Page 1 of 20
IM29.1-7 | Principles of Medical Ethics — SDL Guide
Learning Objectives
- State the four prima facie principles of biomedical ethics (non-maleficence, beneficence, autonomy, justice) and give a clinical example of each
- Explain the Indian regulatory framework governing clinical ethics including the NMC Code 2002, Consumer Protection Act 2019, Mental Healthcare Act 2017, and IPC Sections 88 and 92
- Describe the elements of valid informed consent and apply the reasonable patient standard from Samira Kohli v Dr Prabha Manchanda (2008)
- Analyse principle conflicts (beneficence vs autonomy; confidentiality vs duty to warn) using the prima facie duty framework and identify a defensible resolution
- Discuss advance directives, surrogate decision-making, and emergency incapacity with reference to Common Cause v Union of India (2018)
- Identify the key requirements for ethical conduct of research involving human participants under ICMR Guidelines 2017/2023 and the Declaration of Helsinki
- Apply the four-quadrant ethical analysis (Jonsen) to a case vignette involving resource allocation, consent, or confidentiality
INSTRUCTIONS
Medical ethics provides the intellectual framework within which every clinical decision is embedded. This module develops your ability to identify, reason about, and defend your position on the ethical dimensions of clinical practice — from bedside consent to emergency incapacity, from confidentiality breaches to resource allocation under scarcity. You will learn the four prima facie principles, their interaction and conflict, the Indian regulatory landscape, and how to apply structured ethical reasoning to real clinical dilemmas. This is not a 'soft skills' module — it is the analytical foundation for professional medical practice.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chapter 4 — Ethical Issues in Clinical Medicine (textbook)
- API Textbook of Medicine, 10th ed. — Medical Ethics and Medical Jurisprudence (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed. — Medical Ethics (textbook)
- ICMR National Ethical Guidelines for Biomedical and Health Research Involving Human Participants, 2017 (updated 2023) (guideline)
- NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (amended 2023) (guideline)
- Supreme Court of India: Common Cause v Union of India, AIR 2018 SC 1665 (advance directives and right to die with dignity) (legal)
- Supreme Court of India: Samira Kohli v Dr Prabha Manchanda & Anr, (2008) 2 SCC 1 (informed consent — reasonable patient standard) (legal)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are the registrar on call in a busy medical ward. At 2 AM, Mr. Ramesh, a 58-year-old with end-stage chronic kidney disease, is admitted with severe breathlessness. His family crowd the corridor — his wife, two adult sons, and a daughter who flew in from Bengaluru. They tell you firmly: 'Doctor, he does not know how sick he is. Do not tell him the diagnosis. In our family we protect elders from bad news.' You enter the room. Mr. Ramesh looks up at you, frightened, and asks quietly: 'Doctor, am I going to die?' In the next few seconds, four deeply held values — his right to know the truth, his family's love and cultural authority, your duty not to harm, and your professional honesty — collide with one another. There is no guideline that tells you precisely what to say. You are in the space where medicine becomes ethics. This module gives you the intellectual tools to navigate that space — not with a formula, but with a principled framework.
WHY THIS MATTERS
Medical ethics is not a philosophical luxury reserved for academic debate — it is an operational necessity that shapes every clinical encounter. The NMC 2024 curriculum expects final-year MBBS students to be able to identify, discuss, and defend the medico-legal, socio-cultural, and economic dimensions of clinical decision-making across a range of scenarios: informed consent, advance directives, surrogate decision-making, emergency incapacity, confidentiality, research participation, resource allocation, and justice in health access. These competencies (IM29.1–IM29.7) are at the Knowledge and Application level — you are expected not only to state the four ethical principles but to reason with them, to recognise when they conflict, and to articulate a defensible resolution. In India, these questions are shaped by the NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (and its 2023 revisions), the Consumer Protection Act 2019, the Mental Healthcare Act 2017, and the Transplantation of Human Organs and Tissues Act 1994. Understanding these frameworks protects your patient, protects you as a clinician, and upholds the social contract that gives medicine its authority.
