Page 16 of 23
IM6.18-22 | HIV Counselling Ethics and Adherence — SDL Guide
Learning Objectives
- Counsel patients on prevention of HIV transmission in a non-judgemental manner
- Communicate diagnosis, treatment plan, and follow-up plan to patients with HIV/AIDS
- Communicate with patients on the importance of medication adherence and strategies to improve it
- Demonstrate understanding of ethical and legal issues regarding patient confidentiality and disclosure in HIV/AIDS
- Demonstrate a non-judgemental attitude towards patients with HIV/AIDS and their lifestyles including gender orientation
INSTRUCTIONS
HIV counselling, ethics, and adherence represent the human dimensions of HIV medicine — the clinical skills that transform biomedical competence into effective care. This module addresses the SH-level competencies IM6.18–IM6.22: prevention counselling, diagnostic disclosure, adherence communication, ethical and legal frameworks, and non-judgemental practice. These are skills that require conscious cultivation and are assessed both in OSCEs and in the real clinical encounters of every practitioner.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 197 — Psychosocial Issues and HIV (textbook)
- NACO Operational Guidelines for ART Programmes, 2022 — Counselling and Psychosocial Support (guideline)
- HIV and AIDS (Prevention and Control) Act 2017, India (guideline)
- WHO Consolidated Guidelines on HIV Prevention, Testing, Treatment and Care for Key Populations, 2022 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three moments in one afternoon at an ART centre outpatient clinic. First, a 24-year-old college student named Kavya is sitting across from you, staring at her hands, having just been told her HIV test is positive. She is unmarried, her parents do not know she is here, and her boyfriend is waiting outside. She has not said a word in two minutes. Second, a 38-year-old truck driver named Ramesh has been on ART for 14 months, but his viral load is detectable at 4,800 copies/mL. He shrugs when you ask about missed doses: 'What's the point? I'll die anyway.' Third, a 46-year-old woman named Sumathi, who has been virally suppressed for three years, asks you directly: 'My husband still doesn't know. He has the right to know, doesn't he? But if I tell him, he'll leave me. What should I do?' These three encounters cannot be managed with drug knowledge alone. They require communication skill, ethical clarity, and genuine human respect — the competencies this module builds.
WHY THIS MATTERS
HIV counselling is not a soft skill supplementary to 'real' medicine — it is a clinical competency with measurable outcomes. Effective prevention counselling reduces transmission. Skilled disclosure of a new HIV diagnosis reduces psychological harm and improves engagement with care. Evidence-based adherence communication is the single most modifiable factor in preventing virological failure and drug resistance. And the ethical-legal framework — particularly the HIV and AIDS (Prevention and Control) Act 2017 — defines the clinician's legal obligations and protections. For the NMC SH-level competencies IM6.18–IM6.22, you must be able to demonstrate these skills, not merely describe them. They are assessed in OSCEs, standardised patient encounters, and increasingly in final-year practical examinations. More importantly, they will define the quality of care you provide every time you sit across from a patient with HIV.
RECALL
Before proceeding, activate your prior knowledge of counselling principles from the communication skills curriculum. Effective clinical communication uses open-ended questions ('Tell me how you have been managing the medicines'), active listening (making eye contact, nodding, not interrupting), empathy statements ('That sounds very difficult'), and summarising ('So what I'm hearing is...'). Recall the SPIKES protocol for breaking bad news (Setting, Perception, Invitation, Knowledge, Emotions, Summary) — though designed for oncology, its principles apply directly to HIV diagnosis disclosure. Recall also from community medicine that HIV stigma in India is deeply embedded in social structures — patients face discrimination from family, employers, and sometimes healthcare providers. This stigma is the primary structural barrier to testing, disclosure, and adherence, and understanding it is the context in which every counselling encounter occurs.
