Page 14 of 21
IM4.19-20 | Febrile Syndrome Treatment Communication — SDL Guide
Learning Objectives
- Develop an appropriate empiric treatment plan for a febrile patient based on clinical and immune status, pending definitive microbiological diagnosis
- Communicate to the patient and family the diagnosis, treatment rationale, expected course, danger signs, and follow-up plan in a case of prolonged or complex fever
INSTRUCTIONS
Empiric treatment of fever requires the ability to prioritise safety over elegance — starting treatment for the most dangerous probable diagnosis while still pursuing a definitive diagnosis. Communication requires translating clinical reasoning into language that the patient and family can understand and act on. This module develops both skills through framework, examples, and scenarios.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 10–11 — Fever management (textbook)
- API Textbook of Medicine, 10th ed., Ch. 3–4 — Treatment of fever (textbook)
- WHO Guidelines for the Treatment of Malaria, 3rd ed. 2015 (guideline)
- NTEP Operational Guidelines 2022 — Drug-sensitive TB treatment (guideline)
- Surviving Sepsis Campaign International Guidelines 2021 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM on a Monday. A 24-year-old man is brought to the emergency department by his mother. He is drowsy, temperature 40.2°C, blood glucose 48 mg/dL (hypoglycaemia), and his peripheral blood smear shows P. falciparum ring forms at 4% parasitaemia. His mother is terrified and asks you: 'What is happening to my son, is he going to die, and what are you going to do?' You have two simultaneous tasks: begin IV artesunate immediately (because this is severe falciparum malaria — hypoglycaemia + impaired consciousness = severity criteria), and communicate to a frightened mother what malaria is, what the next 24 hours will look like, and what signs to watch for. The treatment decision and the communication cannot be separated — the mother's understanding of the danger signs and her ability to call for help if her son deteriorates is part of the management plan. This module builds both skills.
WHY THIS MATTERS
Two-thirds of morbidity and mortality from febrile syndromes in India is attributable not to lack of available drugs, but to delayed diagnosis, incorrect empiric treatment, and failure of patients and families to recognise deterioration and seek care promptly. NMC competencies IM4.19 and IM4.20 address both contributors directly: empiric treatment must be precise enough to cover the most dangerous diagnosis without causing harm, and patient communication must be specific enough to create an actionable plan that the patient and family can execute. These are not peripheral 'soft skills' — they are core clinical competencies whose failure has measurable consequences in patient outcomes.
RECALL
Connect this SDL to the management principles from the Fever Foundations module. Recall that antipyretic therapy (paracetamol 500 mg–1 g four-to-six hourly, or ibuprofen 400 mg three times daily with food) provides symptomatic relief by blocking COX-2-generated PGE2, lowering the hypothalamic set-point, and reducing the subjective distress of fever — but antipyretics treat the symptom, not the cause. Recall that empiric antibiotics for sepsis (the Hour-1 bundle from SSC guidelines) must cover gram-negative Enterobacterales in community-acquired sepsis and add MRSA coverage in healthcare-associated cases. Recall that anti-TB therapy under NTEP is 2HRZE + 4HRE — two months of isoniazid + rifampicin + pyrazinamide + ethambutol (intensive phase), followed by four months of isoniazid + rifampicin + ethambutol (continuation phase), weight-band dosed in fixed-dose combinations. Recall that NACO ART guidelines define the first-line regimen for HIV as TDF + 3TC + DTG (tenofovir + lamivudine + dolutegravir) — a single daily pill that constitutes the standard of care.
Clinical Indication for Empiric Treatment in Febrile Syndromes
Empiric treatment is defined as the initiation of therapy for a probable diagnosis before microbiological confirmation is available. Its indication is driven by two parameters that must be weighed simultaneously: the probability of the diagnosis (how likely is this cause given the clinical picture?) and the cost of delay (what is the consequence of withholding treatment for 24–48 hours while awaiting cultures or results?). When both parameters are high — that is, when a dangerous diagnosis is clinically probable and the cost of a 24-hour delay is death or permanent disability — empiric treatment is not only justified but mandatory.