RECALL
Before proceeding, activate what you already know. From your first year, you encountered the Hippocratic tradition and the idea that the physician's first obligation is to the patient's wellbeing. From your community medicine posting, you saw how systemic factors — poverty, gender, caste, geography — determine who gets care and who does not. From your clinical years, you have observed consent forms being signed in corridors, family members speaking on behalf of patients, and colleagues making split-second decisions in emergencies. You have also seen variation: some patients demand to know everything; others say 'just do what is best, doctor.' The question ethics asks is: how do you reason your way through that variation in a principled, consistent, and defensible manner? The four-principle framework — sometimes called principlism or the Georgetown Mantra — provides one widely adopted starting point. Recall too that 'medical law' and 'medical ethics' overlap but are not identical: law defines minimum enforceable standards; ethics asks what you should do even when the law does not compel you.
Why Ethics in Clinical Medicine: Orientation and the Indian Context
The claim that medicine is an applied science tells only half the story. Medicine is also an applied moral enterprise — every diagnostic and therapeutic decision involves choices about what matters, whose interests count, and how to act when certainty is absent. Understanding why ethics is not optional in clinical practice, and how it is embedded in the Indian regulatory and cultural landscape, is the necessary foundation before any principled framework can be meaningfully applied.
The physician-patient relationship is asymmetric in a specific and ethically important way: the patient approaches with need, vulnerability, and often diminished information; the physician holds technical expertise, institutional authority, and access to resources. This asymmetry generates a power differential that ethics is designed to govern. Without ethical principles, clinical authority can become paternalism, and paternalism — however well-intentioned — can violate a person's fundamental dignity. The history of medicine contains instructive failures: experiments conducted on unknowing populations, therapeutic decisions imposed on patients who were never asked, and institutional practices that systematically disadvantaged the poor and the marginalised. Modern medical ethics emerged partly as a corrective — first with the Nuremberg Code 1947 (in response to Nazi medical experimentation), then with the Declaration of Helsinki 1964 (protecting research participants), and in India with the ICMR Guidelines for Biomedical and Health Research 2017 and the NMC Code of Ethics Regulations 2002.
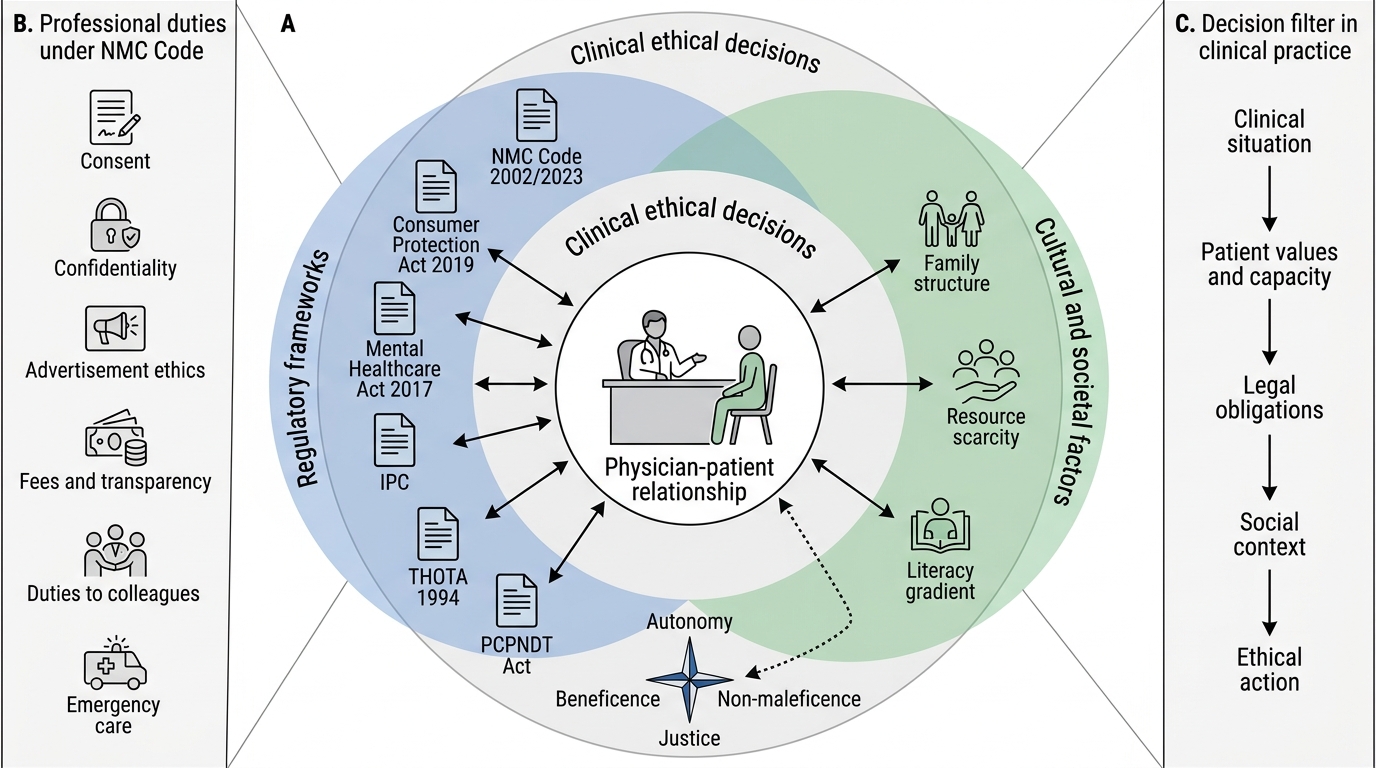
