Page 7 of 20
IM29.{11,15,23} | Lifelong Learning and Information Technology — SDL Guide
Learning Objectives
- Explain why lifelong learning is a professional obligation for every practising physician, not an optional aspiration (IM29.11, IM29.23)
- Describe the principal strategies for self-directed continued learning including CME requirements, reflective practice, and scholarship (IM29.23)
- Demonstrate appropriate use of information technology for patient care, clinical decision support, and continued education (IM29.15)
- Apply evidence-based resources (clinical guidelines, databases, clinical decision support tools) accurately in clinical decision-making
- Identify the regulatory framework for Continuing Medical Education (CME) in India under the NMC Act 2020
INSTRUCTIONS
The medical knowledge base doubles roughly every 73 days (Densen, 2011, Clinical Medicine & Research). The physician who stops learning the day they graduate is practising increasingly obsolete medicine within years. This module develops the frameworks, habits, and digital skills to sustain effective lifelong learning throughout a medical career — and to use information technology in ways that genuinely improve patient care rather than creating new risks.
References
- NMC Competency Based Medical Education Curriculum — IM29 (Physician in the Community) (guideline)
- NMC Continuing Medical Education Regulations, 2023 — CME credit requirements for registration renewal (guideline)
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 4 — Ethical Issues in Clinical Medicine (textbook)
- Sackett DL, Richardson WS, Rosenberg W, Haynes RB — Evidence-Based Medicine: How to Practice and Teach EBM, 2nd ed. (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 1970, a physician who memorised the content of Harrison's Principles of Internal Medicine could reasonably claim to know most of what was clinically knowable. Today, Harrison's runs to over 4,000 pages and a 21st edition that has been substantially rewritten since the 20th. The guidelines for managing type 2 diabetes have been revised four times in the past decade. The drugs of choice for heart failure changed fundamentally with the DAPA-HF trial in 2019, the EMPEROR-Reduced trial in 2020, and the PARADIGM-HF data before them — all of which postdate the training of any physician who qualified before 2015. The NTEP (National TB Elimination Programme) moved from intermittent thrice-weekly regimens to daily fixed-dose combinations — a change that any physician prescribing tuberculosis treatment must know. Here is the hard question this module begins with: when did you last check whether what you know about managing a common condition is actually current? Not a textbook you read in second year — but a guideline published in the last 24 months that might change what you do tomorrow morning on the ward?
WHY THIS MATTERS
Lifelong learning and information technology (IM29.11, IM29.15, IM29.23) are SH (Skill/Habit) level competencies in the NMC 2024 curriculum — meaning the examination board expects to see you demonstrate these behaviours, not just describe them. In practical terms, the OSCE assessor may hand you a patient scenario and ask you to find the current guideline recommendation using a clinical decision support tool — on the spot. The NMC Continuing Medical Education Regulations 2023 require registered practitioners to accumulate CME credits as a condition of maintaining their medical registration, signalling that the regulator views continued learning as a regulatory obligation, not a personal choice. Beyond examinations, the professional and medico-legal case for continued learning is direct: a clinician who applies a treatment protocol that has been superseded by evidence of harm may be found negligent not for technical error but for failure to keep abreast of developments — a standard Indian consumer courts and medical disciplinary bodies have applied.
RECALL
Before proceeding, activate your prior knowledge. From your pharmacology training, recall the concept of evidence levels — Level 1 (systematic reviews and meta-analyses), Level 2 (randomised controlled trials), Level 3 (cohort and case-control studies), Level 4 (case series), Level 5 (expert opinion). From your community medicine training, recall the concept of health information systems and the role of surveillance data in public health. From your clinical years, recall moments when you needed to look up a drug dose, a diagnostic criterion, or a management algorithm — and the resource you used. Think about this: how reliable was that resource? Was it a textbook published ten years ago? A Wikipedia article? A point-of-care app on a colleague's phone that you could not verify? The quality of the clinical decision you made was contingent on the quality of the information you accessed. This module gives you the framework to make that access systematic and trustworthy.