The key conditions in febrile syndrome practice that meet both criteria and therefore mandate empiric treatment include: (1) Suspected falciparum malaria with severity criteria (impaired consciousness, hypoglycaemia, severe anaemia, hyperparasitaemia ≥5%, acute kidney injury, pulmonary oedema, jaundice with evidence of haemolysis) — IV artesunate must be started immediately; a delay of even a few hours from severe malaria to treatment is associated with significantly increased mortality; (2) Bacterial meningitis (fever + signs of meningeal irritation + CSF showing neutrophilic pleocytosis and low glucose) — IV ceftriaxone (2 g twice daily) + IV dexamethasone must be started within one hour of the lumbar puncture result, or empirically before LP if there is clinical deterioration; (3) Sepsis and septic shock (the Hour-1 bundle: cultures first, then antibiotics within one hour); (4) Febrile neutropenia (ANC <500 + temperature ≥38.3°C — IV broad-spectrum antibiotics within one hour); (5) Rickettsial disease — scrub typhus in an endemic-zone patient with fever + headache + eschar (doxycycline 100 mg twice daily can be started on clinical grounds before serology returns — the clinical response within 24–48 hours is itself diagnostic); (6) Infective endocarditis with haemodynamic compromise (IV antibiotics after blood cultures are drawn, not after sensitivity reports).
Conversely, there are febrile syndromes where empiric therapy is actively harmful and must be withheld until a diagnosis is established: (1) FUO workup — empiric broad-spectrum antibiotics mask cultures and delay the diagnosis; empiric steroids for suspected autoimmune FUO are catastrophic if the true cause is TB or kala-azar; (2) Suspected TB — anti-TB therapy is a long-term commitment and should ideally be started on microbiological confirmation (CBNAAT/smear/culture) except when clinical deterioration makes diagnostic delay unacceptable.
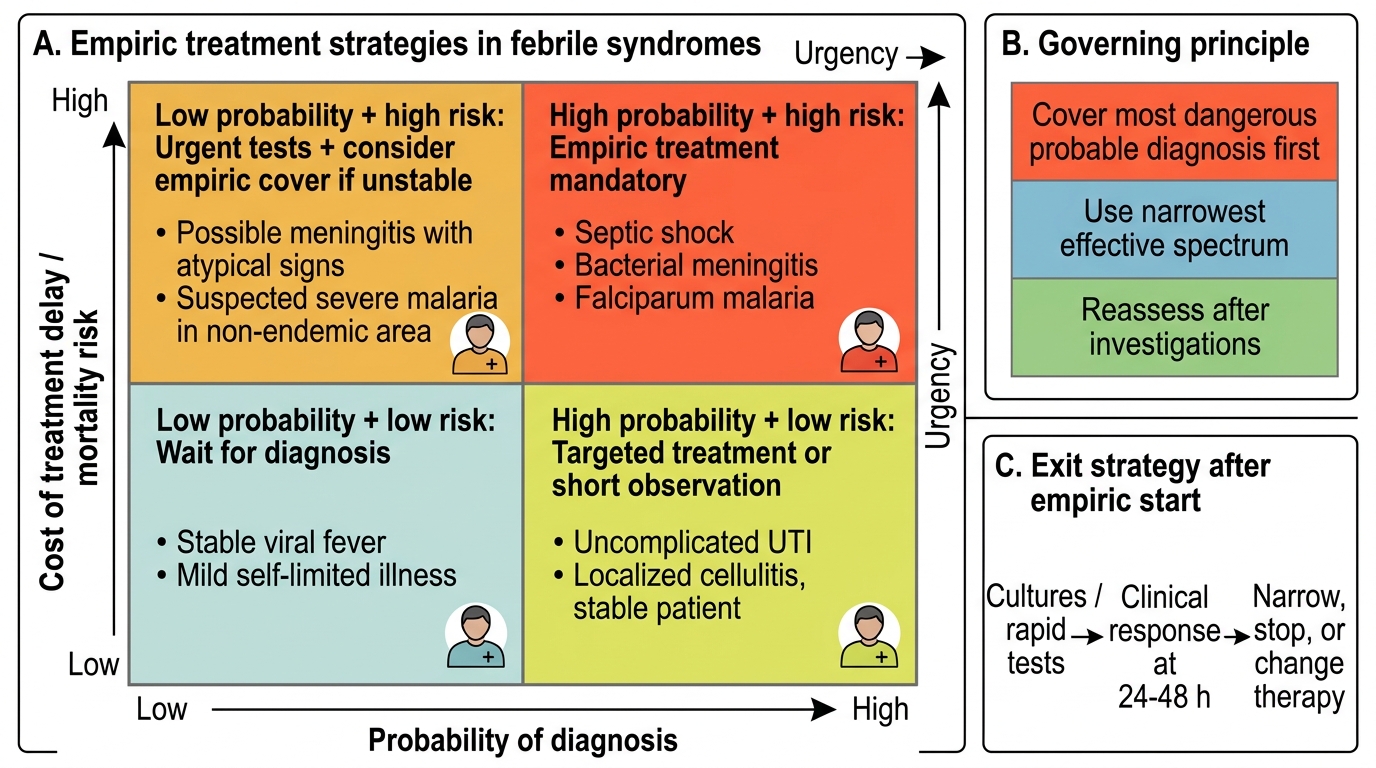
Empiric Treatment Decision Matrix in Febrile Syndromes
Governing Principles of Empiric Treatment
The governing principles of empiric treatment in febrile syndromes are a framework that determines both the content of the empiric regimen (which drugs to choose) and the duration and exit strategy (when to narrow, stop, or change therapy based on new information).
