Page 15 of 21
IM4.19-20 | Febrile Syndrome Treatment Communication — SDL Guide (Part 2)
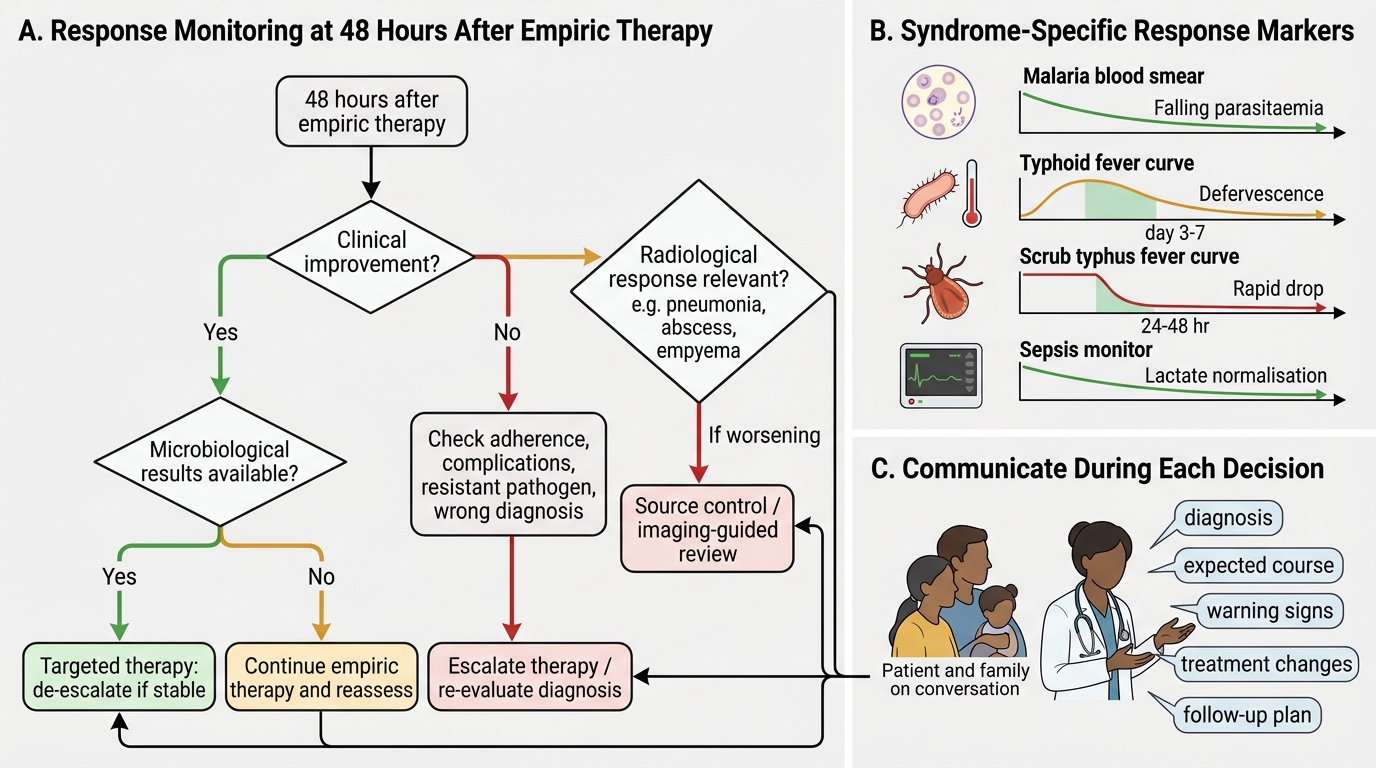
Interpretation: Assessing Response to Empiric Treatment
The assessment of response to empiric treatment is a systematic clinical reasoning process that determines whether the initial treatment hypothesis was correct, whether the regimen is adequate, and whether the diagnosis needs to be revisited. This assessment is performed at 48–72 hours after initiation of empiric therapy and should be documented explicitly in the case notes.
The parameters of treatment response assessment are: (1) Clinical response: is the patient's temperature trending down? Has the rigors/chills pattern changed? Are vital signs normalising (heart rate, blood pressure, respiratory rate)? Is the level of consciousness improving (in cerebral malaria, meningitis, or encephalopathy)? Is organ function improving — creatinine falling (in leptospirosis or septic AKI), bilirubin normalising (in severe malaria with jaundice), platelet count recovering (in dengue — note that platelets typically fall further during the critical phase before recovering in the recovery phase, so a still-falling count at 48 hours in dengue does not indicate treatment failure)? (2) Microbiological response: have culture results returned? Is the organism susceptible to the empiric regimen (de-escalate if so)? Is there a resistant organism requiring escalation? (3) Radiological response: in pneumonia, repeat chest X-ray at 48–72 hours is only useful if clinical response is inadequate — infiltrates normally take 7–14 days to clear on imaging even when the patient is clinically improving; early CXR reassessment is indicated for clinical failure, not routine follow-up.