Why Lifelong Learning Is a Professional Obligation
Lifelong learning in medicine is the commitment to systematically update knowledge, refine clinical skills, and develop professional judgment throughout a career — not as a response to examinations or renewal deadlines, but as an intrinsic expression of the obligation to provide competent care. The NMC curriculum describes this as a commitment to continued learning (IM29.11) and commitment to learning and scholarship (IM29.23), both at the SH (Skill/Habit) level — indicating that the goal is an ingrained professional behaviour, not a declarative knowledge statement.
The urgency of this commitment is not rhetorical. The half-life of medical knowledge — the time after which approximately 50% of what is known in a specialty becomes outdated or superseded — has been estimated at approximately 45 years for basic science knowledge and as short as 5–10 years for clinical practice guidelines in rapidly evolving fields such as oncology, cardiology, and infectious disease. An important empirical illustration: the Cochrane Systematic Review on oxygen therapy targets in critically ill patients (revised 2018) showed that liberal oxygen supplementation — the standard approach for decades — was associated with increased mortality, not decreased. Physicians trained before 2015 who had not updated their knowledge continued to deliver a practice that the evidence showed was harmful. This is not a hypothetical risk; it is a documented mechanism by which outdated practice causes harm.
The Indian regulatory framework for continued learning has been substantially strengthened under the NMC Act 2020 and the NMC Continuing Medical Education Regulations 2023. Under these regulations, registered practitioners are required to obtain a specified number of CME credit hours as a condition of renewing their registration. The CME credits can be accumulated through accredited activities including workshops, conferences, e-learning modules, journal clubs, and structured self-assessment tools. The NMC has established an online portal through which registered practitioners can track and submit CME credits. Failure to comply does not result in immediate deregistration but is a condition that can be flagged during registration renewal — an administrative mechanism designed to make lifelong learning a regulatory expectation, not merely an aspirational standard.
Beyond regulatory compliance, the epistemological obligation is more compelling: the physician-patient relationship is founded on the patient's reasonable assumption that the clinician's advice reflects current knowledge. When that assumption is violated — when a patient is given a treatment recommendation that reflects a guideline superseded four years earlier — the physician has not merely failed to keep up; they have implicitly misrepresented their competence. The ethical dimension is an extension of the beneficence principle: acting in the patient's best interest requires that the action be based on the best available current evidence.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
