Page 8 of 20
IM29.{11,15,23} | Lifelong Learning and Information Technology — SDL Guide (Part 2)
Applying Learning to Practice: Evidence Appraisal and the PICO Framework
The ability to move efficiently from a clinical question to a reliable answer — and to critically evaluate the quality of that answer — is the core applied competency that IM29.15 and IM29.23 target at the SH level. This section develops the practical skill of clinical evidence appraisal, which is the bridge between information retrieval and clinical application.
The PICO framework (Population, Intervention, Comparator, Outcome) is the most widely taught method for structuring clinical questions for evidence retrieval. A well-formed PICO question specifies: who the patient is (age, diagnosis, comorbidities), what intervention you are asking about, what the alternative is (including current standard of care), and what outcome you care about (mortality, symptom relief, hospitalisation, adverse events). Poorly formed questions — 'What drug should I give for diabetes?' — yield overwhelming and unfocused search results. A well-formed PICO — 'In Indian adults with type 2 diabetes and established cardiovascular disease (P), does empagliflozin (I) compared to standard glucose-lowering therapy with metformin and insulin alone (C) reduce the risk of major adverse cardiovascular events (O)?' — yields focused, actionable results.
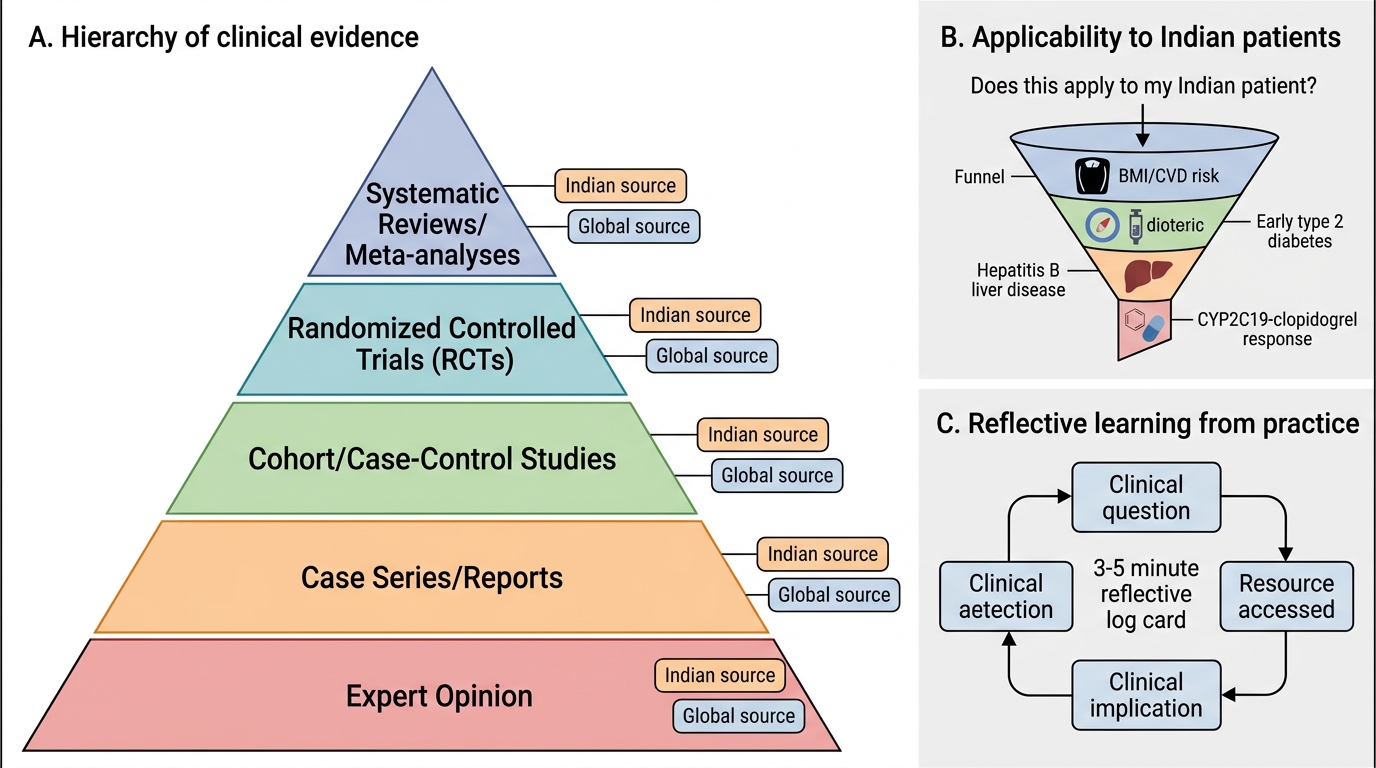
The hierarchy of evidence provides a framework for interpreting the quality of what you find. From highest to lowest:
1. Systematic reviews and meta-analyses (with consistent results across high-quality trials)
2. Individual randomised controlled trials (RCTs) with adequate power and blinding
3. Cohort studies and case-control studies
4. Case series and case reports
5. Expert opinion and consensus statements
Important qualifications to this hierarchy: a poorly conducted systematic review of biased small trials is not better evidence than a well-conducted large RCT; and for rare conditions or new phenomena, expert consensus may be the highest available evidence. The GRADE system (Grading of Recommendations Assessment, Development and Evaluation), used by the WHO, Cochrane Collaboration, and most major clinical guidelines, translates evidence quality into recommendation strength: Strong recommendation (the desirable effects clearly outweigh the undesirable effects for most patients), Conditional recommendation (the balance is uncertain or depends on patient values and context), and We suggest vs We recommend language to signal the difference.
The critical appraisal checklist for a clinical trial involves:
- Was the randomisation adequate and concealed (reduces selection bias)?
- Was blinding maintained — of participants, clinicians, and outcome assessors (reduces performance and detection bias)?
- Was the population representative of patients you see in your practice (external validity)?