In scrub typhus specifically, defervescence within 24–48 hours of starting doxycycline is both a therapeutic and diagnostic response — the rapidity of defervescence is so characteristic that a febrile patient who fails to defervesce within 48 hours of doxycycline therapy requires re-evaluation of the diagnosis. Similarly, in enteric fever treated with ceftriaxone, fever typically resolves within 3–7 days — a patient still febrile at day 7 on appropriate antibiotics raises the possibility of ceftriaxone-resistant Salmonella (send susceptibility testing), complication (intestinal perforation, haemorrhage), or an alternative diagnosis.
The formal assessment of treatment failure should be triggered by: no clinical improvement at 48–72 hours; clinical deterioration at any point; new complications developing after therapy is started; culture results demonstrating resistance; or a new finding on examination that changes the differential diagnosis (e.g., a new skin rash or lymphadenopathy appearing after antibiotic initiation, suggesting drug fever or a different underlying diagnosis).
Monitoring Treatment Response in Febrile Syndromes
Applied Practice: Patient and Family Communication in Prolonged Fever
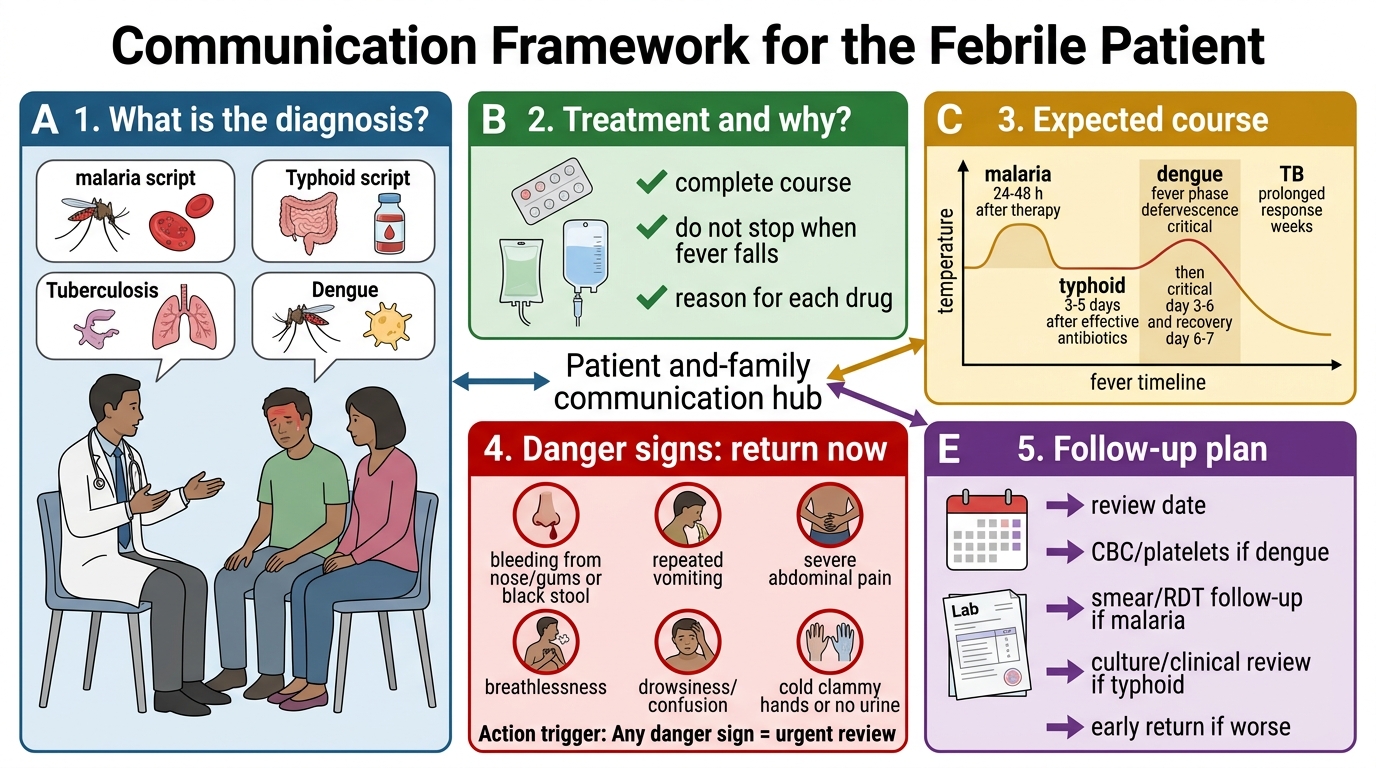
Patient and family communication (NMC competency IM4.20) is not a separate activity that follows clinical management — it is integrated into every step of the clinical encounter. This section provides a structured framework for communicating diagnosis, treatment, expected course, danger signs, and follow-up for the most common febrile syndromes in Indian practice.