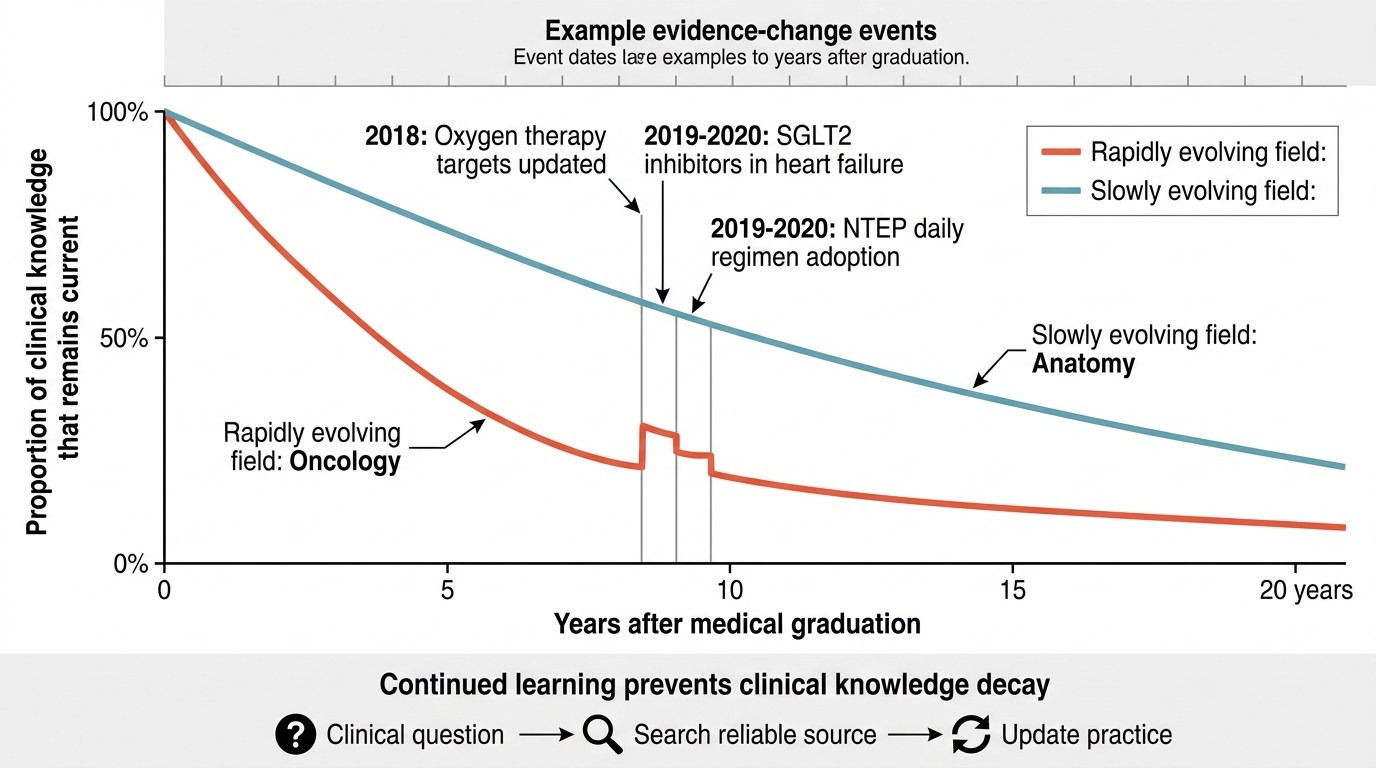
Knowledge Decay After Medical Graduation
Strategies for Effective Continued Learning: From Passive to Deliberate
Not all learning approaches are equally effective, and the transition from student to practitioner requires a conscious shift from the passive absorption model of medical school (attend lectures, read textbooks, pass examinations) to a deliberate, self-directed model anchored in real clinical questions. The research on expert performance — summarised by K. Anders Ericsson's concept of deliberate practice — shows that expertise in complex domains does not accrue automatically from experience; it requires focused, purposeful engagement with specific aspects of performance that need improvement, with feedback on the outcome. The physician who attends a CME conference, sits passively through ten lectures, and changes nothing about their clinical practice is technically fulfilling a regulatory requirement but not substantially learning. The physician who identifies a knowledge gap during a challenging patient encounter, formulates a specific question, searches a reliable resource, and applies the finding at the next relevant clinical opportunity is performing deliberate, practice-embedded learning. The difference between these two physicians, compounded over a 30-year career, produces a measurable divergence in clinical competence and patient outcomes — which is precisely why the NMC 2024 curriculum tests lifelong learning at the Skill/Habit level, not merely the Knowledge level.
For physicians, a practical framework for self-directed continued learning is the Practice-Based Learning and Improvement (PBLI) cycle, which has four stages:
- Identify a practice gap — recognise a clinical encounter in which your knowledge, skill, or judgment was insufficient or uncertain. This might be a diagnosis you were unsure of, a drug dose you had to look up, a complication you did not anticipate, or a patient question you could not answer confidently.
- Formulate a learning question — transform the clinical uncertainty into a structured learning question. The PICO format (Population, Intervention, Comparator, Outcome) is the standard tool for formulating evidence-based clinical questions. For example: 'In a patient with HFrEF (P) does the addition of an SGLT2 inhibitor (I) compared to standard GDMT alone (C) reduce cardiovascular death or worsening heart failure (O)?'
- Access a reliable resource — retrieve the best available evidence relevant to the question, evaluate its quality, and extract the clinically actionable finding.
- Apply and reflect — apply the learning to clinical practice and complete the loop by reflecting on whether it changed your management or understanding.