Clinical Indication: When and Why Counselling Skills Are Required
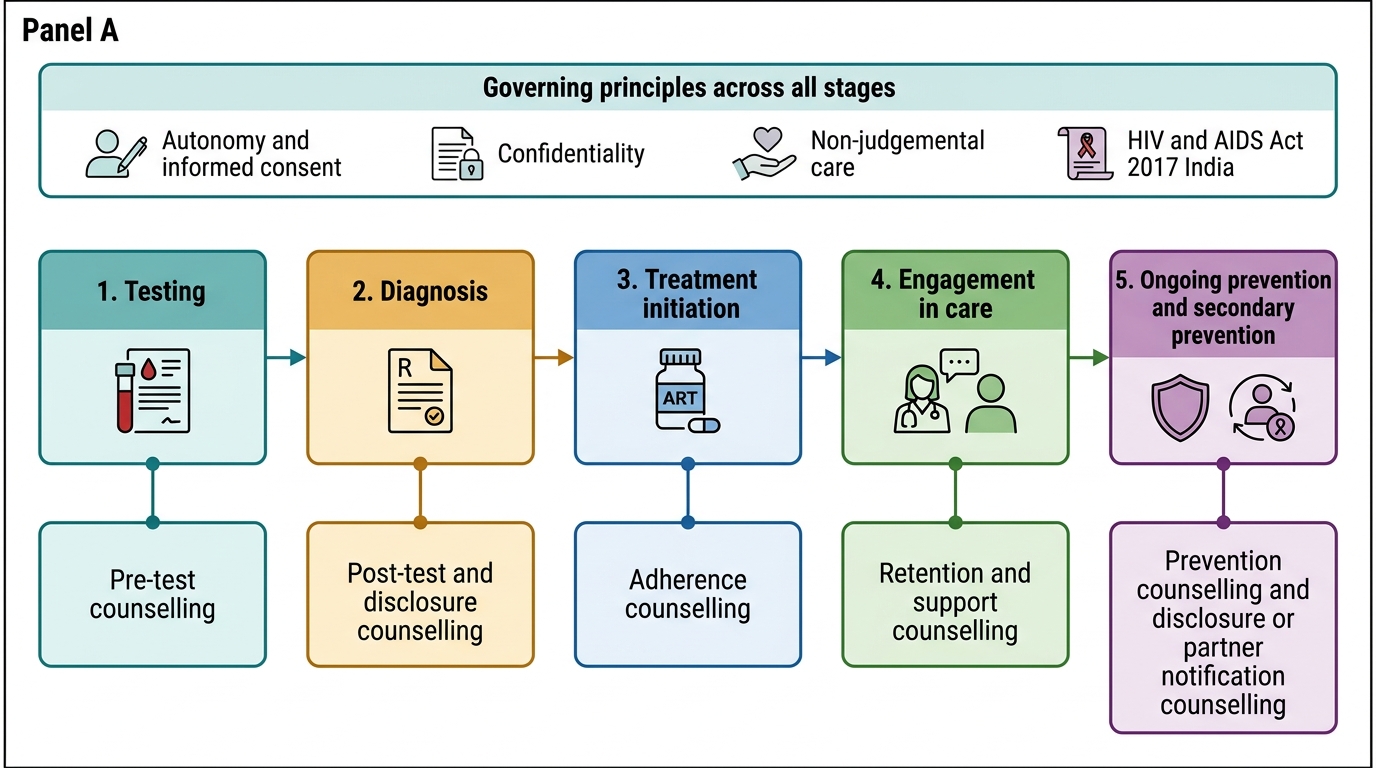
Counselling skills are required at every stage of the HIV care continuum — from the pre-test counselling session before an HIV test is drawn, through disclosure of a positive result, to ongoing adherence support and end-of-life communication. The clinical indications for specific counselling competencies covered in this module are: (1) pre-test counselling — explaining HIV testing, obtaining informed consent, and discussing the implications of a positive or negative result; (2) post-test counselling and diagnosis disclosure — communicating a new HIV diagnosis in a supportive and structured manner; (3) prevention counselling — educating on modes of HIV transmission and strategies to prevent transmission to sexual partners, needle-sharing contacts, and future children; (4) adherence counselling — identifying barriers to ART adherence and applying evidence-based strategies to improve and maintain adherence; (5) disclosure counselling — supporting patients through the decision of whether and how to disclose their HIV status to partners and family members; and (6) ethical consultations — navigating confidentiality, partner notification, duty to warn, and anti-discrimination obligations under Indian law.