- What was the absolute risk reduction (ARR) and number needed to treat (NNT), not just the relative risk reduction (RRR)? A drug that reduces relative risk of stroke by 25% sounds impressive — but if the absolute baseline risk is only 1%, the absolute reduction is 0.25% and the NNT is 400, meaning 400 patients must be treated for one year for one to benefit.
- What were the harms — what was the number needed to harm (NNH)?
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Evidence Hierarchy and Contextual Clinical Judgment
The applied significance of this skill for the Indian physician: clinical practice guidelines developed in European or North American populations may not be directly applicable to Indian patients, who have different phenotypic risk profiles (higher cardiovascular risk at lower BMI, earlier onset type 2 diabetes, higher rates of hepatitis B as a cause of chronic liver disease, different genetic variants affecting drug metabolism — e.g. CYP2C19 polymorphisms affecting clopidogrel efficacy). The physician who applies evidence uncritically — without asking 'does this apply to my patient?' — is performing a form of intellectual shortcut that can harm patients in whom the assumed population parameters do not hold.
The habit of clinical reflection and learning from practice — the component of IM29.23 beyond formal CME — involves a daily discipline of identifying knowledge gaps during clinical work and systematically addressing them. The most effective method, supported by educational research, is the reflective log: a brief (3–5 minute) written note at the end of each clinical session recording one clinical question that arose, the resource accessed to answer it, and the clinical implication. This habit, sustained over months, builds a personalised clinical knowledge base and documents the lifelong learning behaviour the NMC expects.
SELF-CHECK
A new trial reports that drug X reduces the relative risk of cardiovascular death by 25% compared to placebo (RRR = 25%). The absolute risk of cardiovascular death in the trial population was 8% over 5 years in the placebo group and 6% in the treatment group. What is the Number Needed to Treat (NNT) to prevent one cardiovascular death over 5 years?
A. 4 patients
B. 25 patients
C. 50 patients
D. 12.5 patients
Reveal Answer
Answer: C. 50 patients
NNT = 1 / Absolute Risk Reduction (ARR). ARR = 8% - 6% = 2% = 0.02. NNT = 1/0.02 = 50. This means 50 patients must be treated with drug X for 5 years to prevent one cardiovascular death. The relative risk reduction of 25% (which sounds large) corresponds to an ARR of only 2% because the baseline event rate is low. Understanding ARR and NNT — rather than reporting only RRR — is essential for communicating treatment benefits to patients and for cost-effectiveness analysis. A treatment with NNT = 50 may still be worth prescribing if the condition is serious and the drug is safe and affordable, but the physician should know the NNT to make an informed recommendation.