Formal structures for continued learning available to Indian physicians include:
- Journal club — regular group review of recent literature in a specialty; develops critical appraisal skills and collective knowledge update
- Morbidity and mortality (M&M) conference — structured case-based review of adverse events and near-misses; combines continued learning with quality improvement
- Grand rounds — formal departmental educational presentation, typically on a topic of current relevance
- CME workshops and conferences — accredited for NMC CME credits; most effective when they require active participation rather than passive attendance
- Case-based discussions (CBD) and directly observed procedural skills (DOPS) — formative assessments used in postgraduate training that also function as structured learning opportunities
- E-learning and point-of-care resources — discussed in detail in the next section
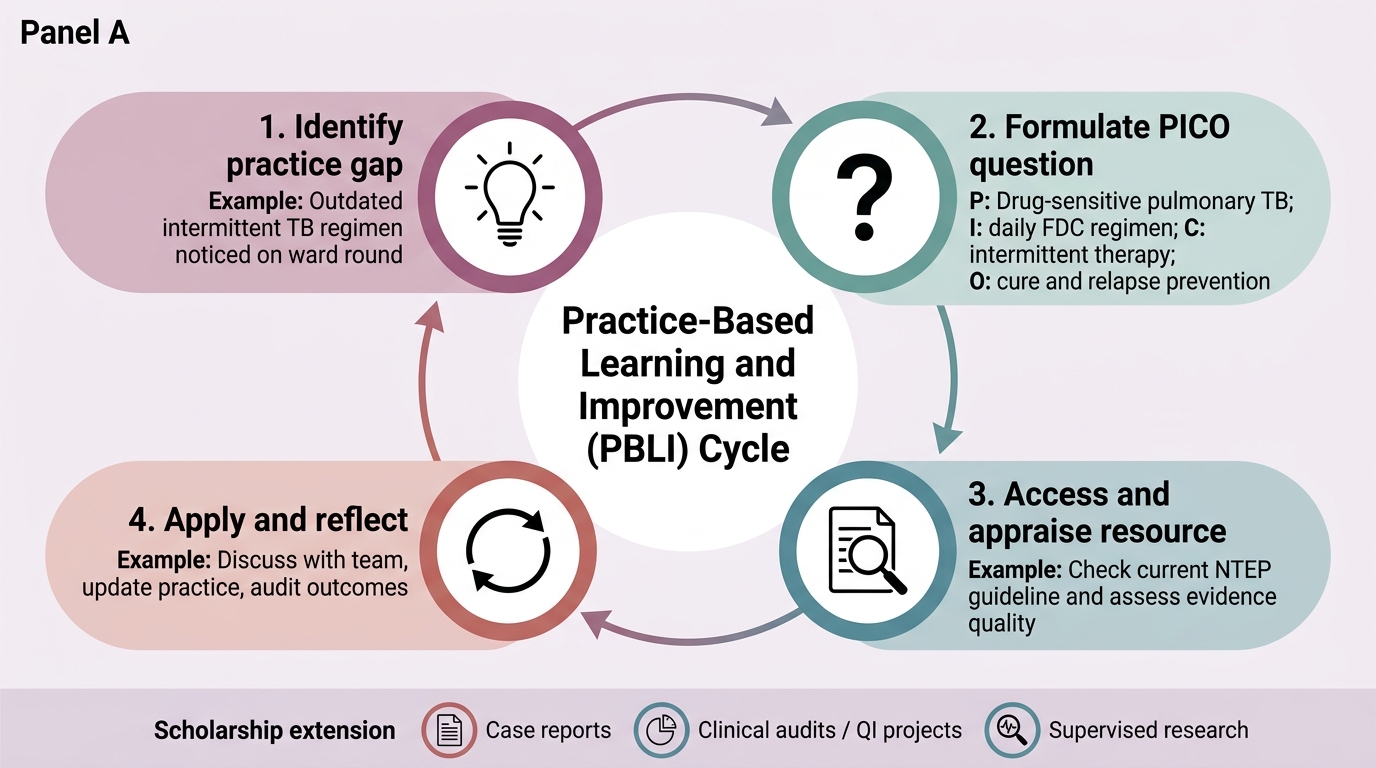
Practice-Based Learning and Improvement Cycle
Scholarship (IM29.23) extends the commitment beyond personal knowledge update to contribution to the knowledge base. At the final-year level, scholarship is demonstrated through participation in case reports, audits, quality improvement projects, and structured research under supervision — activities that develop the habits of systematic inquiry, evidence evaluation, and critical writing. The NMC curriculum includes research participation (IM29.26) as a specific competency for this reason. An Indian physician who understands only how to consume evidence — and not how to evaluate its quality or contribute to it — is a weaker practitioner than one who has developed both skills.