The reason all clinicians — not only specialist counsellors — must develop these competencies is that critical counselling moments arise unpredictably in clinical practice. A patient may disclose a positive HIV test in a routine outpatient consultation. A family member may demand an HIV result in the ward. A patient on a surgical list may be found HIV-positive on routine screening. In the Indian district hospital, where there may be no specialist HIV counsellor, the doctor is the counsellor by default. Knowing how to act in these moments — calmly, ethically, and competently — is a core clinical responsibility.
HIV Care Continuum and Counselling Competencies
Governing Principles: Ethics, Law, and Non-Judgement
The governing principles of HIV counselling rest on three foundations: the ethical principles of medical practice (autonomy, beneficence, non-maleficence, justice), the specific legal framework of the HIV and AIDS (Prevention and Control) Act 2017 (India), and the clinical evidence base for non-judgemental practice as a determinant of patient outcomes. Each of these foundations shapes every counselling encounter, and failing to understand any one of them exposes both the patient and the clinician to harm.
Autonomy and informed consent: Every adult patient with HIV has the right to make decisions about their own care, including whether to disclose their status to family, partners, or employers. The clinician's role is to support autonomous decision-making through information and counselling — not to make decisions on the patient's behalf. Informed consent for HIV testing is mandatory: the patient must understand what the test is, what a positive result means, and how confidentiality will be protected, before the test is drawn. Under the HIV Act 2017, HIV testing without informed consent is prohibited.
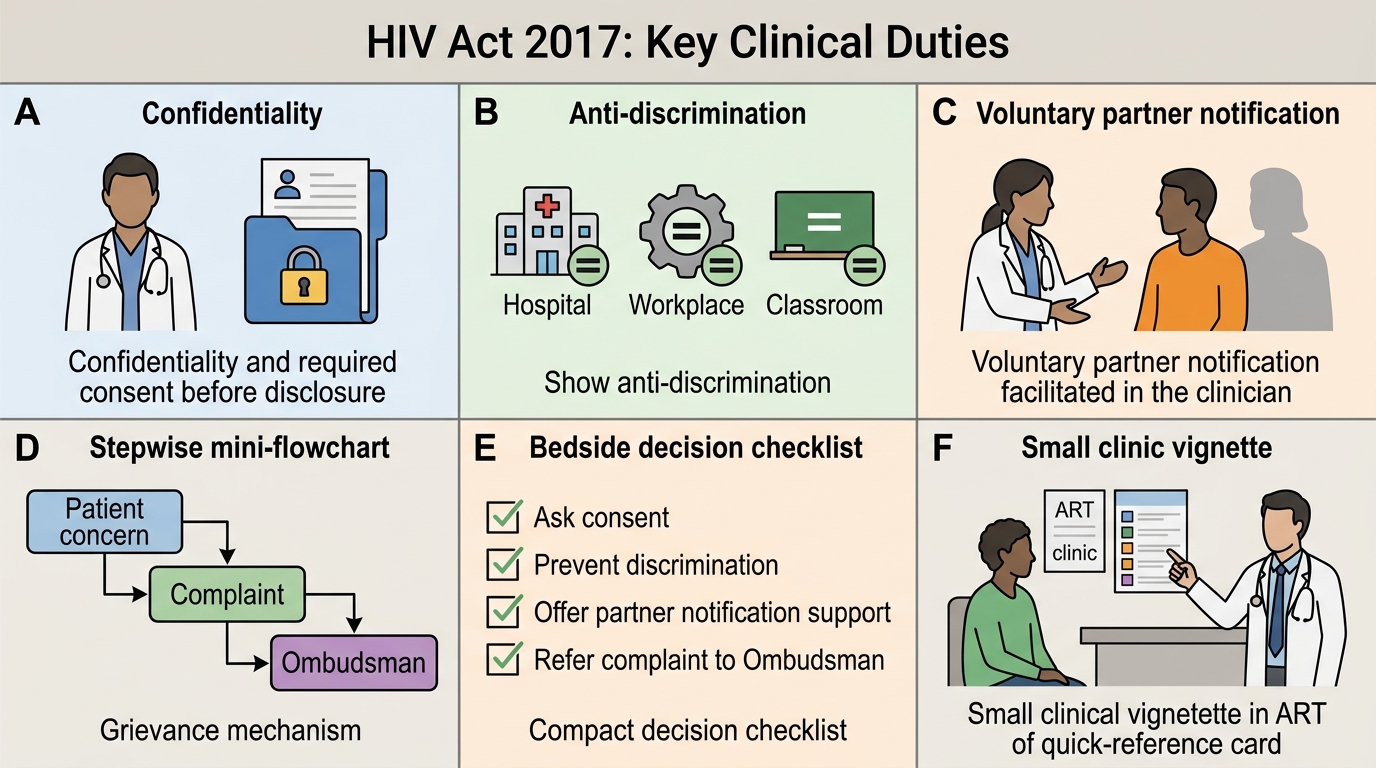
The HIV and AIDS (Prevention and Control) Act 2017 — key provisions:
- Confidentiality: HIV status is legally protected information. No healthcare provider may disclose a patient's HIV status to any third party (including family members, employers, or other healthcare providers) without the patient's written informed consent. Breach of confidentiality is a criminal offence under the Act.
- Anti-discrimination: No person may be denied access to healthcare, employment, education, insurance, or housing on the basis of HIV status. Healthcare providers have a legal duty to provide care to PLHIV without discrimination.
- Partner notification: The Act does not impose a duty to warn identified third parties at risk. However, it does empower the patient to disclose — the clinician should counsel the patient on the importance of partner notification and support voluntary disclosure.