The communication framework for a febrile patient and family comprises five components that should be covered in every significant discussion:
(1) What is the diagnosis? Explain in plain language what condition the patient has, avoiding medical jargon without oversimplifying. For malaria: 'Your son has a type of malaria called falciparum malaria, which is caused by a parasite that entered his bloodstream from a mosquito bite. This type can be serious if not treated quickly, which is why we are giving him treatment through the drip right now.' For typhoid: 'Your daughter has typhoid fever, which is caused by a bacteria called Salmonella that gets into the body from contaminated food or water. It is treatable with antibiotics, but it takes 7–10 days for the fever to come down fully.' Avoid vague statements like 'there is some infection' without naming the diagnosis.
(2) What is the treatment and why? Explain what drugs are being given and why — this improves adherence and builds trust. For TB: 'You will be taking four medicines for the first two months, and then three medicines for four more months — a total of six months. It is very important that you take them every day without missing a dose, because if you stop in the middle, the bacteria can become resistant to the medicines and much harder to treat.' For ART in HIV: 'This is one tablet that you take once a day, at the same time every day, for life. The medicine keeps the virus under control; stopping it allows the virus to grow again.' Use the tablet names in the language the patient understands where possible.
(3) What is the expected course? Set realistic expectations about how long fever will last, when the patient should start to feel better, and what is normal. For dengue: 'Dengue fever typically lasts 5–7 days. The fever may break in 2–3 days, but you may feel very weak for 1–2 weeks afterwards. The platelet count usually falls until day 5–7 and then rises — we will check it every day.' For typhoid treated with ceftriaxone: 'Fever usually starts to come down after 3–5 days of antibiotics, though some patients take 7 days. You should feel better by the end of the first week.' For severe malaria: 'The fever should come down within the first day of IV treatment, but we will need to monitor him closely for the next 48–72 hours for complications including kidney function, blood glucose, and blood count.'
(4) What are the danger signs to watch for? This is the most critical communication task — it empowers the family to recognise deterioration and seek help before an adverse outcome. Danger signs must be communicated in specific, observable terms, not abstract medical language. Examples: 'If your son becomes confused or you cannot wake him up easily, bring him to the hospital immediately.' (Cerebral malaria / encephalitis.) 'If you see any bleeding — from the gums, nose, or in the urine — call us or come to the hospital right away.' (Dengue haemorrhagic fever.) 'If he is still having fever after 5 days despite taking the antibiotics, please come back — do not wait.' (Typhoid treatment failure / complication.) 'If your daughter's breathing becomes fast or she feels very short of breath, or if her skin turns yellow, come immediately.' (Severe malaria complications.)
(5) What is the follow-up plan? Be specific about when to return: exact date, specific tests to be done, and what will be reviewed. 'Please come back in 3 days for a repeat blood test to check the platelet count. If there is any bleeding or if his condition gets worse before then, come immediately — do not wait for the 3-day appointment.' For TB: 'We will review you after 2 months to check your sputum and decide if we can reduce the number of medicines. Please bring your DOTS diary every visit.'
Communication in practice is not a monologue — it requires checking the patient's and family's understanding (teach-back technique: 'Can you tell me in your own words what the two warning signs are that should make you come back to the hospital immediately?') and answering questions honestly, including about prognosis.
Communication Framework for the Febrile Patient
SELF-CHECK
A patient with dengue fever (confirmed NS1 positive, day 4 of illness) has a platelet count of 48,000/mm³ today, down from 95,000 yesterday. He is alert, taking oral fluids, and has no bleeding. What is the correct communication to the family about his platelet count?