SELF-CHECK
During a morning ward round, a senior resident prescribes thrice-weekly intermittent TB therapy for a newly diagnosed drug-sensitive pulmonary TB patient. As a final-year student who has recently reviewed current NTEP guidelines, you recognise this may be outdated practice. Which of the following BEST describes the current NTEP-recommended regimen for drug-sensitive TB?
A. 2HRZE + 4HR thrice-weekly intermittent, all weight-band patients
B. 2HRZE + 4HRE daily, fixed-dose combinations, weight-band dosing
C. 2HRZ + 4HR daily with individual drug formulations
D. 3HRZE + 3HR daily for all adult patients regardless of weight
Reveal Answer
Answer: B. 2HRZE + 4HRE daily, fixed-dose combinations, weight-band dosing
The current NTEP (National TB Elimination Programme — formerly RNTCP) regimen for new drug-sensitive pulmonary TB is 2HRZE (intensive phase, 2 months: isoniazid, rifampicin, pyrazinamide, ethambutol) + 4HRE (continuation phase, 4 months: isoniazid, rifampicin, ethambutol), all administered daily using fixed-dose combinations (FDCs), with weight-band dosing. The old thrice-weekly intermittent regimen was phased out because daily therapy produces higher sputum conversion rates and lower acquired drug resistance. This is a key 'knowledge currency' point: any physician prescribing the old intermittent regimen is applying superseded practice. RNTCP is now NTEP (renamed in 2020). The regimen in option C omits ethambutol from the intensive phase.
Information Technology in Clinical Practice: Tools, Risks, and Standards
Information technology in clinical medicine has transformed both the delivery of care and the process of continued learning over the past two decades. The NMC competency IM29.15 requires that the final-year student demonstrate adequate knowledge and use of information technology for both appropriate patient care and continued learning — a dual mandate that reflects the two principal domains in which IT has clinical significance: at the point of care (clinical decision support, electronic prescribing, telemedicine) and at the point of learning (evidence databases, e-learning platforms, digital scholarship tools). This dual function is not a technicality — the quality of the IT tools a clinician uses and the skill with which they are used has direct, measurable consequences for patient outcomes. Studies comparing hospitals with high versus low UpToDate penetration have found significant differences in length of stay, rates of adverse drug events, and diagnostic accuracy. India is simultaneously building one of the world’s largest digital health infrastructures — the Ayushman Bharat Digital Mission — and navigating a healthcare system in which many district hospitals still lack reliable broadband. The final-year student must be competent at both ends of this spectrum: fluent with the most sophisticated clinical decision support tools, and resourceful enough to access good evidence in a low-connectivity setting. This section maps the landscape of clinically relevant IT, distinguishes reliable from unreliable resources, and addresses the safety risks that come with digital tools.