- Guardianship for children: Special provisions for children with HIV, including guardianship rights and protection of minors.
- Ombudsman mechanism: Every state must appoint an HIV/AIDS Ombudsman to receive complaints of discrimination or confidentiality breaches.
Non-judgemental practice as a clinical skill: Evidence consistently shows that patients who perceive judgemental attitudes from healthcare providers are less likely to disclose accurate risk histories, less likely to adhere to treatment, and more likely to disengage from care. The Lancet HIV Commission (2018) identified stigma — including from within the healthcare system — as a central driver of the global HIV epidemic's persistence. Non-judgemental practice is not merely a value preference; it is a clinical intervention with measurable effects on HIV outcomes. It requires: use of person-first language ('person living with HIV' rather than 'HIV patient' or 'AIDS victim'); normalising and neutral language in risk history-taking; explicit assurance of confidentiality at the start of every consultation; and active self-reflection on implicit biases related to sexual orientation, gender identity, sex work, and injecting drug use.
HIV Act 2017: Key Clinical Duties
Prevention Counselling: Communicating HIV Transmission and Prevention
Prevention counselling addresses the knowledge, skills, and motivation that enable patients to prevent HIV transmission to others and to protect themselves from reinfection or co-infection with drug-resistant strains. It is not a one-time lecture but a recurring conversation tailored to the patient's specific risks, relationships, and life context. The content of prevention counselling must be accurate, specific, and non-shaming — generic 'use a condom' advice delivered without contextual engagement is not counselling; it is information delivery. The most important recent development in HIV prevention counselling is the U=U principle (Undetectable = Untransmittable), which transforms the prevention message from one of restriction and risk to one of empowerment and agency: a patient who is virally suppressed on ART is not only protecting their own health but is also effectively non-transmissible to their partner. This evidence-based message, when delivered correctly, has been shown to improve both ART adherence and engagement in care, because it connects the biomedical intervention (taking tablets) to a concrete human benefit (protecting the people the patient loves). Prevention counselling that does not include U=U for virally suppressed patients is incomplete.