Self-Assessment: Applying Lifelong Learning and IT Competencies
You have now covered the professional obligation of lifelong learning, the regulatory framework under NMC 2023 CME regulations, the PBLI cycle for self-directed learning, the major categories of information technology for clinical practice and learning, and the evidence appraisal skills needed to translate information into action. The scenarios below integrate these competencies in the format expected in the final-year examination.
For each scenario, identify which competency (IM29.11, IM29.15, or IM29.23) is primarily at stake, describe the appropriate approach, and explain the reasoning.
Scenario A — Out-of-date clinical practice:
A 52-year-old woman is admitted with a first-episode atrial fibrillation with rapid ventricular rate and no structural heart disease on echocardiogram. A senior colleague recommends digoxin for rate control, as he was trained 25 years ago. Current guidelines (ACC/AHA 2019; ESC 2020) position digoxin as a fourth-line agent for rate control in AF, after beta-blockers and non-dihydropyridine calcium channel blockers, and only when other agents are contraindicated or insufficient — a significant change from its position 25 years ago. How would you, as the most junior member of the team, address this knowledge gap professionally while remaining within appropriate professional hierarchies?
Analysis: This is IM29.11 and IM29.23 in action. The appropriate approach is not confrontation but evidence-based advocacy: access the current guideline on UpToDate or the ACC/AHA portal (IM29.15), identify the specific recommendation and evidence grade, and raise it with the senior colleague in a respectful, evidence-based way — 'I was just checking the current guideline for AF rate control and noticed that beta-blockers are now first-line — would you like me to pull it up for the round?' This approach serves the patient's interest, demonstrates the lifelong learning habit, and models evidence-based practice without undermining the professional relationship. If the concern is not addressed and the patient is at risk, escalating to the registrar or using the institution's clinical governance channel is appropriate.
Scenario B — Digital resource quality:
You are on a community health posting and a colleague uses a smartphone app to check the dosing for an antiretroviral drug for a new HIV-positive patient. The app has 4.5 stars in the App Store, was last updated 18 months ago, and provides no citations. He follows the recommendation and prescribes accordingly. What is the problem, and what resource would you recommend instead?
Analysis: The problem is the uncritical use of an unvalidated digital resource for a high-stakes clinical decision. The characteristics of a reliable HIV/ART prescribing resource: continuous updates aligned with NACO ART guidelines and WHO consolidated ARV guidelines; evidence citations; regulation by a professional body or government authority. The appropriate resources for ART prescribing in India are the NACO ART Guidelines (available on the naco.gov.in portal), the WHO Consolidated Guidelines on HIV (who.int), and the clinical pharmacology sections of DHHS ART guidelines (aidsinfo.nih.gov) for complex drug interactions. A 4.5-star app is not a substitute for these authoritative sources, especially for schedule H1 drugs with narrow therapeutic windows and complex drug interactions (e.g., rifampicin-based NTEP regimen with efavirenz-based ART — a combination requiring dose adjustment and monitoring).