The categories of clinically relevant information technology available to the Indian physician in 2026 include:
Point-of-care clinical decision support (CDS) tools:
- UpToDate — a continuously updated evidence synthesis resource; widely considered the highest-quality peer-reviewed point-of-care reference; its recommendations are graded by evidence strength and updated every 4–6 weeks; studies have demonstrated that UpToDate use is associated with reduced length of stay and lower rates of adverse drug events in hospital settings
- Medscape Drug Interactions — for checking drug-drug, drug-disease, and drug-pregnancy interactions; important in a country where polypharmacy in elderly and multi-morbid patients is common
- MDCalc — a validated clinical calculator platform aggregating over 500 clinical scoring tools, from CHA₂DS₂-VASc (atrial fibrillation anticoagulation decision) to CURB-65 (pneumonia severity) to Child-Pugh (liver disease); each calculator includes the primary citation and validity data
- WHO Essential Medicines List and NTEP/NACO guidelines — freely accessible via WHO and government of India portals; the authoritative source for public health programme protocols
Evidence databases:
- PubMed/MEDLINE — the US National Library of Medicine's database of peer-reviewed biomedical literature; free access; essential for literature searches and evidence appraisal
- Cochrane Library — systematic reviews of clinical evidence; considered the highest level of evidence synthesis; full access available through some Indian institutions and the NLM
- NICE guidelines (UK) and Indian-specific clinical practice guidelines issued by professional bodies such as the API (Association of Physicians of India), RSSDI (diabetes), CSI (cardiology), INASL (liver)
Telemedicine and digital health:
- India's Telemedicine Practice Guidelines 2020 (issued by the Ministry of Health and Family Welfare and NMC) define the legal framework for telemedicine practice — who can practise, which consultations are permissible, what constitutes a valid telemedicine prescription, and documentation standards. Key provisions: registered practitioners only; synchronous video consultation for first-time prescribing of schedule H1 drugs; text/voice consultation permitted for follow-up; no schedule X drugs via telemedicine
- Electronic health records (EHR): under the National Digital Health Mission (ABDM — Ayushman Bharat Digital Mission), India is building a national digital health ecosystem with a unique health identifier (ABHA — Ayushman Bharat Health Account). Clinicians practising in ABDM-linked institutions will increasingly interact with linked EHRs; standards for interoperability are based on HL7 FHIR (Fast Healthcare Interoperability Resources)
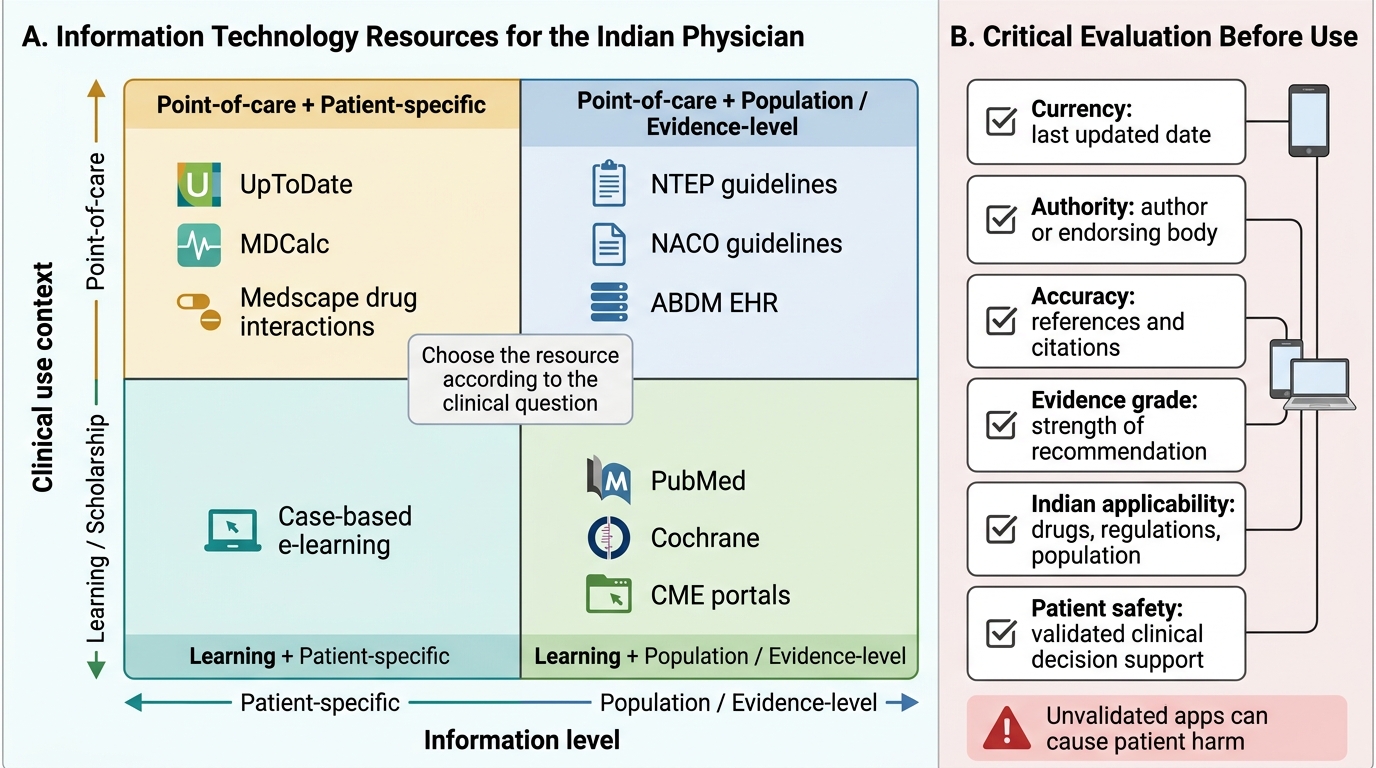
Digital Resource Map for the Indian Physician
Critical evaluation of digital resources is as important as knowing they exist. Not all apps, websites, or databases are equivalent — and the proliferation of unvalidated clinical decision support tools on the internet and app stores is a genuine patient safety concern. Key evaluation criteria:
| Criterion | What to check |
|---|---|
| Currency | When was the content last updated? Is there a date? |
