Page 10 of 20
IM3.7-14 | Pneumonia Diagnostic Testing — SDL Guide (Part 3)
Applied Practice: Clinical Decision-Making from Diagnostic Results
Applied diagnostic practice in pneumonia means translating each investigation result into a specific management decision — not collecting data passively, but using each result to answer a clinical question and take action. This section consolidates the diagnostic skills through the lens of the most common clinical decision points encountered in day-to-day ward and emergency medicine practice in India.
Decision 1 — Does this patient need to be admitted, and to which level of care? This is answered by the CURB-65 score derived from clinical examination (RR, BP, mental status) and the urea from the blood workup. A CURB-65 of 0–1 supports outpatient treatment with oral antibiotics. A score of 2 warrants a judgment call on admission, particularly in elderly patients or those with comorbidities. A score of ≥3 mandates hospital admission; a score of ≥4 prompts immediate assessment for ICU-level care. The ABG is the confirmatory investigation for respiratory failure severity — a PaO2 <60 mmHg on room air or PaCO2 >50 mmHg (type 2 failure) with pH <7.35 are ICU-transfer triggers. In practice, run the CURB-65 as soon as the urea result returns, because the score may change the care plan before any antibiotic decision is needed.
Decision 2 — Should the empirical antibiotic be changed at 48–72 hours? This decision hinges on two inputs: clinical response (fever, respiratory rate, SpO2 trajectory) and microbiological results (blood cultures, sputum culture). If blood cultures grow Streptococcus pneumoniae susceptible to penicillin, de-escalate from broad-spectrum ceftriaxone + azithromycin to IV benzylpenicillin or oral amoxicillin — this is antibiotic stewardship in direct action. If the blood culture result is a single-bottle CNS, discard as contamination and continue current treatment. If the culture grows MRSA, add vancomycin (target trough 15–20 mg/L) or switch to linezolid. If no organism is identified but the patient is improving, continue empirical cover to 5 days (non-severe CAP) or 7 days (severe CAP). If the patient is NOT improving at 48–72 hours despite appropriate empirical cover, this is a diagnostic red flag — revisit the differential and consider: empyema requiring drainage (check pleural fluid pH if not already done), TB (send GeneXpert), malignancy (HRCT), resistant organism, or a non-infectious diagnosis (COP, vasculitis).
Decision 3 — Does this effusion need to be drained? This is the most time-sensitive applied diagnostic decision. The pH of the pleural fluid is the single best discriminator: pH <7.2 = drain immediately; pH 7.2–7.45 = continue antibiotics and reassess at 24 hours; pH >7.45 = likely transudate, investigate for heart failure/cirrhosis rather than treating as empyema. In practice, if you aspirate turbid fluid or frank pus, do not wait for the pH result — arrange intercostal tube drainage immediately. The key operational principle is that a delay in draining an infected effusion allows fibrin organisation into a multiloculated empyema, which requires more invasive surgical intervention (video-assisted thoracoscopic surgery, VATS decortication) to manage.
Decision 4 — Does this patient need HIV testing? Apply PITC to all patients with pneumonia that is severe, atypical, or not responding to standard antibiotics. In practical terms: if a young adult presents with bilateral perihilar infiltrates and disproportionate hypoxia without an obvious community exposure history, offer HIV testing before continuing empirical antibiotic treatment, because PCP management (high-dose co-trimoxazole + adjunctive steroids if PaO2 <70 mmHg) is fundamentally different from bacterial CAP management and should begin as soon as the clinical picture suggests PCP.