A. The platelet count is dangerously low and he needs platelet transfusion immediately
B. A falling platelet count in dengue during the critical phase (day 3–6) is expected; it will typically recover after day 6–7; the key is to watch for signs of active bleeding, not the platelet number alone
C. The falling count means the dengue is worsening and antibiotics should be added
D. He should be discharged home as the platelet count, though low, is not critical
Reveal Answer
Answer: B. A falling platelet count in dengue during the critical phase (day 3–6) is expected; it will typically recover after day 6–7; the key is to watch for signs of active bleeding, not the platelet number alone
In dengue fever, the platelet count typically falls progressively during the critical phase (days 3–6 of illness) due to immune-mediated platelet destruction and bone marrow suppression, then recovers spontaneously after defervescence (days 6–7). A platelet count of 48,000/mm³ on day 4 in an alert, haemodynamically stable patient without active bleeding does NOT by itself indicate a need for platelet transfusion — the WHO dengue guidelines recommend platelet transfusion only for significant active bleeding with severe thrombocytopaenia, not prophylactically based on platelet count alone. The key communication is: the platelet count falling now is the normal expected pattern of dengue; the critical thing to watch for is bleeding (gums, nose, skin purpura, blood in urine or stools). Antibiotics have no role in uncomplicated dengue (no bacterial co-infection). Discharging a day-4 dengue patient with falling platelets without adequate monitoring would be unsafe.
Self-Assessment: Empiric Treatment and Communication Scenarios
These scenarios test your ability to develop an empiric treatment plan and communicate it to the patient and family. For each scenario, identify the empiric treatment, the rationale, the expected timeline, and the specific danger signs to communicate.
Scenario A — Empiric treatment decision: A 40-year-old male labourer from Kerala was exposed to flood water during post-monsoon flooding 8 days ago. He now presents with 5 days of fever (39.5°C), severe myalgia, conjunctival suffusion, and jaundice (serum bilirubin 5.2 mg/dL, predominantly direct). He is alert, blood pressure 118/76 mmHg. Creatinine is 1.9 mg/dL (baseline normal). IgM ELISA for leptospirosis is pending. What is your empiric treatment, and why should you start before the serology returns?
Analysis: The clinical diagnosis is leptospirosis (Weil's disease) — flood exposure + fever + myalgia + conjunctival suffusion + hepatorenal involvement (jaundice + rising creatinine) is a pattern that is clinically diagnostic in an endemic setting (Kerala, post-flood). The serology (MAT is gold standard; IgM ELISA is more accessible) will take days to return a confirmed positive result. The rationale for empiric treatment before serology: leptospirosis responds best to antibiotics started early in the illness; outcome deteriorates with each additional day of untreated infection; the hepatorenal syndrome can progress to oliguric acute kidney injury, pulmonary haemorrhage (a life-threatening complication), and DIC within 24–48 hours of this stage. Treatment: IV benzylpenicillin 1.5 million units (1.5 MU) six-hourly for 7 days (for moderate-severe disease); alternatively, IV ceftriaxone 1 g daily. Oral doxycycline 100 mg twice daily is reserved for mild disease not requiring hospitalisation. Monitor urine output, creatinine, and respiratory status daily — deteriorating creatinine may require renal replacement therapy.
Scenario B — Patient communication: You have diagnosed a 52-year-old woman with smear-positive pulmonary TB. This is her first diagnosis of TB. She lives with her husband and two adult children. She is anxious and asks: 'Can I give this to my family? Why do I need to take medicines for 6 months? Can I stop when I feel better?'
Analysis: Communication points for this patient: (1) Infectivity and isolation: 'Pulmonary TB with positive sputum is infectious — the bacteria spread through the air when you cough, sneeze, or speak. You should cover your mouth when coughing, sleep in a well-ventilated room, and avoid being in crowded closed spaces for the first 2 weeks of treatment. After 2 weeks of daily treatment, your sputum will be much less infectious.' (2) Family contacts: 'Your husband and children should all come for a Mantoux test and chest X-ray within the next 2 weeks — this is a contact tracing protocol. If any of them have been infected, we can give preventive treatment.' (3) Duration of treatment: 'TB bacteria are very slow-growing and stubborn — it takes 6 months of medicines to kill all of them. If you stop when you feel better (usually after 2–3 months), the remaining bacteria can develop resistance to the medicines, making your TB much harder to treat.' (4) Adherence support: 'A health worker will visit you or call you to make sure you are taking the medicines every day under the NTEP DOTS programme — this is to help you, not to monitor you.' (5) Danger signs to return: 'Come back immediately if you develop jaundice (yellow eyes), skin rash, or visual changes — these may be side effects of the medicines that need to be addressed.'
