Page 2 of 20
IM29.1-7 | Principles of Medical Ethics — SDL Guide (Part 2)
Applied Clinical Ethics: Consent, Confidentiality, End-of-Life, and Medico-Legal Dimensions
Ethical principles acquire their full operational meaning only when applied to concrete clinical situations. This section works through six domains of applied ethics that correspond directly to the IM29 competency set — consent and capacity, advance directives and surrogate decision-making, emergency incapacity, confidentiality, resource allocation and justice, and research ethics. Each domain is mapped to its regulatory framework in India.
Informed consent — the legal and ethical standard (IM29.2, IM29.5)
In India, informed consent is required before every diagnostic procedure and therapeutic intervention that carries material risk. The legal basis is: (a) the NMC Code of Ethics Regulations 2002, which mandates written consent for operations and invasive procedures; (b) the Supreme Court's ruling in Samira Kohli v Dr Prabha Manchanda (2008), which established that the standard is what a reasonable patient would want to know — not merely what a reasonable doctor thinks is necessary to disclose; and (c) the Consumer Protection Act 2019, under which failure to obtain adequate consent is a deficiency of service actionable before a consumer forum. The elements of valid consent are: (1) disclosure of diagnosis, proposed procedure, material risks and benefits, reasonable alternatives including no treatment, and prognosis with and without treatment; (2) demonstrated understanding by the patient; (3) voluntariness — absence of coercion or undue influence; (4) capacity; and (5) decision. Consent must be specific — consent to an appendicectomy does not authorise removal of an incidentally found ovarian cyst unless separate intraoperative consent is obtained. A signature on a blanket consent form does not constitute informed consent; it is merely evidence that some conversation occurred.
The doctrine of therapeutic privilege — withholding information on the grounds that disclosure would harm the patient — has been substantially narrowed by Indian jurisprudence following the Samira Kohli ruling. Therapeutic privilege cannot be used routinely to justify non-disclosure; it may be invoked only in exceptional circumstances where disclosure would cause immediate serious psychological or physical harm, and even then the physician must document the reasoning.
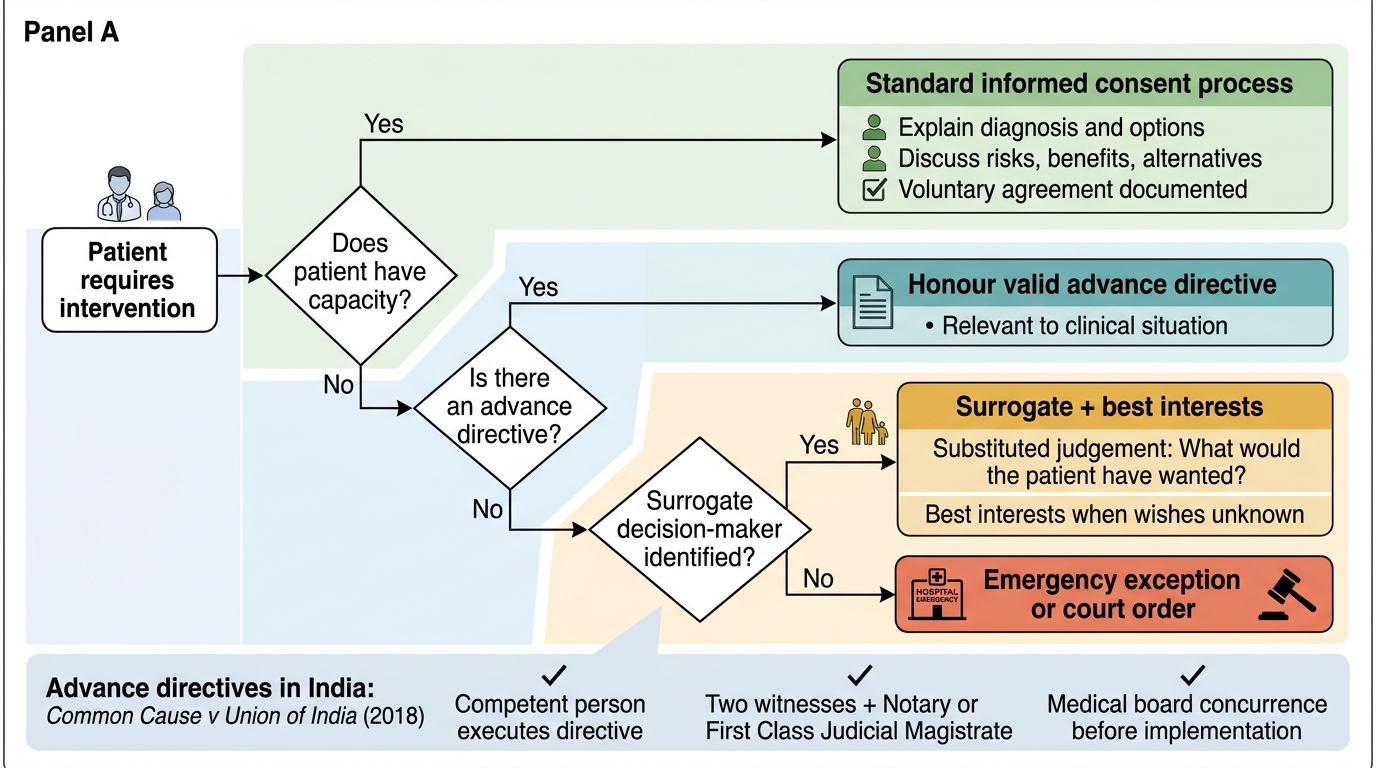
Consent Decision Pathway for Medical Intervention
Advance directives and surrogate decision-making (IM29.5)
An advance directive (also called a 'living will') is a document in which a competent person specifies the medical treatments they wish to receive or refuse in the event of future incapacity. In India, the Supreme Court in Common Cause v Union of India (2018) affirmed the constitutional right to execute an advance directive regarding end-of-life care, including the right to refuse life-sustaining treatment. The ruling established a procedure: the directive must be signed in the presence of two witnesses and countersigned by a Notary or First Class Judicial Magistrate, and a medical board must concur before it can be implemented. Advance directives are legally binding on the treating physician when properly executed and relevant to the clinical situation. When no advance directive exists and the patient lacks capacity, surrogate decision-making applies. The surrogate — usually the nearest relative — is expected to apply a substituted judgement standard: 'What would this patient have wanted?' (based on their known values and previously expressed wishes), not 'What do I want for this patient?' or 'What would I want in this situation?'