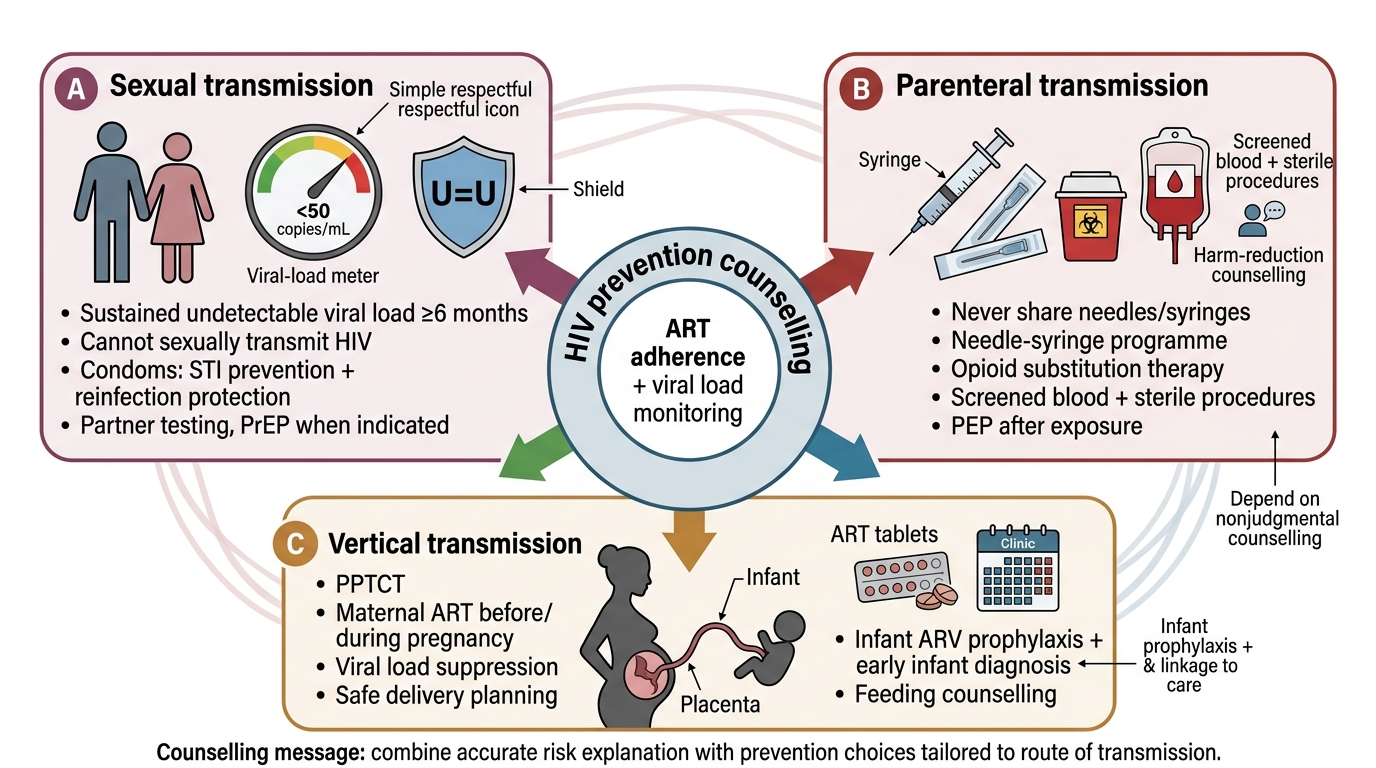
The core content areas of HIV prevention counselling for a patient with HIV are:
1. Modes of transmission and prevention strategies:
- Sexual transmission: Consistent and correct use of condoms (both male and female condoms) during vaginal and anal intercourse. Viral suppression on ART = Undetectable = Untransmittable (U=U) — a patient with a sustained undetectable viral load cannot sexually transmit HIV. This is the most empowering message in modern HIV medicine and must be communicated to all PLHIV on ART: effective treatment is also prevention. Treat concurrent STIs promptly (mucosal ulcers increase HIV transmissibility).
