Page 9 of 20
IM3.7-14 | Pneumonia Diagnostic Testing — SDL Guide (Part 2)
Arterial Blood Gas: Collection Technique and Interpretation
The arterial blood gas (ABG) is one of the most information-dense investigations available in acute medicine — a single sample from a single blood draw yields information about oxygenation, ventilation, acid-base balance, and metabolic status simultaneously. In pneumonia, the ABG is indicated whenever there is clinical concern for respiratory failure: SpO2 <94% on room air, respiratory rate ≥30/min, suspected hypercapnic respiratory failure (in known COPD), assessment of response to oxygen therapy, or before and after initiating ventilatory support. The NMC competency IM3.8 requires you to demonstrate correct ABG collection technique on a mannequin, and IM3.9 requires you to interpret the report — both skills are tested in clinical examinations.
ABG collection technique (radial artery — most commonly used site): Before collection, perform the modified Allen's test — compress both the radial and ulnar arteries simultaneously while the patient opens and closes their fist several times to exsanguinate the hand; then release the ulnar artery while maintaining radial compression; if the hand flushes pink within 5–7 seconds (normal), the ulnar artery can maintain hand perfusion if the radial artery is damaged, and it is safe to proceed. A negative Allen's test (failure to flush within 7 seconds) indicates inadequate ulnar collateral circulation; consider the femoral or brachial artery instead. The technique: position the patient's wrist in extension (use a rolled towel under the wrist) to bring the radial artery to the surface; palpate the radial pulse approximately 1–2 cm proximal to the radial styloid; clean with 70% alcohol and allow to dry; use a pre-heparinised ABG syringe (commercially supplied, contains dried lithium heparin); insert the needle at a 45–60° angle, bevel up, against the direction of arterial blood flow (i.e., angling slightly proximally); a pulsatile blood column will fill the syringe under arterial pressure — no aspiration required; collect 1–3 mL; immediately apply firm pressure to the puncture site for a minimum of 5 minutes (extend to 10–15 minutes for anticoagulated patients or thrombocytopaenic patients); expel all air bubbles from the syringe immediately (air equilibrates with blood and will falsely raise PO2 and lower PCO2); cap the syringe and roll between palms to mix; transport on ice and process within 15 minutes. Complications: arterial spasm (transient, resolves spontaneously), haematoma (minimised by adequate post-procedure pressure), thrombosis (rare with good technique), and infection (minimised by sterile technique).
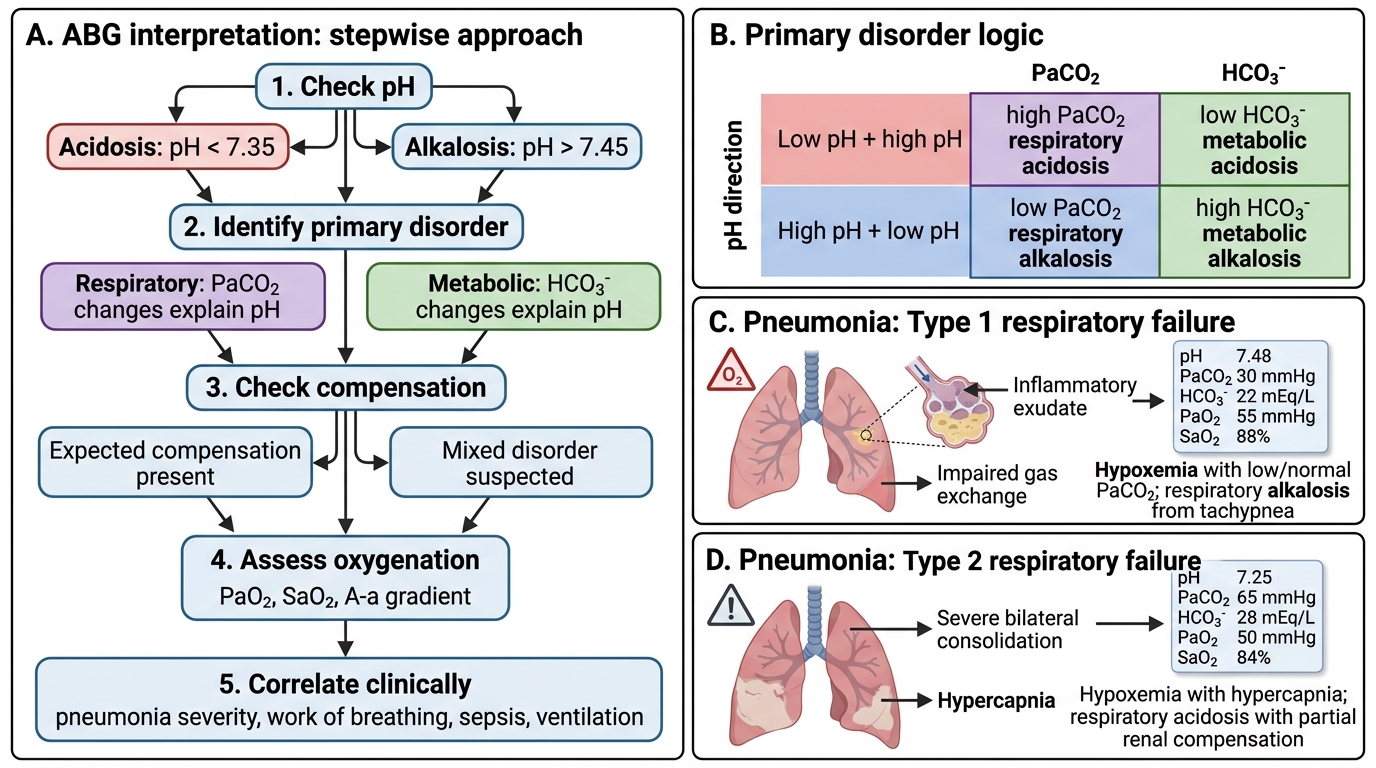