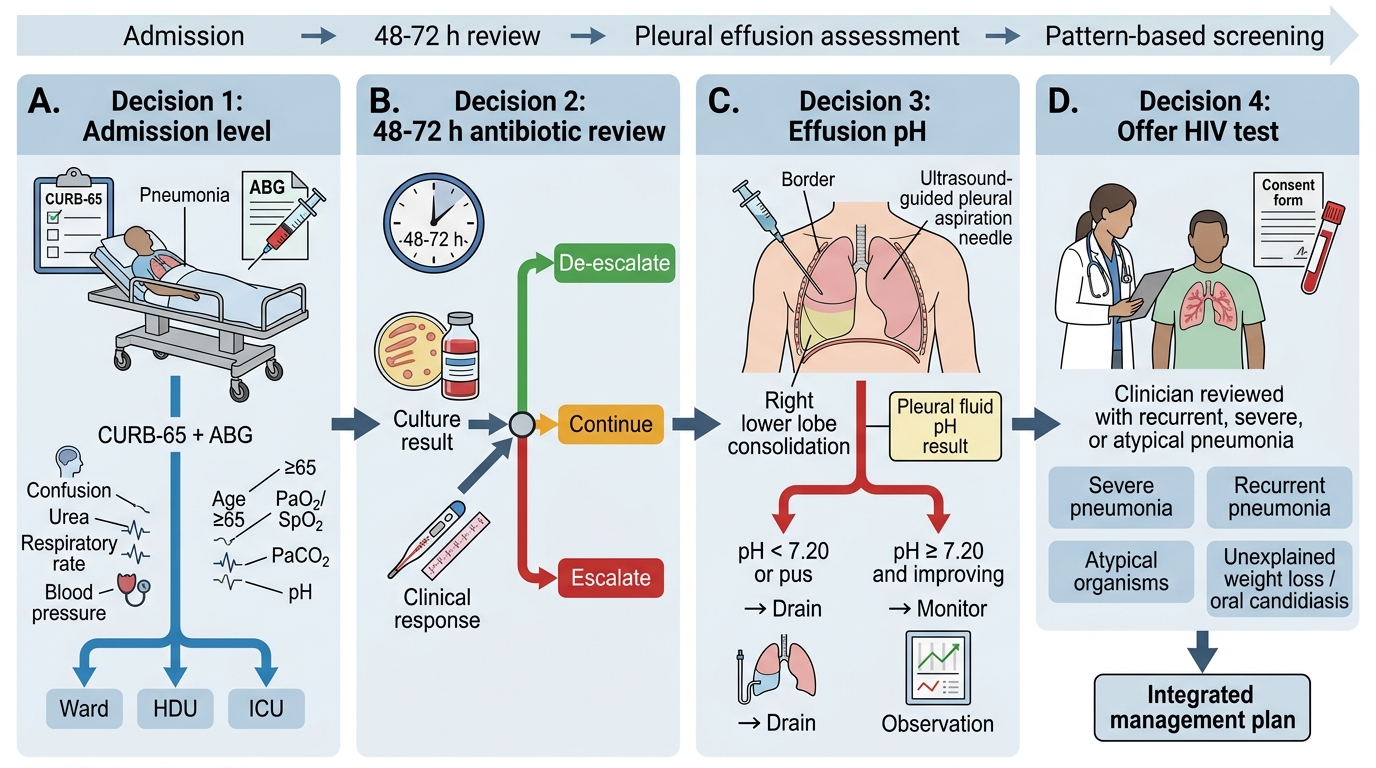
Four-Decision Algorithm for Admitted Pneumonia
Self-Assessment: Integrating Diagnostic Skills
The eight competencies covered in this module form an integrated diagnostic toolkit — no single test is sufficient alone, and the value of each test depends on the clinical context in which it is ordered and the skill with which it is interpreted. A CXR showing right lower lobe consolidation is only diagnostically complete when paired with a CBC showing leucocytosis, a sputum Gram stain confirming pneumococcal morphology, blood cultures drawn before antibiotics, and an ABG that confirms or excludes respiratory failure. Each piece of data refines the clinical picture and guides a specific management decision. The self-assessment below tests your ability to apply the diagnostic skills in an integrated manner — selecting the appropriate test for the clinical scenario, interpreting the result correctly, and determining the management implication.
This integration of clinical skills is particularly important for the procedural components: the ABG must be collected correctly (modified Allen's test, upper rib border for pleural aspiration) because a technically flawed specimen gives false results; a sputum sample incorrectly collected yields salivary flora instead of respiratory pathogens; blood cultures drawn after antibiotics may be negative despite true bacteraemia. The procedural rigour underlying each investigation is as important as the interpretation of its result, and this is what the NMC competency framework means by the SH (Skills and Handling) level.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
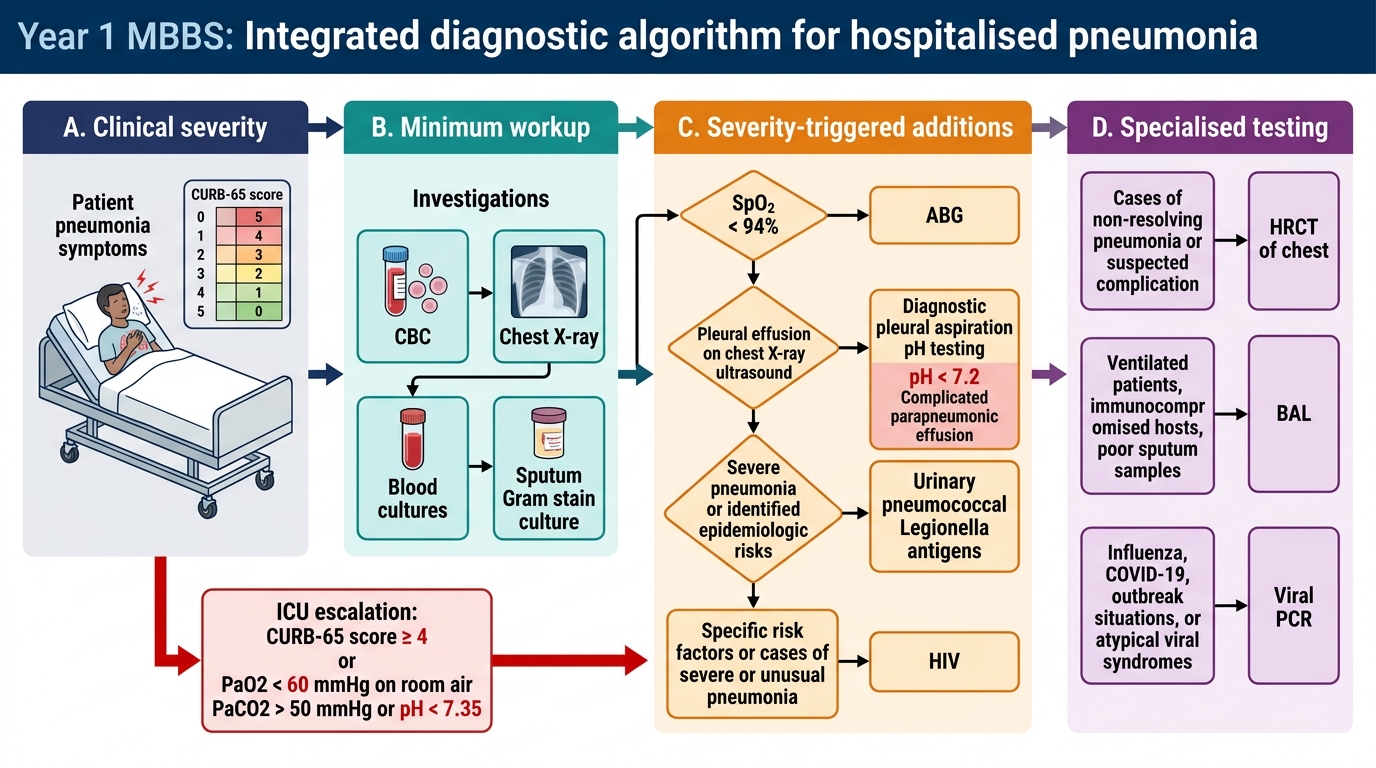
Integrated Diagnostic Algorithm for Hospitalised Pneumonia
Key take-aways for self-assessment:
1. Sputum quality check: always verify ≥25 PMNs and <10 squamous epithelial cells before accepting a sputum Gram stain report as valid.
2. Modified Allen's test is performed before EVERY radial artery ABG — even in a familiar patient — because radial artery patency can change.