In the Indian clinical context, three structural features make ethical reasoning especially important. First, socio-economic heterogeneity: the physician in a public teaching hospital serves patients across an enormous range of literacy, economic means, and health understanding — the ethical obligation of explanation and consent cannot be met with the same conversation in all cases. Second, family-centred decision culture: in contrast to the Northern European and North American model of strict individual autonomy, Indian patients frequently make decisions within a family unit, and families frequently assert authority over disclosure. This is not ethically wrong per se — it must, however, be navigated without substituting the family's preference for the patient's own expressed wish. Third, regulatory complexity: the physician in India operates under at least six overlapping legal frameworks — the Indian Medical Council Act 1956 (now superseded by the NMC Act 2020), the Indian Penal Code (covering negligence and homicide by rash/negligent act), the Consumer Protection Act 2019 (medical services are 'services' and patients are 'consumers'), the Mental Healthcare Act 2017, the Pre-conception and Pre-natal Diagnostic Techniques (PCPNDT) Act 1994, and the Transplantation of Human Organs and Tissues Act (THOTA) 1994. A clinician who understands only the clinical science and not these frameworks is incompletely equipped.
Ethical Decision-Making Around the Physician-Patient Relationship
The NMC Code of Professional Conduct, Etiquette and Ethics Regulations 2002 (amended 2023) defines the physician's obligations in concrete terms: duties regarding consent, confidentiality, advertisement, fees, duties to colleagues, duties in emergencies, and duties with respect to torture and unethical practices. Importantly, the NMC Code makes clear that a registered medical practitioner is expected to maintain professional standards regardless of institutional pressure, commercial incentive, or personal relationship. Violations can lead to disciplinary action including suspension or removal from the NMC register — a consequence with immediate legal and professional force. Understanding the Code is therefore not merely about ethics in the abstract but about professional survival.
The Four Prima Facie Principles and the Indian Regulatory Frame
The dominant organising framework for clinical ethics in contemporary medicine is the four-principle approach articulated by Tom Beauchamp and James Childress in Principles of Biomedical Ethics (first published 1979; now in its eighth edition). This framework has been adopted by medical councils, professional bodies, and courts worldwide as the baseline language of ethical reasoning in clinical settings. The four principles are: non-maleficence, beneficence, autonomy, and justice. Each is described as prima facie binding — meaning it creates a presumptive moral obligation that must be respected unless overridden by a stronger competing obligation from another principle. No single principle is lexically superior to the others; when they conflict, the task is principled deliberation, not a predetermined hierarchy.
Provided image
Understanding these four principles as the structural vocabulary of medical ethics is analogous to understanding the four vital signs in clinical assessment — they do not tell you the diagnosis, but without them you cannot organise your thinking.