ABG interpretation — the five-step approach: The disciplined interpretation of an ABG requires a systematic sequence that prevents common errors of premature pattern-matching. Step 1 — Check the pH: pH <7.35 = acidosis; pH >7.45 = alkalosis. Step 2 — Determine the primary disorder: if pH is acidotic, check PaCO2 — if PaCO2 is elevated (>45 mmHg) the primary disorder is respiratory acidosis; if PaCO2 is normal or low and HCO3 is low, the primary disorder is metabolic acidosis. If pH is alkalotic, check PaCO2 — if PaCO2 is reduced (<35 mmHg) the primary disorder is respiratory alkalosis; if PaCO2 is normal or high and HCO3 is elevated, the primary disorder is metabolic alkalosis. Step 3 — Check for compensation: the body's compensatory responses are predictable. In respiratory acidosis, the kidneys retain bicarbonate (HCO3 rises); in respiratory alkalosis, the kidneys excrete bicarbonate (HCO3 falls). In metabolic acidosis, hyperventilation reduces PaCO2; in metabolic alkalosis, hypoventilation raises PaCO2. Step 4 — Assess oxygenation: PaO2 and SaO2; calculate the A-a (alveolar-arterial) oxygen gradient where needed (particularly for PCP diagnosis). Step 5 — Correlate with the clinical picture.
In pneumonia, the typical ABG patterns are: (a) Type 1 respiratory failure (commonest) — PaO2 <60 mmHg with low/normal PaCO2; the hypoxaemia from V/Q mismatch drives hyperventilation, which reduces PaCO2 to below normal — producing a respiratory alkalosis (pH elevated, PaCO2 low, HCO3 mildly reduced as compensatory renal response begins); (b) Type 2 respiratory failure (severe pneumonia with muscle fatigue or underlying COPD) — PaO2 <60 mmHg with PaCO2 >50 mmHg; respiratory acidosis (pH reduced, PaCO2 elevated); this pattern signals impending or established ventilatory failure and is a key trigger for escalation to NIV or mechanical ventilation; (c) Mixed picture in septic patients — a combined respiratory alkalosis from hyperventilation and metabolic acidosis from lactic acidosis of sepsis.
ABG Interpretation in Pneumonia
Pleural Aspiration: Technique and Fluid Interpretation
Pleural aspiration (thoracentesis) serves two purposes in pneumonia management: diagnostic — analysis of pleural fluid to determine if it requires drainage (empyema versus simple parapneumonic effusion), and therapeutic — removal of fluid for symptomatic relief of breathlessness in large effusions. The NMC competency IM3.10 requires demonstration of correct technique on a mannequin; IM3.11 requires knowledge of which tests to perform on the fluid and ability to interpret the results. Both competencies are tested in clinical examinations.
Pre-procedure requirements: Confirm the presence, size, and location of the effusion by clinical examination (stony dullness, reduced breath sounds, shifting dullness) and CXR (blunting of the costophrenic angle on PA CXR — typically visible when effusion volume exceeds 250–300 mL; lateral decubitus CXR detects smaller effusions ≥50 mL and confirms free-flowing vs loculated). Ultrasound guidance is strongly preferred and reduces complication risk — it is now the standard of care in most institutions. Consent the patient.