3. Pleural aspiration pH <7.2 = drain. This is a threshold decision, not a judgment call — there is no role for observation once pH is below 7.2.
4. Blood cultures: two sets, two sites, both before antibiotics; S. aureus and S. pneumoniae are NEVER contaminants.
5. ABG type 1 failure in pneumonia = respiratory alkalosis + hypoxia (PaCO2 low, pH high, PaO2 low). Type 2 = respiratory acidosis + hypoxia (PaCO2 high, pH low, PaO2 low) — this signals ventilatory failure.
6. In HIV-positive patients with bilateral perihilar infiltrates, the A-a gradient will be markedly elevated in PCP — if oxygen supplementation corrects SpO2 but A-a gradient remains wide, PCP should be aggressively treated empirically.
CLINICAL PEARL
The single most common error in pneumonia diagnostic practice is starting antibiotics before collecting microbiological specimens. In the urgency of treating a breathless, febrile patient, the sequence 'antibiotics first, cultures later' is intuitive but wrong — even one dose of a beta-lactam dramatically reduces the sensitivity of blood cultures and sputum culture for pneumococcus within hours. The correct sequence is: venepuncture for two blood culture sets → collect expectorated sputum specimen → THEN give the first antibiotic dose. This takes 5–10 minutes and does not meaningfully delay treatment. The yield from blood cultures post-antibiotics drops from ~25% to ~5% for pneumococcal bacteraemia. A missed opportunity to identify the pathogen means empirical broad-spectrum antibiotics are continued for 5–7 days instead of de-escalating to a narrow-spectrum penicillin at 48 hours — contributing to resistance, adverse drug effects, and Clostridium difficile risk. The rule is absolute: obtain cultures before antibiotics, not 'when convenient.' In a patient presenting in extremis where even 5 minutes matters (septic shock), blood cultures can be drawn concurrently with IV line insertion — the extra minute is always available.