1. Non-maleficence — the duty to avoid causing harm (IM29.1)
Non-maleficence derives from the Hippocratic phrase primum non nocere — 'first, do no harm'. In clinical practice it operates as a negative duty: refrain from actions that cause unnecessary harm to the patient. It is important to note that non-maleficence does not mean 'take no action' — many beneficial interventions carry inherent risk (surgery, chemotherapy, invasive diagnostics). The principle requires that risks be proportionate to expected benefit and that harm not be imposed carelessly, unnecessarily, or without the patient's informed understanding. The classic doctrine of double effect addresses situations where a beneficial action has an unavoidable harmful side effect — for example, administering adequate opioid analgesia in a terminally ill patient may hasten death as a foreseen but unintended side effect. The double effect doctrine holds this permissible when: (a) the act itself is not intrinsically wrong, (b) the agent intends the benefit not the harm, (c) the harm is not the mechanism by which the benefit is achieved, and (d) the benefit is proportionate to the harm. In Indian law, actions taken in good faith for the benefit of a patient are protected under Section 88 of the Indian Penal Code — a clinician acting in good faith without criminal intent is not criminally liable even if harm results.
2. Autonomy and shared responsibility — the right to self-determination (IM29.2)
Autonomy is the principle that a competent person has the right to make decisions about their own body and health care, free from coercion. In clinical practice this principle manifests primarily as the requirement for informed consent — before any diagnostic procedure or therapeutic intervention, the patient must be given adequate information (diagnosis, proposed intervention, reasonable alternatives, risks and benefits, and the option of refusal) in a language and format they can understand, must have the capacity to understand and decide, and must consent voluntarily. Shared responsibility is the complementary idea that the patient and physician are both moral agents in the clinical relationship — the physician holds expertise; the patient holds authority over their own person. The physician's role is to inform and advise, not to decide on the patient's behalf. In the Indian cultural context, autonomy must be interpreted with sensitivity to family dynamics: a patient may choose to delegate decision-making to a family member, and this choice itself is an exercise of autonomy. The ethical problem arises when the family makes decisions the patient has not authorised.
3. Beneficence — the duty to act for the patient's benefit (IM29.3)
Beneficence is the positive duty to act in the patient's best interests. It is what motivates the physician to treat, to diagnose, to alleviate suffering, and to preserve life. Beneficence must be distinguished from paternalism — acting for someone's benefit in ways that override their autonomous choices. Strong paternalism (overriding a competent patient's explicit refusal for their own good) is generally ethically impermissible. Weak paternalism (acting for a patient's benefit when they lack capacity, as in an emergency) may be justified. The principle of beneficence also encompasses the obligation to refer — if the clinician does not have the competence to provide the best care, the ethical obligation to act in the patient's interest requires timely referral to someone who does.
4. Justice — fairness in access and resource allocation (IM29.4)
Justice in healthcare ethics addresses two domains: (a) distributive justice — the fair allocation of healthcare resources across populations; and (b) rights-based justice — the claim that all patients, regardless of socio-economic status, caste, religion, gender, or disability, have an equal claim to appropriate care. In India, distributive justice is acutely visible: the public health system is chronically under-resourced, and the physician working in a district hospital operates under real scarcity. The ethical question becomes not merely 'what does this patient need?' but 'how do I allocate what is available in a way that is fair and defensible?' The National Health Mission and Ayushman Bharat PM-JAY scheme represent policy-level attempts to address the justice dimension — expanding coverage to below-poverty-line families. At the bedside, justice requires non-discrimination and equal dignity in treatment.
The magnitude of ethical dilemmas in practice is significant: studies from Indian tertiary care hospitals suggest that ethical issues arise in 30–50% of ICU admissions (consent, family surrogacy, withholding/withdrawing treatment), and that physicians report under-preparedness to handle them. This is not a rare occurrence but a routine feature of clinical practice.