Principle 1 — Cover the most dangerous probable diagnosis first. The empiric regimen must treat the single most life-threatening disease in the differential. If the differential includes both a benign viral illness and falciparum malaria, the empiric decision is driven by malaria — not the viral illness. If the differential includes both dengue (supportive treatment only) and bacterial meningitis, the clinical picture determines which is more probable and more dangerous, and the empiric treatment targets meningitis.
Principle 2 — Use the narrowest effective spectrum. Broad-spectrum antibiotics that cover everything are appropriate only when the diagnostic uncertainty is genuinely broad (as in the first hour of septic shock before a focus is identified). As soon as a microbiological focus is identified or cultures return, therapy must be de-escalated to the narrowest effective agent — this reduces collateral damage (resistance selection, C. difficile superinfection, adverse drug effects). In India, the antibiogram at the local hospital is the most important reference for empiric choices — the empiric regimen that is appropriate for community-acquired pyelonephritis in Chennai differs from that in a Delhi ICU because the local resistance patterns differ.
Principle 3 — Reassess at 48–72 hours. Empiric treatment is not a set-and-forget decision. At 48–72 hours, culture and sensitivity results begin returning; clinical response (or lack thereof) provides additional information. The 48-hour reassessment should systematically address: has the patient improved (temperature trending down, haemodynamics stable, organ function improving)? Have microbiological results confirmed, excluded, or changed the diagnosis? Is there a reason to narrow the antibiotic spectrum? Is there a drug-resistant organism requiring escalation? Failure to improve at 48–72 hours should trigger a systematic re-evaluation — not automatic antibiotic escalation.
Principle 4 — Differentiate treatable from untreatable causes. Some infections respond to specific antimicrobials; others are managed supportively. Dengue has no antiviral therapy — management is fluid balance, monitoring for bleeding, and avoidance of NSAIDs and aspirin (which worsen thrombocytopaenia and bleeding risk); no antibiotic is indicated for uncomplicated dengue. Chikungunya is similarly supportive (NSAIDs are the mainstay for arthritic pain after fever resolves). Starting empiric antibiotics for dengue is a common error that adds toxicity without benefit and may delay recognition of the correct diagnosis.
Principle 5 — Host context modifies the empiric choice. An immunocompetent 25-year-old with community-acquired pneumonia requires different empiric coverage from a 65-year-old diabetic with healthcare-associated pneumonia. A neutropenic patient requires antifungal cover (IV fluconazole or caspofungin) after 5–7 days of antibiotics without clinical improvement. An HIV-positive patient with CD4 <100 and consolidation on CXR may have PJP requiring high-dose co-trimoxazole (trimethoprim-sulfamethoxazole 15–20 mg/kg/day in divided doses × 21 days) in addition to bacterial pneumonia coverage.