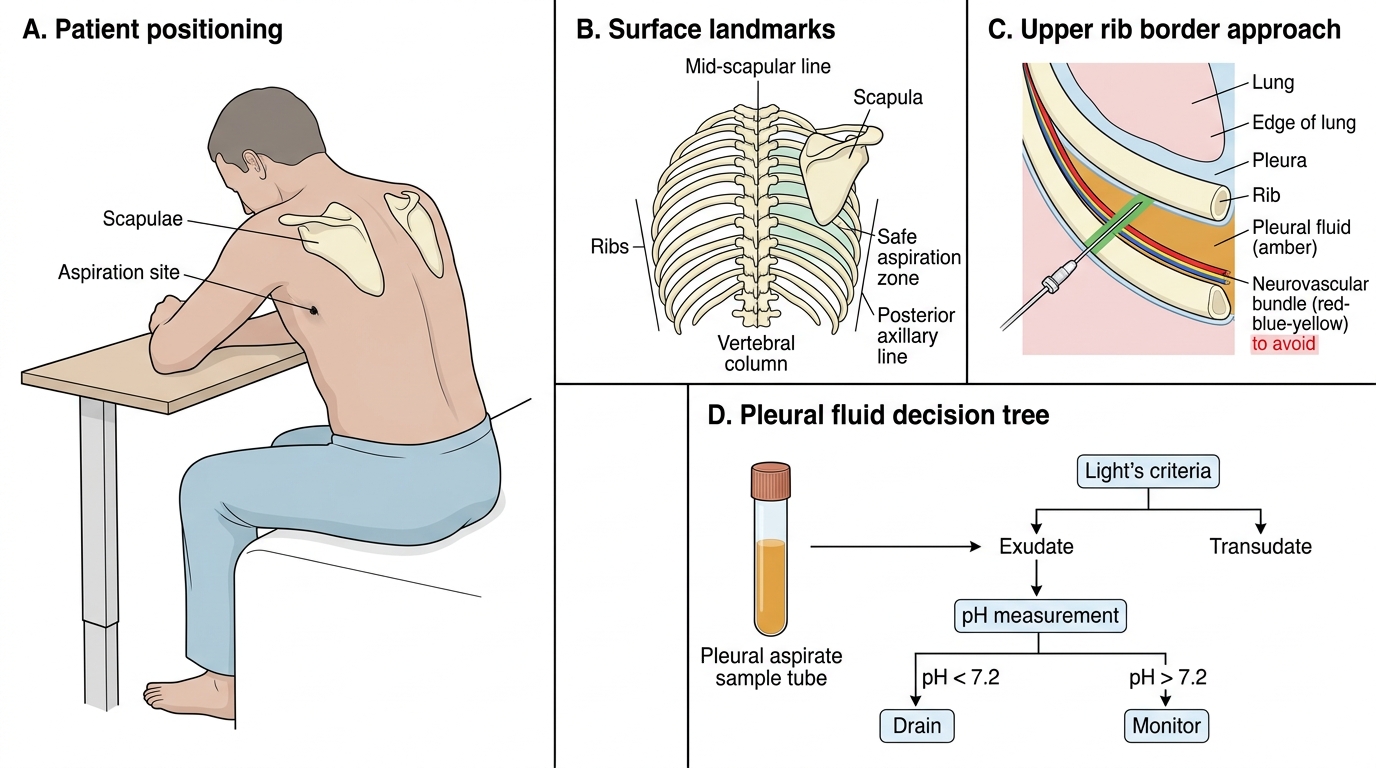
Technique (landmark-guided, posterior approach): Position the patient sitting upright, leaning slightly forward with arms supported. Identify the level of maximal dullness on percussion — the aspiration site is one intercostal space below this level, in the mid-scapular line or posterior axillary line to avoid major vessels. The needle is inserted at the upper border of the lower rib to avoid the neurovascular bundle (intercostal nerve, artery, and vein run along the inferior border of the rib — a subcostal approach would risk vascular injury and haemothorax). Infiltrate local anaesthetic (2% lignocaine) from skin down to the parietal pleura — the pleura itself is pain-sensitive (the parietal pleura has pain receptors; the visceral pleura does not) and adequate local anaesthesia is essential. Insert the aspiration needle (typically a 21G needle on a 20–50 mL syringe) perpendicular to the chest wall at the upper rib border. Aspirate 20–50 mL for diagnostic purposes; if therapeutic drainage is needed, a larger-bore cannula (using Seldinger technique or a commercial pleural aspiration kit) is required for adequate drainage.