How Principles Interact: Mechanisms of Ethical Reasoning and Conflict
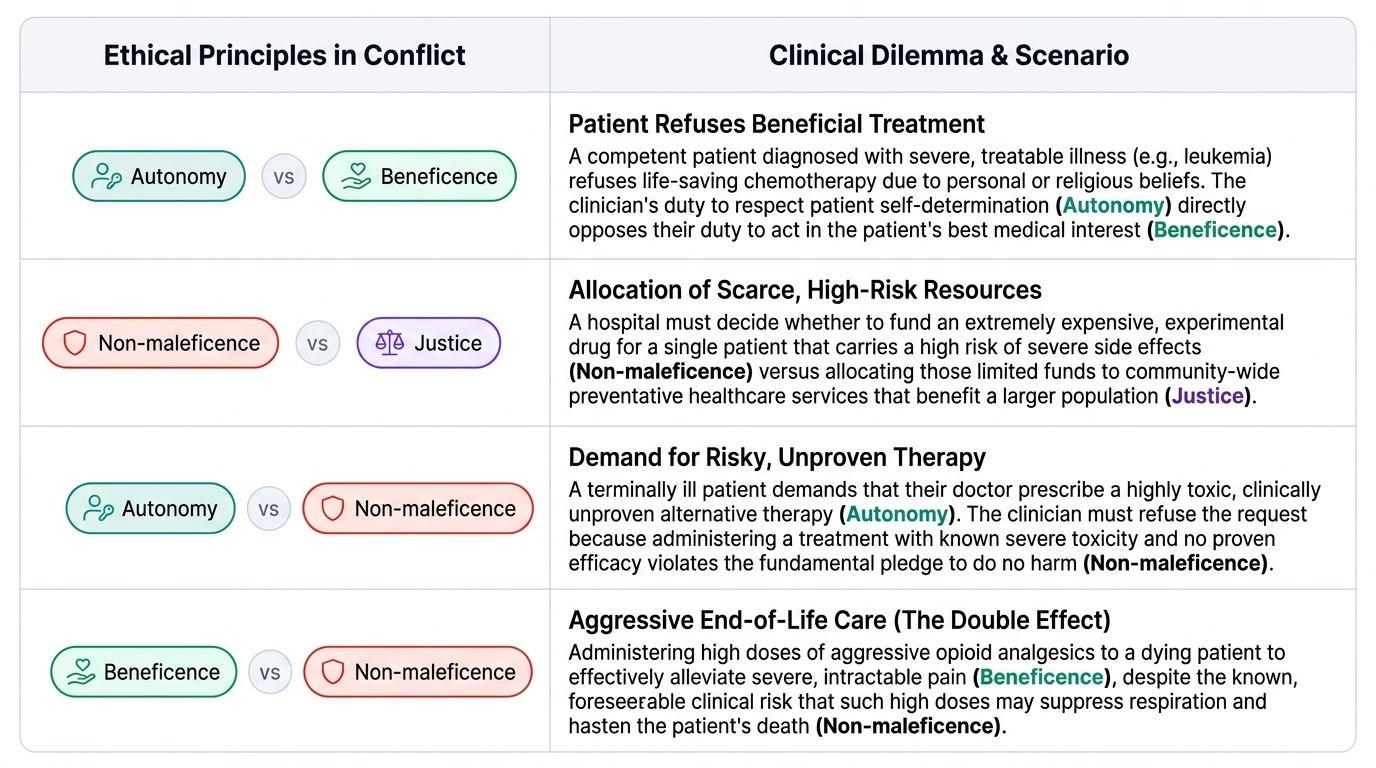
The four principles do not operate in isolation from one another, nor do they yield automatic answers. The core intellectual challenge of clinical ethics is navigating principle conflict — situations where acting on one principle requires compromising another. Understanding the mechanisms by which principles interact, conflict, and are weighed is the analytical skill that distinguishes ethical reasoning from ethical platitude.
The central insight of principlism is that moral obligations are not absolute rules but prima facie duties (W.D. Ross's term, adopted by Beauchamp and Childress). A prima facie duty is binding unless it is overridden by a stronger duty in a specific situation. When two prima facie duties conflict, the clinician must assess the weight of each obligation in that particular context — considering the severity of the harm at stake, the degree of capacity the patient has, the availability of alternatives, and the cultural and relational context. This process is called moral deliberation, and it is the skill this section develops.
The beneficence-autonomy conflict is the most commonly encountered and most instructive. Beneficence says: this patient needs treatment X. Autonomy says: the patient has the right to refuse. When a competent adult patient refuses treatment — including life-saving treatment — autonomy typically prevails. The physician's obligation is to ensure the patient's decision is truly informed (not based on a misunderstanding) and truly voluntary (not coerced by fear or family pressure), to document the refusal, and to continue to offer care while respecting the decision. The legal standard in India is that proceeding with treatment against a competent patient's explicit written refusal constitutes battery. However, when the patient lacks capacity — due to unconsciousness, severe psychiatric illness, dementia, or intellectual disability — the beneficence obligation can legitimately override the absent autonomous choice, and the physician acts in what is called the patient's best interests.