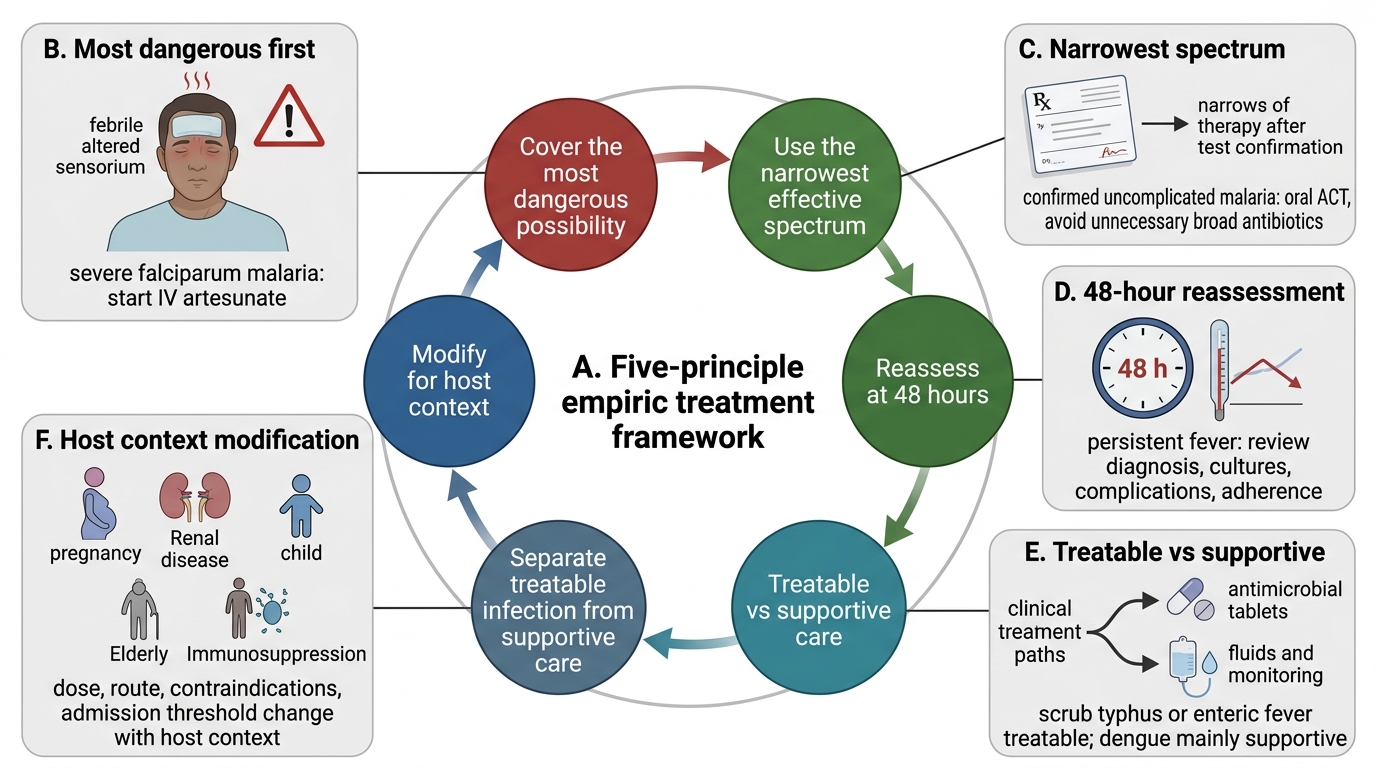
Five-Principle Framework for Empiric Fever Treatment
Procedure: Developing an Empiric Treatment Plan by Syndrome
This section details the empiric treatment plan for the five most important febrile syndromes encountered in Indian general medicine, applying the governing principles above. For each syndrome, the plan specifies the indication, drug choice, dose and route, duration, and the 48-hour review triggers.
1. Falciparum malaria (uncomplicated and severe):
Uncomplicated falciparum malaria (no severity criteria, able to take oral medication): artemether-lumefantrine (AL) — the recommended oral ACT under NVBDCP; weight-based dosing (four tablets twice daily for 3 days for adults >35 kg), taken with a fatty meal to enhance lumefantrine absorption. Alternative: artesunate-amodiaquine or dihydroartemisinin-piperaquine (state-programme dependent). Severe falciparum malaria (severity criteria present — impaired consciousness, acidosis, hypoglycaemia, hyperparasitaemia, severe anaemia, pulmonary oedema, renal failure, jaundice, haemoglobinuria, abnormal bleeding): IV artesunate 2.4 mg/kg at 0, 12, and 24 hours, then daily until oral therapy can be started (minimum 24 hours of IV artesunate); after clinical improvement, complete treatment with a full course of oral ACT. In India, IV quinine (infusion) is an alternative for severe malaria when IV artesunate is unavailable. Simultaneously manage complications: IV dextrose for hypoglycaemia (target blood glucose 4–8 mmol/L), careful fluid resuscitation for renal failure (avoid fluid overload in pulmonary oedema), anti-seizure drugs for cerebral malaria. Do NOT use corticosteroids in severe malaria — they increase mortality.