Pleural fluid analysis — which tests to order and how to interpret them: Send the aspirated fluid for: (1) Appearance — straw-coloured (simple exudate/transudate), turbid or cloudy (exudate, inflammatory, infected), frank pus (empyema — stop immediately, arrange intercostal tube drainage), blood-stained (haemothorax, malignancy, PE with infarction, traumatic tap); (2) Protein — use Light's criteria to distinguish exudate from transudate: exudate if ANY of: pleural fluid protein/serum protein >0.5; OR pleural fluid LDH/serum LDH >0.6; OR pleural fluid LDH >2/3 of the upper limit of normal serum LDH. Parapneumonic effusion = exudate. Transudate (protein <3 g/dL, Light's criteria not met) suggests heart failure, cirrhosis, or nephrotic syndrome — not an infected effusion. (3) Glucose — low pleural fluid glucose (<2.2 mmol/L or pleural/serum glucose <0.5) indicates empyema, malignancy, TB, or rheumatoid pleuritis; simple parapneumonic effusion has near-normal glucose; (4) pH — the most important parameter for deciding drainage: pH <7.2 = complicated parapneumonic effusion or empyema requiring drainage; pH 7.2–7.45 = simple effusion, may respond to antibiotics alone; pH >7.45 = transudate; (5) LDH — elevated in exudates; >1000 IU/L is a strong indicator of empyema or complicated parapneumonic effusion; (6) Microscopy, culture, and sensitivity (MC&S) — Gram stain and culture for bacterial identification; (7) Cytology — for malignant cells (not acute management but important if effusion is unexplained); (8) AFB smear and mycobacterial culture — for TB pleuritis (particularly in India).
Complications of pleural aspiration: Pneumothorax (most common — from lung puncture; prevented by ultrasound guidance and correct site selection; post-procedure CXR is mandatory); haemothorax (from intercostal vessel injury — avoided by upper rib border approach); vasovagal reaction (patient should be warned and positioned safely); re-expansion pulmonary oedema (rare, after removal of very large volumes in one sitting — limit drainage to <1.5 L per session).
Pleural Aspiration Technique and Fluid Analysis
SELF-CHECK
Pleural fluid aspirated from a patient with right lower lobe pneumonia and a right-sided effusion has the following results: protein 4.8 g/dL (serum protein 6.5 g/dL), LDH 1,200 IU/L (serum LDH 280 IU/L), glucose 1.1 mmol/L, pH 7.10, appearance turbid yellow. What is the MOST appropriate immediate management?
A. Continue IV antibiotics and repeat aspiration in 48 hours
B. Increase the antibiotic dose and reassess in 24 hours
C. Arrange intercostal tube drainage immediately
D. Perform a repeat CXR and observe for 12 hours
Reveal Answer
Answer: C. Arrange intercostal tube drainage immediately
This pleural fluid meets multiple criteria for empyema or complicated parapneumonic effusion requiring immediate drainage: pH <7.2 (7.10 is critically low — the key drainage trigger), glucose <2.2 mmol/L (1.1 mmol/L), LDH >1000 IU/L (1200 IU/L), and turbid appearance (indicating frank infection/pus). Light's criteria also confirm exudate. Antibiotics alone will NOT clear a loculated empyema — the antibiotic cannot adequately penetrate the organised pleural pus, and undrained empyema has a mortality risk. Intercostal tube drainage is the mandatory immediate step, typically using a 14–28 Fr chest drain placed under ultrasound guidance.
HIV Testing, ABG Interpretation in Context, and Advanced Diagnostics
HIV testing in the context of pneumonia workup is not optional in the Indian clinical setting — it is a standard of care. HIV co-infection fundamentally alters the diagnostic and management approach to pneumonia, and many patients are unaware of their HIV status at the time of presentation. NACO guidelines recommend provider-initiated testing and counselling (PITC) — HIV testing offered by the clinician as a routine part of care in all patients presenting with pneumonia, TB, or other indicator diseases, with pre-test information (brief, not lengthy counselling) and post-test counselling based on the result. The HIV rapid test (a finger-prick test using a validated rapid antibody/antigen assay) is available at all integrated counselling and testing centres (ICTCs) attached to government hospitals and provides a result in 15–20 minutes. Confirming HIV status in a patient with severe pneumonia changes three things immediately: (1) the differential diagnosis expands to include PCP, disseminated TB, and fungal infections; (2) empirical antibiotic cover must address PCP if CD4 is likely <200 (add high-dose co-trimoxazole); (3) ART initiation should be planned, including the timing relative to treatment of the opportunistic infection.
