occupational health response?
Analysis: This is suspected silicosis — upper-zone fibrosis in a sandblaster is silicosis until proven otherwise. Surgical masks provide zero protection against crystalline silica — FFP3 is the minimum standard, but the key occupational health lesson is that engineering controls (wet abrasive blasting, process enclosure) should have been the primary approach. Document the occupational exposure; refer to pulmonologist for HRCT and formal diagnosis; notify the occupational safety authority (DGFASLI); refer for ESI disability assessment. Patient counselling: silicosis is irreversible but further exposure must be stopped — support a disability compensation claim if employment ends.
Scenario B: During a COPD review, a 52-year-old man says he stopped smoking 2 months ago — his fifth attempt — but looks uncertain about confidence. Baseline FTND was 8. He is on NRT patch alone. What do you do next?
Analysis: FTND 8 = very high physical dependence; NRT patch alone has lower success rates for high-dependence patients. Two months is still within the high-risk relapse window. Appropriate response: (1) Reinforce the 2-month success — significant given FTND 8; (2) Escalate pharmacotherapy: add short-acting NRT gum for breakthrough cravings AND consider adding varenicline, which is more effective than NRT alone for high-dependence patients; (3) Explore emerging triggers or social pressures; (4) Schedule review at 3 months.
Scenario C: A colleague says: "I never counsel COPD patients about smoking — they will just relapse anyway." How do you respond?
Analysis: Relapse is the rule, not the exception (8–10 attempts average before sustained abstinence); brief physician advice alone doubles cessation attempt rates; pharmacotherapy substantially increases per-attempt success. The appropriate practice is to apply the 5As at every visit — even Ask + Advise in 30 seconds — because each attempt builds toward eventual success. Therapeutic nihilism about cessation is a modifiable barrier that costs patients years of lung function and life expectancy.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
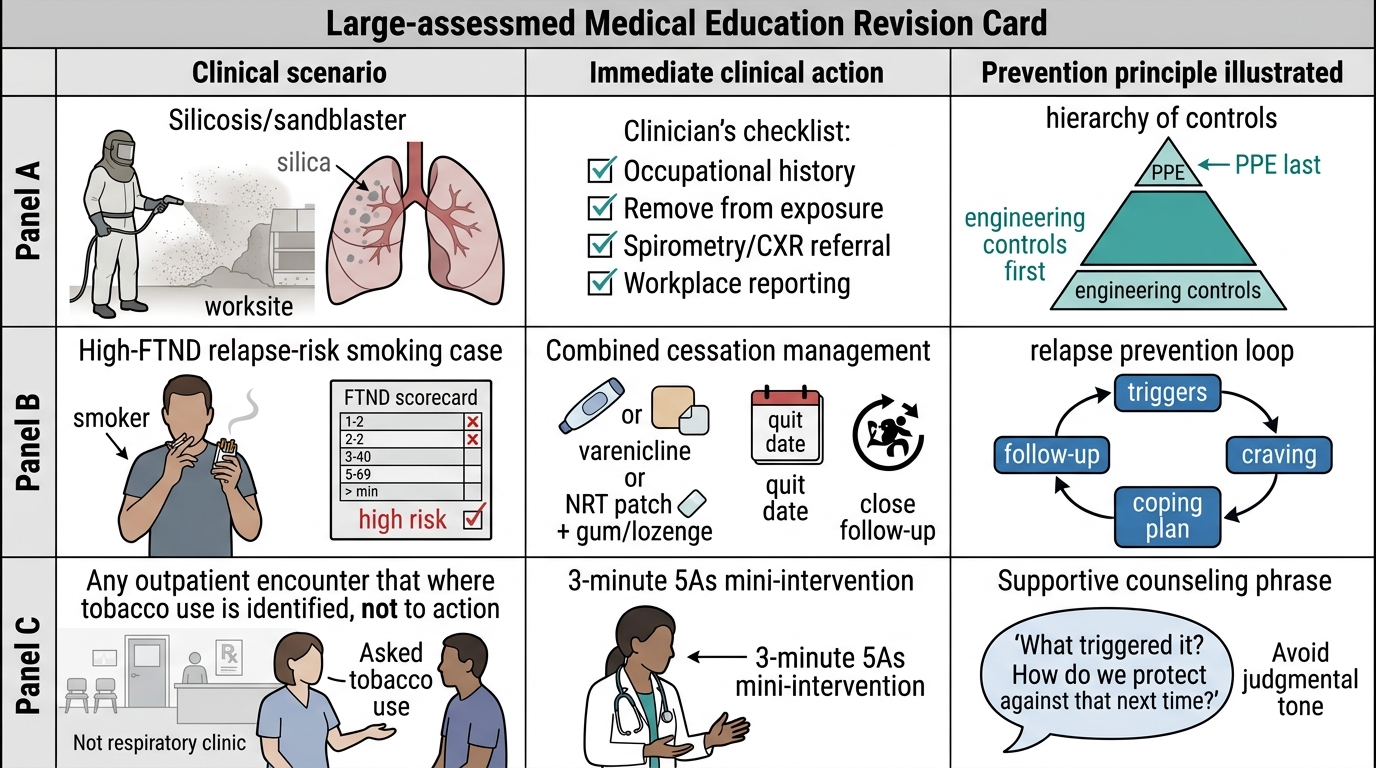
OAD Prevention: OSPE Self-Assessment Card
CLINICAL PEARL
Three prevention pearls for OAD: First, the 5As framework works even in 3 minutes — Ask every patient about tobacco at every visit (not just respiratory patients), Advise clearly and personally, Assess readiness — this minimal intervention alone doubles cessation attempt rates. Second, PPE is the last resort, not the first response in occupational OAD — always ask whether engineering controls (wet drilling, local exhaust ventilation) are in place before defaulting to recommending masks, which protect only the individual and depend entirely on correct use. Third, relapse is the rule, not the exception in smoking cessation — the average patient needs 8–10 attempts; your clinical response to relapse should be curious and forward-looking ('what triggered it, how do we protect against that next time?'), not judgmental ('why did you start again?').