2. Enteric fever (typhoid and paratyphoid):
First-line antibiotic: IV/oral ceftriaxone 1–2 g daily for 10–14 days OR oral azithromycin 1 g daily × 5 days (for uncomplicated typhoid; high bioavailability). Fluoroquinolone resistance is now widespread in India — ciprofloxacin/norfloxacin should NOT be used empirically unless susceptibility is confirmed. Chloramphenicol, ampicillin, and co-trimoxazole are effective for susceptible strains but resistance is common. Duration and route depend on severity — severe typhoid with intestinal complications requires IV therapy and consideration of surgical consultation. Dexamethasone in high-dose (3 mg/kg initial dose, then 1 mg/kg four-hourly for 48 hours) reduces mortality in severe typhoid with altered consciousness or shock — a specifically evidence-based indication.
3. Sepsis (community-acquired focus unclear):
Following the Hour-1 Bundle: after two sets of blood cultures, IV broad-spectrum antibiotics immediately. Empiric choices in India depend on the likely source and local resistance patterns. For community-acquired sepsis without a clear focus: IV piperacillin-tazobactam 4.5 g eight-hourly covers gram-negative Enterobacterales and anaerobes; OR IV ceftriaxone 2 g daily + IV metronidazole 500 mg eight-hourly for abdominal or pelvic source. For healthcare-associated sepsis (patient hospitalised in the preceding 90 days, resident in a healthcare facility, on IV antibiotics in the preceding 30 days, or haemodialysis patients): broader coverage for ESBL-producing organisms and MRSA — IV meropenem 1 g eight-hourly + IV vancomycin 15–20 mg/kg eight-hourly (targeting trough 15–20 mg/L). Vasopressor (noradrenaline, first-line) started for MAP <65 mmHg despite 30 mL/kg crystalloid bolus.
4. Drug-sensitive pulmonary TB (NTEP DOTS regimen):
2HRZE + 4HRE (standard Category I regimen for new cases): Intensive phase (2 months): daily H (isoniazid) + R (rifampicin) + Z (pyrazinamide) + E (ethambutol) in fixed-dose combination tablets, weight-band dosed (e.g., for 55–70 kg: H300/R600/Z1500/E1100 mg/day). Continuation phase (4 months): daily H + R + E in fixed-dose combination. All doses are daily (NOT thrice-weekly intermittent — the obsolete intermittent DOTS regimen has been phased out by NTEP in favour of daily therapy). Treatment must be directly observed or supported to prevent non-adherence and resistance emergence. Note: drug interactions — rifampicin is a potent CYP450 inducer; it reduces plasma levels of warfarin, oral contraceptives, methadone, and many antiretrovirals; adjust or substitute as needed.
5. HIV antiretroviral therapy (NACO guidelines):
First-line ART: TDF/3TC/DTG — tenofovir disoproxil fumarate 300 mg + lamivudine 300 mg + dolutegravir 50 mg — all in a single daily fixed-dose combination tablet. When to start ART in HIV with TB co-infection: ART should be started within 2–8 weeks of starting anti-TB therapy (not simultaneously — the risk of IRIS and pill burden is high at simultaneous initiation; however, in patients with CD4 <50 cells/mm³, ART should be started as early as 2 weeks after TB treatment begins because the risk of AIDS-defining illness is high). Rifampicin-based anti-TB therapy lowers dolutegravir levels — dolutegravir dose is doubled to 50 mg twice daily when co-administered with rifampicin.