Contextual ABG interpretation — connecting the numbers to the patient: The five-step approach described in the previous section must always be applied with the clinical context. Three scenarios specific to pneumonia are worth consolidating. First, a patient with normal SpO2 on room air but dyspnoea and tachypnoea: the ABG may show a respiratory alkalosis (low PaCO2, high pH, normal PaO2) — this is the early compensatory pattern of hypoxaemia that the SpO2 may not yet reflect, or of early metabolic acidosis that the patient is hyperventilating to compensate; a normal SpO2 does NOT exclude early respiratory failure. Second, a patient with known COPD on supplemental oxygen, drowsy, with SpO2 of 94% on 6 L/min: the ABG may show type 2 respiratory failure with a rising PaCO2 — the high oxygen delivery has suppressed the hypoxic drive in this COPD patient, reducing minute ventilation and causing CO2 to accumulate; reduce the FiO2 to target SpO2 88–92% and consider NIV. Third, a patient in septic shock with pneumonia — the ABG shows a mixed picture: respiratory alkalosis (from fever-driven hyperventilation) combined with metabolic acidosis (from lactic acidosis of tissue hypoperfusion); the pH may be near-normal despite both processes operating simultaneously (partially compensated) — do not be reassured by a pH in the 7.35–7.45 range if the PaCO2 is low and the bicarbonate is also low, as this represents a stressed physiological state that may decompensate rapidly.
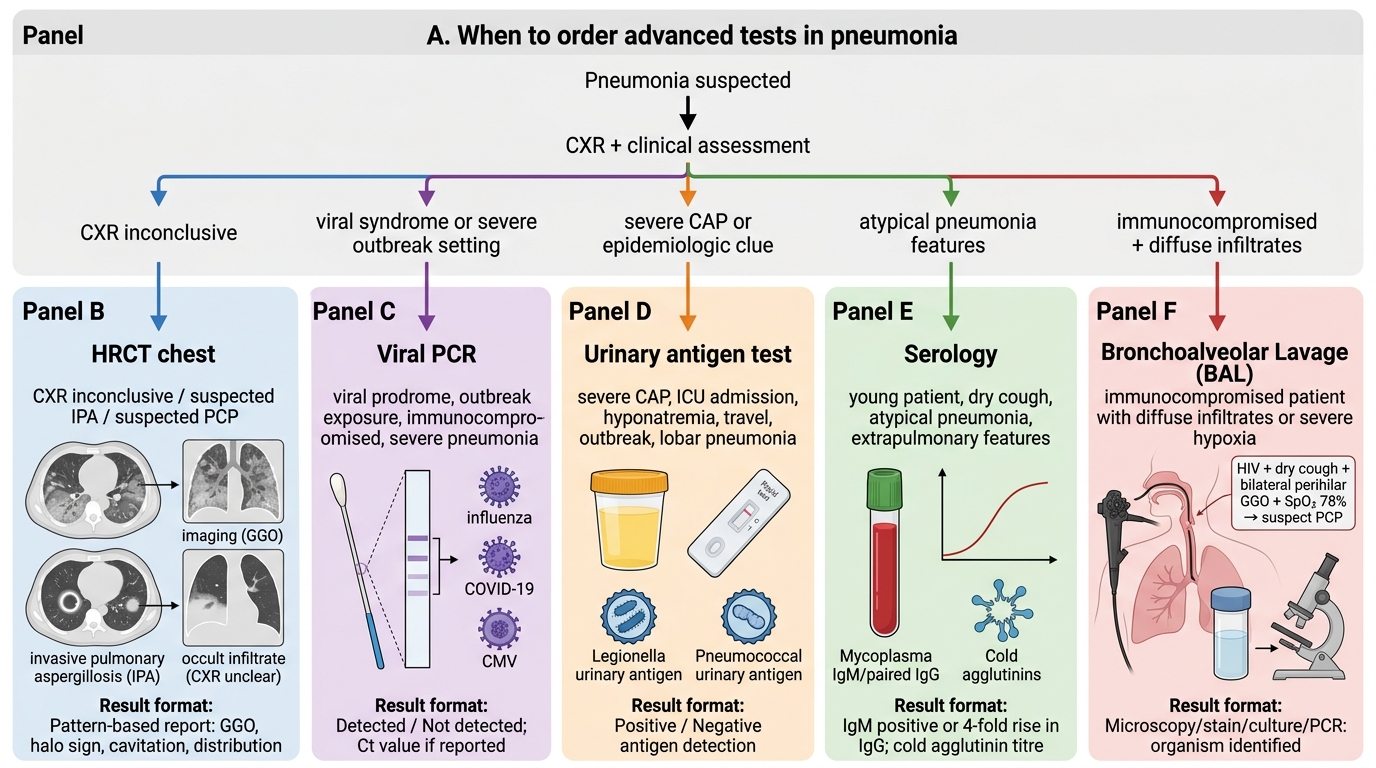
Indications for and interpretation of advanced diagnostic tests (IM3.14): Several investigations are not part of the routine workup but are indicated in specific clinical scenarios. HRCT (high-resolution computed tomography) of the chest is indicated when: CXR appears normal but there is strong clinical suspicion of pneumonia (particularly PCP, atypical pneumonia, early IPA); when the CXR pattern is equivocal and distinguishing pneumonia from an alternative diagnosis (pulmonary embolism, malignancy, COP) will change management; when complications such as cavitation, early abscess, or pericardial/mediastinal involvement need characterisation; and when a patient does not respond to empirical antibiotics and the differential needs broadening. HRCT is more sensitive than CXR for all pneumonia patterns and for identifying the halo sign (IPA), ground-glass in PCP, and mosaic attenuation in hypersensitivity pneumonitis. Viral cultures and PCR: Indicated during epidemic and pandemic situations (influenza PCR during influenza season, SARS-CoV-2 PCR), in immunocompromised patients with diffuse