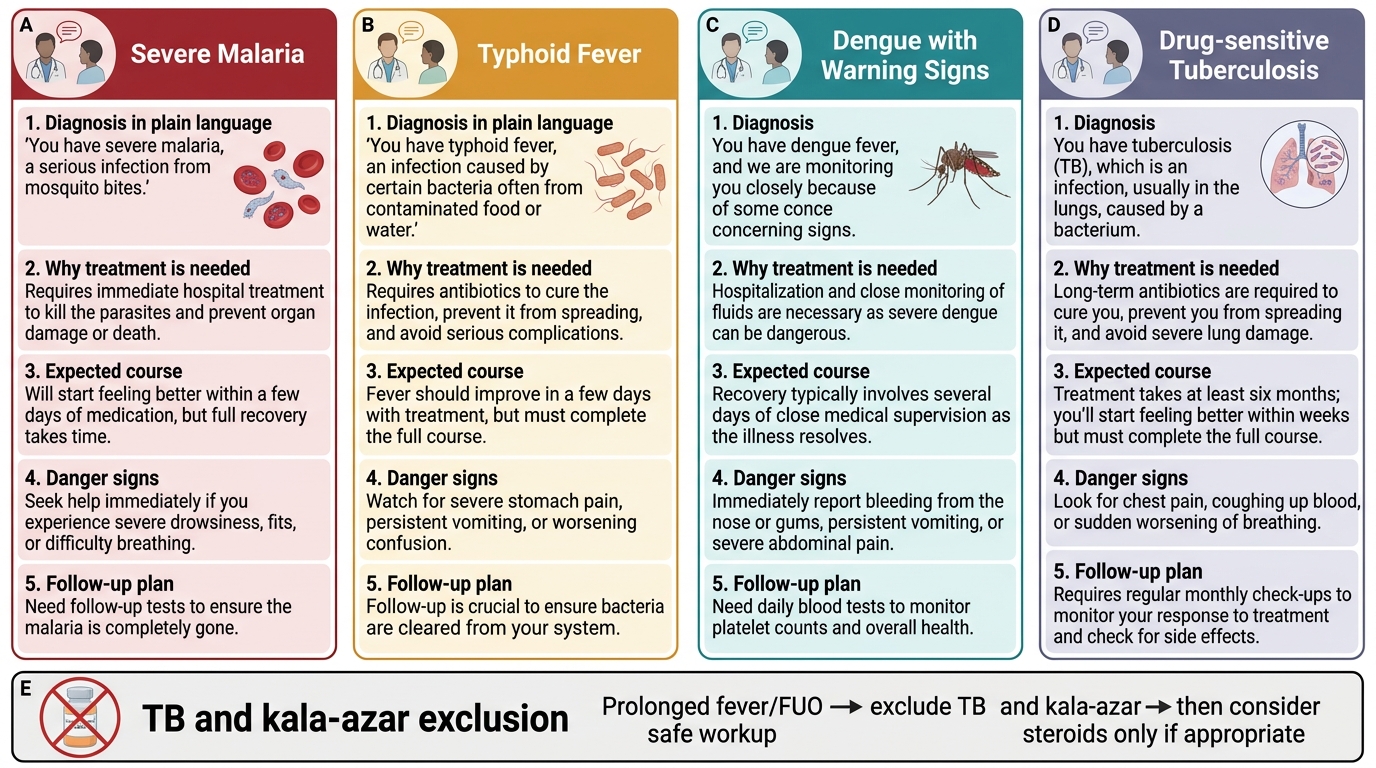
Patient Communication Script Cards for Febrile Syndromes
CLINICAL PEARL
The most important rule in empiric treatment of febrile syndromes is: never start empiric corticosteroids for prolonged fever without first actively excluding TB and kala-azar. Both conditions worsen catastrophically when immunosuppressed. This error is made repeatedly in Indian hospitals when a physician, frustrated by weeks of unexplained fever and suspecting an autoimmune aetiology, starts prednisolone before completing the infectious workup. The clinical response is initially dramatic (corticosteroids suppress the inflammatory fever whether the cause is autoimmune or infectious) — making the clinician believe the diagnosis was correct — until 2–4 weeks later when the patient presents with miliary TB, meningitis, or massively worsening kala-azar. This is a preventable catastrophe. Exclude TB (CBNAAT, IGRA, bone marrow if needed) and kala-azar (rK39, bone marrow) before starting steroids in any FUO patient.