- Blood/parenteral transmission: Never share needles, syringes, or drug-using equipment. Use sterile equipment for all injections. Needle and syringe exchange programmes are available in India for injecting drug users (harm reduction services under NACP).
- Vertical (mother-to-child) transmission: Effective PPTCT (Prevention of Parent-to-Child Transmission) reduces MTCT from ~30% to <1%. Counsel HIV-positive women of reproductive age on: starting or continuing ART throughout pregnancy (TLD throughout pregnancy under NACO 'Treat All' guidelines); planned delivery at a facility with PPTCT capacity; avoidance of breastfeeding when safe alternatives are available (formula feeding in resource-adequate settings); infant prophylaxis with nevirapine syrup for 6 weeks.
2. PEP and PrEP awareness: Counsel all PLHIV on the availability of PEP for their HIV-negative contacts who may have had an accidental exposure — this is relevant for healthcare worker partners and for serodiscordant couples. Offer PrEP counselling to the HIV-negative partner in serodiscordant relationships.
3. Secondary prevention — preventing reinfection and superinfection: A patient with HIV who is virally suppressed can still be re-infected with a drug-resistant HIV strain from a partner (HIV superinfection) — condom use remains important for PLHIV even when their own viral load is undetectable. Concurrent STI acquisition is also a risk even on ART.
4. Harm reduction services under NACP: Opioid Substitution Therapy (OST) with buprenorphine-naloxone for injecting drug users; needle and syringe exchange; targeted interventions for sex workers and MSM under NACP. Counsel patients on how to access these services.
The key technique in prevention counselling is to start with a risk assessment specific to the individual ('What does a typical week look like for you in terms of sexual activity or drug use?') rather than a generic lecture. Then tailor the counselling message to the specific risk domains that apply. Conclude by checking understanding with an open-ended question: 'In your own words, can you tell me what you'll do differently to protect your partner?' This checks comprehension, not just information receipt.
HIV Prevention Counselling Framework
SELF-CHECK
A 30-year-old man with HIV has been on ART for 18 months with consistently undetectable viral load (<50 copies/mL). He asks you whether he still needs to use condoms with his HIV-negative partner. What is the MOST accurate and evidence-based response?
A. 'Yes, you must always use condoms — HIV can still be transmitted even with treatment'
B. 'According to the U=U evidence, a sustained undetectable viral load means you cannot sexually transmit HIV, but condom use remains advisable for STI prevention and reinfection protection'
C. 'No, you don't need condoms at all — treatment cures HIV transmission completely'
D. 'I'm not sure — you should ask a specialist about this'
Reveal Answer
Answer: B. 'According to the U=U evidence, a sustained undetectable viral load means you cannot sexually transmit HIV, but condom use remains advisable for STI prevention and reinfection protection'
The Undetectable = Untransmittable (U=U) principle is well-established: a person with HIV who has maintained an undetectable viral load on ART for ≥6 months cannot sexually transmit HIV. This is the most empowering and accurate message to give. However, condoms remain advisable for two additional reasons: (1) protection against other STIs (herpes, gonorrhoea, syphilis, HPV) which are not prevented by ART; (2) protection against HIV superinfection with a drug-resistant strain. Option A is factually incorrect (overstates transmission risk when virally suppressed). Option C is factually incorrect (does not address STI risk). Option D is inappropriate — this is a well-established evidence-based finding that the attending physician should be able to communicate.