Emergency incapacity and the doctrine of implied consent (IM29.6)
When a patient presents in an emergency and is unable to give consent (due to unconsciousness, severe intoxication, acute psychosis, or critical illness), the legal and ethical framework in India permits — and requires — emergency treatment under the doctrine of implied consent: a reasonable person in that situation would consent to life-saving treatment, and the physician is therefore authorised to proceed. This authorisation is limited to what is immediately necessary to preserve life and prevent serious deterioration; it does not extend to elective or non-urgent interventions. The NMC Code (Regulation 2.3) explicitly states that a physician must provide emergency care and that refusal to treat in a life-threatening emergency is unethical. Under Section 92 of the IPC, acts done in good faith for the benefit of a person who cannot give consent (due to unsoundness of mind or extreme incapacity) are protected from criminal liability.
The challenge arises when family members refuse emergency treatment on the patient's behalf — for example, refusing a blood transfusion on religious grounds for an unconscious patient. In Indian law, a competent patient's own refusal of life-saving treatment is ultimately autonomous and legally protected. However, a family member's refusal on behalf of an unconscious patient does not have absolute legal force — the physician is ethically and legally permitted to proceed with emergency life-saving treatment unless there is a clearly documented advance directive from the patient specifically refusing that intervention.
Confidentiality — scope and legally permissible exceptions
Medical confidentiality is the duty to protect all information disclosed by the patient in the clinical relationship from disclosure to third parties without consent. It is foundational to trust — without it, patients would withhold information that is clinically necessary. The NMC Code Regulations 2002 (Chapter 2, Regulation 2.2) specify the duty of professional secrecy and its exceptions. The legally permissible exceptions to confidentiality in India are: (1) mandatory notification of notifiable diseases (cholera, plague, malaria, measles, typhoid, hepatitis, HIV under the NACO guidelines — notification to public health authorities, not to family); (2) duty to warn an identifiable third party at serious risk (the Tarasoff principle, adopted by ICMR guidelines for HIV and infectious disease contexts); (3) court orders or requirements under the CrPC to produce medical evidence; (4) disclosure to other treating healthcare professionals on a need-to-know basis; and (5) the coroner or police in cases of unnatural death, suspected poisoning, or medico-legal emergency.