Resource Selection Matrix for Evidence-Based Practice in Indian District Settings
Scenario C — Applying evidence in a resource-constrained setting:
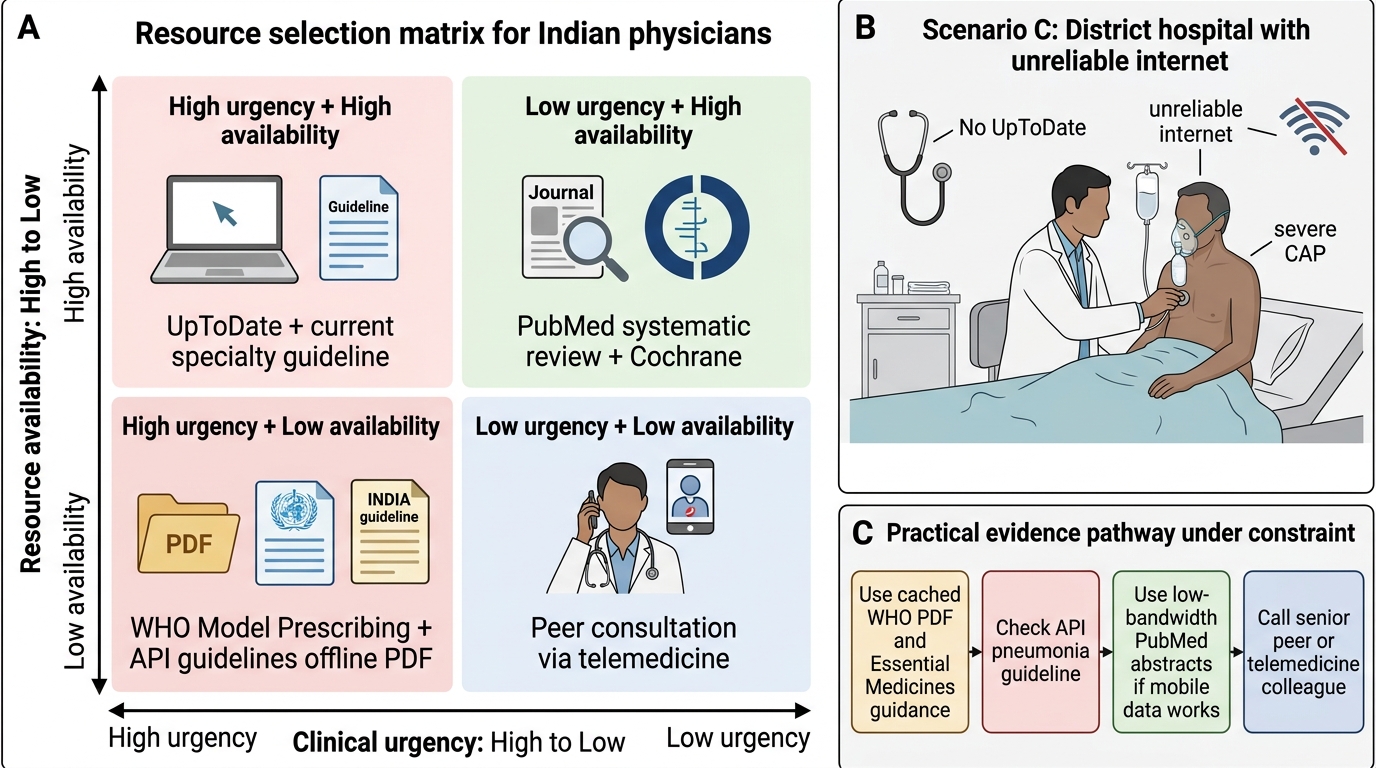
You are posted to a district hospital where UpToDate is not available and internet access is unreliable. A patient presents with severe community-acquired pneumonia. How would you access current evidence for management without institutional database access?
Analysis: This tests practical digital literacy under constraint (IM29.15). Options in this scenario: (1) The WHO Model Prescribing Information and WHO Essential Medicines guidelines are downloadable as PDF for offline use; (2) The API Clinical Practice Guidelines for pneumonia (Association of Physicians of India, freely available) are India-specific and applicable to the public sector drug formulary; (3) PubMed abstracts are freely accessible even on mobile data at low bandwidth; (4) Many professional society guideline documents (British Thoracic Society, Infectious Diseases Society of America) are available as free PDF downloads and can be cached offline; (5) Colleagues in larger hospitals can be consulted via telemedicine under the Telemedicine Practice Guidelines 2020. The lesson: lifelong learning and digital resource access are not only possible in resource-constrained settings — they require more deliberate planning, but the core resources exist and can be accessed with a modest and systematic effort.
CLINICAL PEARL
The 'five-year rule' for clinical knowledge: in rapidly evolving specialties (oncology, cardiology, infectious disease, diabetology), assume that any clinical knowledge you acquired more than five years ago may have been substantially revised, and verify it against a current guideline before applying it to a patient with a new presentation in those fields. The NTEP shift from intermittent to daily TB regimens, the SGLT2 inhibitor revolution in heart failure, the DOAC displacement of warfarin for most AF indications, and the CAR-T cell therapies in haematological malignancies all happened within the last decade. A physician who graduated in 2015 and has not actively updated their knowledge in any of these areas is practising with significant gaps.
A second pearl on IT safety: alert fatigue — the phenomenon by which clinicians begin ignoring automated drug interaction or allergy alerts because they are too frequent and too many are low-priority — is now a major safety concern in hospitals with electronic prescribing. Studies suggest that up to 95% of drug interaction alerts in some EHR systems are overridden. The clinical implication: do not assume the system will protect you — critical alerts (particularly for high-alert medications and known severe drug interactions) should always be actively reviewed, not routinely dismissed. The computer alert is a tool; the clinical judgment is yours.