| Authority | Who authored/endorsed the resource? Is it a peer-reviewed, professionally governed organisation? |
| Accuracy | Are statements referenced to primary literature? Are there citations? |
| Evidence grade | Is the recommendation strength specified (e.g., Grade A/B/C, Class I/IIa/III)? |
| Indian applicability | Are drug availability, regulatory context, and Indian population data considered? |
A common error among junior doctors is to use a smartphone app or a Wikipedia article as a primary clinical reference. Wikipedia is useful for orientation but is not peer-reviewed, not continuously quality-monitored, and not graded for clinical applicability. The gold standard for point-of-care clinical questions is a validated, continuously updated clinical reference such as UpToDate or the relevant specialty society guideline — not a search engine result, a drug package insert alone, or an unattributed website.
Digital literacy and safety — the use of IT in clinical care also creates new risks: data entry errors in electronic prescribing systems (the wrong patient selected from a drop-down list), over-reliance on automated alerts leading to alert fatigue and ignored warnings, and the privacy risks of cloud-based health records (discussed under IM29.10). The competent physician uses technology as a tool and not as a substitute for clinical judgment — checking an app recommendation against their own clinical reasoning rather than applying it uncritically.
SELF-CHECK
A 68-year-old patient with newly diagnosed heart failure with reduced ejection fraction (HFrEF, LVEF 32%) is being seen in the outpatient clinic. You want to confirm the current guideline-recommended medical therapy. Which resource is MOST appropriate for retrieving an up-to-date, evidence-graded recommendation at the point of care?
A. Wikipedia's article on heart failure — freely available and comprehensive
B. A cardiology textbook in the hospital library, published in 2018
C. UpToDate or the most recent ESC/ACC/AHA Heart Failure Guidelines, accessed via the professional society website
D. A drug package insert from the ward stock of the medication you plan to prescribe
Reveal Answer
Answer: C. UpToDate or the most recent ESC/ACC/AHA Heart Failure Guidelines, accessed via the professional society website
For evidence-graded point-of-care clinical recommendations, the appropriate resources are continuously updated clinical decision support tools such as UpToDate or the most recent professional society guidelines (ESC Heart Failure Guidelines 2021, updated 2023; ACC/AHA/HFSA 2022). These provide evidence-graded recommendations (Class I/IIa/III with evidence levels) and are updated when new trial data changes practice (e.g., the addition of SGLT2 inhibitors to standard HFrEF therapy after DAPA-HF 2019 and EMPEROR-Reduced 2020). Wikipedia (option A) is not peer-reviewed or evidence-graded. A 2018 textbook (option B) predates the SGLT2 inhibitor evidence, which would give an incomplete treatment recommendation. A drug package insert (option D) describes the approved uses and dosing of a single drug but does not provide comparative evidence or guideline-based treatment algorithms.