Resource allocation, equity, and justice at the bedside (IM29.4)
The final-year physician in India frequently confronts resource scarcity in its rawest form: one ventilator, two critically ill patients; a single unit of packed cells when both a trauma patient and a patient with GI bleeding need it. The macro-allocation of resources (budget, national programmes, insurance coverage) is a policy decision. But micro-allocation — who gets the available resource — falls to the clinician. The ethical framework for micro-allocation is: (a) medical utility — prioritise the patient most likely to benefit; (b) fair innings — consider the difference between a 25-year-old and an 85-year-old with the same severity of illness (this is ethically contested but clinically applied); (c) first come, first served as a fairness default when clinical factors are equal; and (d) absolute prohibition on allocation based on race, caste, religion, gender, or ability to pay. The Ayushman Bharat scheme represents an institutional attempt to reduce the financial barrier dimension of justice — the physician must ensure eligible patients are enrolled and receive entitled benefits.
Research ethics and the rights of study participants (IM29.7)
The physician involved in research — whether as principal investigator, sub-investigator, or co-author — operates under the ICMR Guidelines for Biomedical and Health Research Involving Human Participants 2017 (updated 2023) and the Good Clinical Practice Guidelines issued by the Central Drugs Standard Control Organisation. The foundational principles are those of the Belmont Report 1979: respect for persons (voluntary informed consent with special protection for vulnerable groups), beneficence (maximising benefit and minimising risk), and justice (fair selection of research participants, not exploiting vulnerable populations). In India, specific protections apply to research on vulnerable populations: prisoners, children, pregnant women, tribal communities, and illiterate individuals require additional safeguards and often independent witness consent. All research involving human participants must be approved by an Institutional Ethics Committee (IEC) registered with the NMC/ICMR before recruitment begins — retrospective ethics approval is not acceptable. The Declaration of Helsinki 2013 requires that research protocols be registered in a publicly accessible database (Clinical Trials Registry of India — CTRI) before the first participant is enrolled.
SELF-CHECK
A 70-year-old patient is admitted unconscious following a cerebrovascular accident. His son tells you: 'My father told me last year he would never want to be on a machine to keep him alive.' There is no written advance directive. His Glasgow Coma Score is 6. You need to decide whether to intubate. What is the most defensible course of action?
A. Intubate immediately without discussing with family — emergency consent applies
B. Defer to the son's account and withhold intubation, documenting his verbal report
C. Proceed with intubation as immediate life-preserving emergency measure, while initiating formal surrogate decision process and noting son's account in the record
D. Convene a full ethics committee meeting before any decision
Reveal Answer
Answer: C. Proceed with intubation as immediate life-preserving emergency measure, while initiating formal surrogate decision process and noting son's account in the record
In an acute emergency with a life-threatening condition, the doctrine of implied consent authorises immediate life-preserving intervention. A verbal second-hand account of the patient's previously expressed wishes, without a formal advance directive, does not meet the legal threshold set by the Supreme Court in Common Cause v Union of India (2018) for withholding life-sustaining treatment. The correct approach is to stabilise the patient (intubate) while simultaneously initiating the formal surrogate decision-making process, carefully documenting the son's account, and if possible convening the required medical board review if a decision to withdraw treatment is subsequently considered. Option A is technically correct in the emergency context but ignores the son's input — documenting his account and initiating formal process is part of good practice. Option B is legally unsafe: a verbal report is insufficient to withhold intubation. Option D would cause fatal delay.
SELF-CHECK
A Phase III clinical trial is being conducted in your hospital. A 55-year-old illiterate farmer is a potential participant. The principal investigator has explained the study to him in detail in his local language. The patient says he 'understands' but cannot read or sign. What is the correct consent procedure?
A. Verbal consent alone is sufficient if clearly documented in the case record
B. The patient's thumbprint plus a witness signature on the consent form, after independent confirmation of understanding
C. A family member may sign the consent form on his behalf since he is illiterate
D. Exclude him from the trial — illiterate individuals cannot ethically participate in research
Reveal Answer
Answer: B. The patient's thumbprint plus a witness signature on the consent form, after independent confirmation of understanding
ICMR Guidelines for Biomedical and Health Research 2017 and GCP Guidelines explicitly address illiterate participants: the participant's thumbprint (or other identifying mark) is acceptable in place of a signature, but it must be accompanied by the signature of an impartial witness who independently confirms that the participant was given the information, understood it, and is consenting voluntarily. The witness must be independent of the research team. A family member signing is not the same as the participant consenting — family consent substitutes the patient's autonomy. Verbal consent alone is insufficient for formal research documentation. Excluding illiterate individuals from research would create an unjust knowledge gap (illiterate populations are among the most medically underserved) and violates the Belmont principle of fair access.