bilateral infiltrates (CMV PCR in transplant recipients), and when routine bacterial investigations are non-diagnostic. Viral PCR from nasopharyngeal swab or BAL specimen is the diagnostic method of choice — culture is time-consuming and not practical for acute management. Specialised serology: Legionella urinary antigen (rapid, detects Legionella pneumophila serogroup 1 in urine — results in 15 minutes, covers ~80% of cases); pneumococcal urinary antigen (rapid, sensitive for pneumococcal pneumonia and positive even after antibiotic treatment has begun); Mycoplasma serology (IgM antibodies; a fourfold rise in paired acute/convalescent titres is diagnostic); cold agglutinins (positive in ~50% of Mycoplasma CAP — a bedside semi-quantitative test where a few drops of blood in a blue-top tube placed on ice will agglutinate at 4°C but disaggregate at 37°C). Bronchoalveolar lavage (BAL) via flexible bronchoscopy is the definitive diagnostic procedure for immunocompromised patients with diffuse pulmonary infiltrates (PCP diagnosis by immunofluorescence or PCR; IPA by galactomannan in BAL fluid; CMV by shell vial culture; TB in non-expectorating patients).
Advanced Diagnostic Tests in Pneumonia
SELF-CHECK
A 44-year-old man with newly diagnosed HIV (CD4 count not yet known) presents with 2 weeks of progressive breathlessness, dry cough, and bilateral perihilar ground-glass opacities on CXR. His SpO2 is 78% on room air. His ABG shows: pH 7.50, PaO2 42 mmHg, PaCO2 29 mmHg, HCO3 22 mEq/L. How should this ABG be interpreted?
A. Metabolic alkalosis with adequate oxygenation
B. Respiratory acidosis with type 2 failure — start NIV
C. Respiratory alkalosis with type 1 failure — hypoxia driving hyperventilation
D. Mixed respiratory and metabolic acidosis
Reveal Answer
Answer: C. Respiratory alkalosis with type 1 failure — hypoxia driving hyperventilation
Step-by-step: pH 7.50 = alkalosis. PaCO2 29 mmHg (low) = respiratory alkalosis (primary respiratory process). HCO3 22 mEq/L = normal (no significant metabolic component). Oxygenation: PaO2 42 mmHg = severe hypoxia (normal 80–100). This is type 1 respiratory failure (hypoxia with low PaCO2) — the severe hypoxia from V/Q mismatch is driving hyperventilation, which reduces PaCO2 and produces a respiratory alkalosis. This is the classic PCP pattern in HIV: severe hypoxia, dry cough, bilateral interstitial infiltrates, and an ABG showing type 1 failure with respiratory alkalosis. PaCO2 is LOW (not raised), so this is not type 2 failure and NIV for hypercapnia is not indicated; supplemental oxygen is the priority, plus empirical high-dose co-trimoxazole for PCP.