Capacity is a crucial and frequently mis-assessed concept. Decision-making capacity is not a binary label ('competent' or 'incompetent') but a task-specific, time-specific, and decision-specific assessment. A patient may have capacity to consent to a blood draw but not to a complex surgical decision. The functional elements of capacity are: (1) ability to understand the relevant information; (2) ability to appreciate how the information applies to their own situation; (3) ability to reason about options; and (4) ability to express a consistent choice. Mental illness does not automatically remove capacity; nor does illiteracy or poor education. When capacity is genuinely absent, a hierarchy of surrogate decision-making applies — in descending order: a legally appointed healthcare proxy, a spouse or nearest relative, the patient's previously expressed wishes (oral or in an advance directive), and the physician's assessment of best interests.
The non-maleficence vs beneficence tension arises when treating a condition requires exposing the patient to risk. All significant medical and surgical interventions carry this tension. The resolution framework is the benefit-risk calculus: the expected benefit must outweigh the expected risk, assessed probabilistically and calibrated to the individual patient's values. A 40% mortality risk from surgery is acceptable to a patient whose only alternative is certain death from disease, but may not be acceptable to a patient with a terminal illness who values remaining time and quality over quantity of life. The physician who does not ask about the patient's values is doing arithmetic, not ethics.
The justice-autonomy tension emerges in contexts of resource allocation. A patient may have the autonomy to request high-cost, low-yield treatment (e.g., fourth-line chemotherapy for refractory cancer). The justice principle asks whether providing that treatment is fair to other patients competing for the same scarce resource. Triage in emergency medicine is the most systematic formalised attempt to resolve this tension — allocating priority of care based on clinical urgency and expected benefit, not on who arrived first or who can pay. The ethical defensibility of triage depends on its transparency, consistency, and freedom from discriminatory factors.
The confidentiality-beneficence tension (or confidentiality vs duty to warn) arises when a patient discloses information suggesting risk to a third party. The paradigmatic case is a patient who discloses HIV-positive status but refuses to inform a regular sexual partner. The physician's duty of confidentiality (rooted in both autonomy and the foundational trust relationship that makes patients disclose at all) conflicts with the duty to prevent harm to the identifiable partner. Indian ethical guidance (ICMR guidelines, NMC Code) permits breach of confidentiality to prevent serious harm to an identifiable third party — but only after attempting to persuade the patient to disclose voluntarily, and the breach must be the minimum necessary. The same principle applies to disclosure of a patient's fitness-to-drive in severe cardiac or neurological illness.
A useful analytical tool is the ethical grid or four-quadrant analysis developed by Albert Jonsen and colleagues: assess each clinical case across (1) Medical indications — what are the clinical facts and what can medicine offer?; (2) Patient preferences — what does this patient want and have they expressed it?; (3) Quality of life — how does the proposed intervention affect the patient's quality and length of life?; and (4) Contextual features — family, culture, institutional, and legal constraints. Working through all four quadrants before deciding avoids the common error of focusing exclusively on the clinical facts while ignoring what the patient actually wants.
SELF-CHECK
A 45-year-old farmer with newly diagnosed pulmonary tuberculosis tells you his family does not know he has TB and he does not want to tell his wife, with whom he shares a bed. He refuses permission to contact her. Which ethical principle most directly supports maintaining his confidentiality, and which principle most directly supports disclosure to his wife?
A. Beneficence supports confidentiality; non-maleficence supports disclosure
B. Autonomy supports confidentiality; justice supports disclosure
C. Autonomy supports confidentiality; non-maleficence supports disclosure
D. Non-maleficence supports confidentiality; beneficence supports disclosure
Reveal Answer
Answer: C. Autonomy supports confidentiality; non-maleficence supports disclosure
The patient's right to control sensitive personal health information is an exercise of autonomy — respecting his decision not to disclose is an autonomy-based obligation. However, the wife faces a real and preventable risk of infection: non-maleficence (the duty to avoid causing harm to others) supports warning her. This is the classic confidentiality vs duty-to-warn conflict. ICMR and NMC guidance allows breach of confidentiality to prevent serious harm to an identifiable third party, but only after attempting voluntary disclosure first. Justice would be relevant to broader resource allocation questions; beneficence is about the patient's own benefit, not preventing harm to a third party.