Self-Assessment: Ethical Reasoning in Practice
You have now covered the foundational orientation, the four prima facie principles and their Indian regulatory frame, the mechanisms of principle conflict and ethical deliberation, and the applied domains of consent, confidentiality, emergency care, advance directives, research ethics, and justice. The scenarios below ask you to integrate this learning by applying principled reasoning to structured clinical-ethical dilemmas. For each scenario, identify the relevant principles, name the conflict, and articulate the defensible resolution — then compare with the analysis provided.
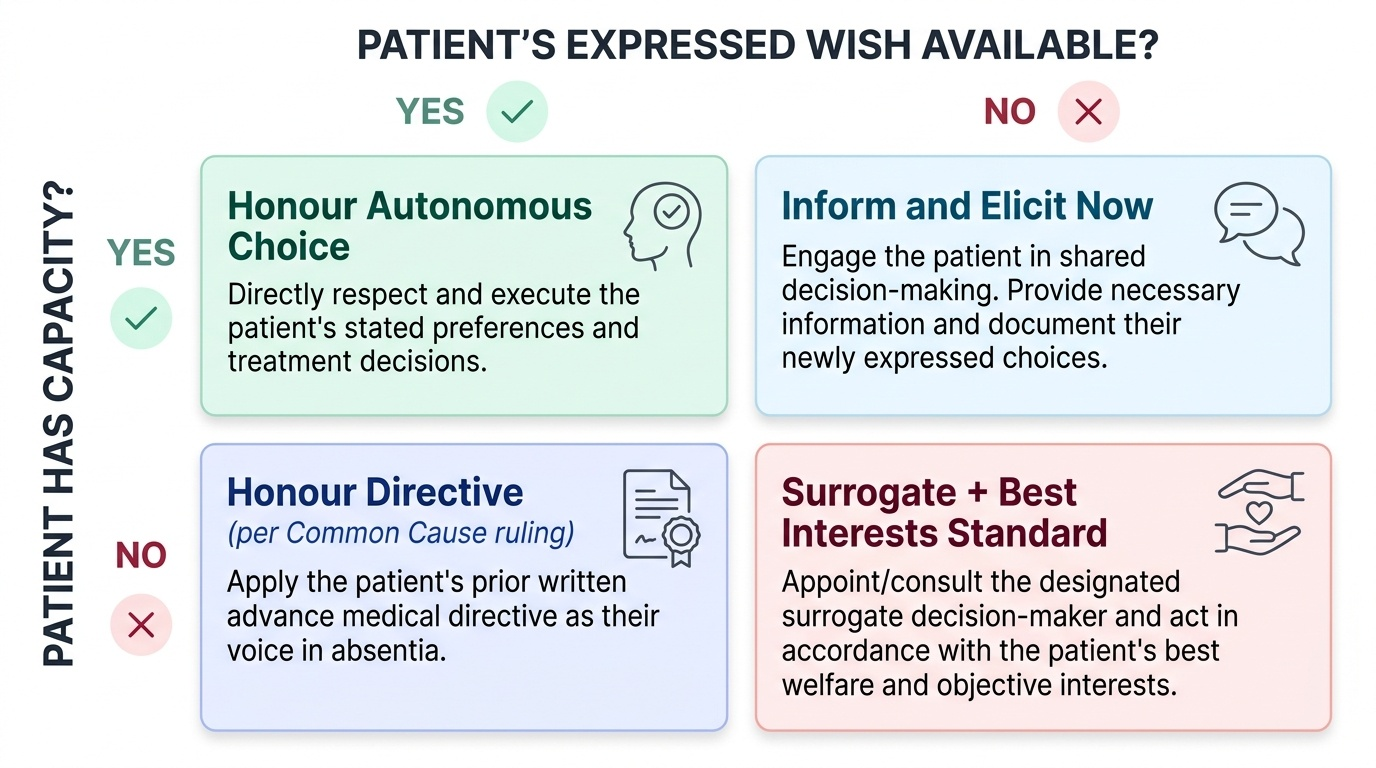
Provided image
A useful self-check is the decision audit: before declaring a clinical-ethical decision final, ask yourself four questions — (1) Would I be comfortable if my supervisor, ethics committee, and the patient's family all heard exactly what I did and why? (2) Does my decision respect the patient's informed choice or, if capacity is absent, their best interests? (3) Can I document the reasoning in the medical record in a way that is defensible to a legal forum? (4) Would another reasonable, experienced clinician looking at the same facts reach a similar conclusion? If the answer to any of these is 'no' or 'I am not sure', the decision requires further deliberation before action.