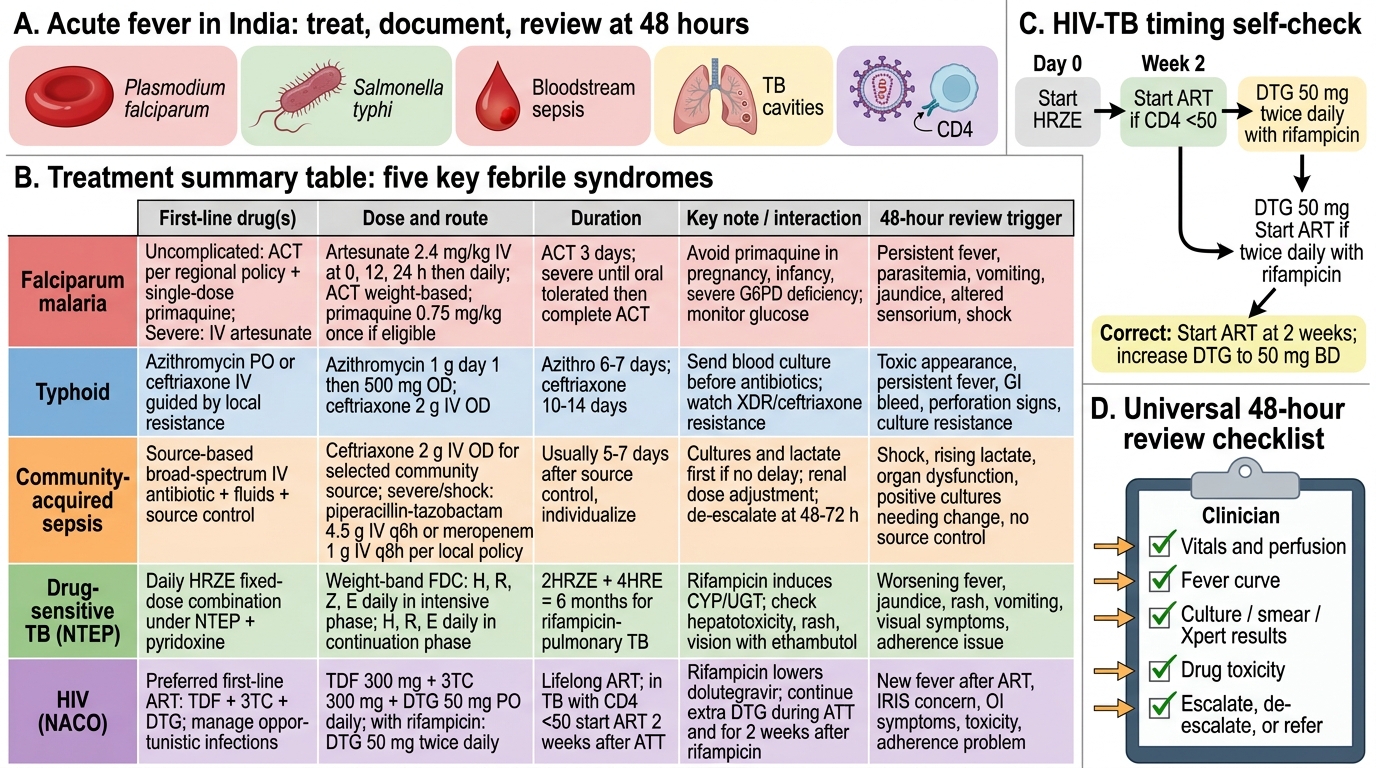
Treatment Summary for Five Febrile Syndromes in India
SELF-CHECK
A 35-year-old man is diagnosed with drug-sensitive pulmonary tuberculosis confirmed by Xpert MTB/RIF (rifampicin-sensitive). He is also HIV-positive with a CD4 count of 42 cells/mm³ and is currently not on ART. He is started on daily HRZE (isoniazid, rifampicin, pyrazinamide, ethambutol) under NTEP. When should ART be started, and how should dolutegravir dosing be adjusted?
A. ART should be started simultaneously with anti-TB therapy on day 1; dolutegravir standard dose 50 mg once daily
B. ART should be deferred until TB treatment is completed (6 months) to avoid drug interactions
C. ART should be started 2 weeks after TB therapy in view of CD4 <50; dolutegravir dose should be increased to 50 mg twice daily due to rifampicin induction
D. ART should be started 8 weeks after TB therapy; standard dolutegravir dose 50 mg once daily
Reveal Answer
Answer: C. ART should be started 2 weeks after TB therapy in view of CD4 <50; dolutegravir dose should be increased to 50 mg twice daily due to rifampicin induction
NACO guidelines recommend starting ART within 2 weeks of anti-TB therapy in HIV-TB co-infected patients with CD4 <50 cells/mm³, because of the high risk of AIDS-defining opportunistic infections at this level of immunosuppression. For CD4 50–200, ART is started within 8 weeks of anti-TB therapy. Deferring ART until TB treatment completion is inappropriate and dangerous at CD4 <50. Simultaneous initiation increases the risk of IRIS (immune reconstitution inflammatory syndrome) and pill burden, though it may be considered in very advanced disease under close monitoring. Rifampicin is a potent inducer of CYP3A4 and UGT1A1, which metabolises dolutegravir — rifampicin reduces dolutegravir plasma levels by approximately 75%, so the dose must be increased to 50 mg twice daily (total 100 mg/day) when co-administered with rifampicin-containing regimens.