Scenario A — Therapeutic privilege and the family-first culture:
Mr. Singh, 62, has been diagnosed with stage IV carcinoma of the lung. His family requests that you not disclose the diagnosis to him. They say he is 'too weak to take bad news.' He appears alert and asks you directly what the scan showed.
Analysis: Mr. Singh has capacity — he is alert and has directly asked. Autonomy requires that he be given the information he is requesting. The therapeutic privilege exception (withholding information to prevent harm) cannot be applied routinely; the Samira Kohli ruling makes clear that the reasonable patient standard prevails. You are ethically and legally obligated to answer his question honestly. The ethical management of the family's distress is a separate and equally important task — a frank conversation with them explaining that the patient's right to know overrides their protective impulse, and offering support for how to communicate as a family. A possible middle path is to ask Mr. Singh directly: 'Would you like to know the results yourself, or would you prefer your family to be present?' This respects his autonomy while creating space for family involvement he may welcome.
Scenario B — Jehovah's Witness patient refusing blood transfusion:
Mrs. Patel, 35, a Jehovah's Witness, is admitted with severe post-partum haemorrhage. She is conscious and alert. She has a signed, witnessed, advance refusal of blood transfusion in her records. Her haemoglobin is 4 g/dL. Without transfusion, the medical team believes she will likely die.
Analysis: This is the hardest intersection of autonomy and beneficence. Mrs. Patel is competent, has anticipated this exact situation, and has executed a valid advance directive. The principle of autonomy — including the right to refuse treatment — overrides beneficence in a competent patient. In Indian law, a competent adult's refusal of medical treatment is ultimately protected. The physician's obligations are: (a) confirm current capacity and that the refusal is uncoerced; (b) ensure she understands the likely consequence (death); (c) explore all alternatives (cell salvage, erythropoietin, bloodless surgery techniques, volume expansion); (d) document everything comprehensively; and (e) continue to offer blood transfusion while respecting the refusal. Proceeding with transfusion against her expressed and documented refusal would constitute battery and a violation of her fundamental rights under Article 21 of the Constitution (right to life and personal liberty includes the right to refuse treatment). Note: the situation is different if she loses capacity (becomes unconscious) — then the advance directive governs and the physician is bound by it unless it fails the Common Cause procedural requirements.
Scenario C — Mandatory reporting vs patient confidentiality:
Dr. Priya's patient is a truck driver who was recently diagnosed with a first generalised tonic-clonic seizure. He is on anti-epileptic medication and seizure-free for three months. He informs you that he has not reported this to the transport licensing authority and continues to drive long-haul routes. You are aware that current Indian guidelines recommend a seizure-free period before resuming driving.
Analysis: The confidentiality-non-maleficence tension. The patient's autonomy supports confidentiality. However, non-maleficence to identifiable third parties (other road users, passengers) supports disclosure. The standard approach is: (a) counsel the patient strongly and document that he has been advised of the risk and the guidelines; (b) ask him to self-report to the licensing authority; (c) if he refuses, consult your institution's ethics policy — in many jurisdictions, the physician has the right (and in some, the obligation) to report to the licensing authority if the patient refuses after counselling. The NMC Code does not explicitly address this scenario, but ICMR guidelines and Indian court precedent support a duty to warn where the risk is serious, specific, and identifiable. Document every step.
The three scenarios illustrate the recurring structure of clinical-ethical dilemmas: identify the relevant principles, name the conflict, assess which obligation is weightier in this specific context, consider all options including options that partially satisfy both competing obligations, act, and document.
CLINICAL PEARL
The four ethical principles are not a checklist to complete before proceeding — they are a live analytical frame to be held in mind throughout a clinical encounter. The most common ethical error in clinical practice is not malicious — it is the failure of moral attention: being so focused on the clinical problem that the patient's perspective, values, and autonomous choices are not actually heard. When you leave the bedside after an important clinical conversation, ask yourself: did I listen as carefully as I spoke? Did I give the patient a genuine opportunity to ask questions and to refuse? Did I use language they could understand?
A second pearl specific to the Indian context: documentation is ethics in action. A consent discussion that is not documented is, in the eyes of a consumer forum or a medical negligence court, a consent discussion that did not happen. Write the substance of your explanation in the case record — not just 'consent obtained'. Note who was present, what was explained, what questions were asked, and what the patient's response was. This protects the patient by ensuring the record reflects their choices, and it protects you by demonstrating that you fulfilled your ethical and legal obligations.