Page 17 of 23
IM6.18-22 | HIV Counselling Ethics and Adherence — SDL Guide (Part 2)
Communicating Diagnosis, Treatment Plan, and Follow-Up
Communicating a new HIV diagnosis is one of the most challenging communication encounters in clinical medicine. It must be done in a structured, sensitive, and accurate way — the clinician's choice of words, tone, and framing in this first conversation will significantly shape the patient's initial psychological response, their willingness to engage with care, and their early treatment adherence. The consequences of a poorly handled disclosure — patient leaving the clinic without follow-up, refusal to share results with a partner, or acute psychological crisis — are measurable in health outcomes. Research on HIV diagnosis disclosure consistently shows that patients who receive their diagnosis from a clinician who uses structured, empathic communication are more likely to return for follow-up, engage with ART initiation, and make disclosure decisions about their partners. Conversely, diagnosis delivered in a rushed, dismissive, or judgemental manner is a predictor of loss to follow-up. The diagnosis encounter is not merely an information transfer; it is the foundation of the therapeutic relationship that will support ART adherence for years or decades. Every minute invested in this encounter is repaid in long-term treatment engagement.
A structured framework for HIV diagnosis disclosure follows the SPIKES model adapted for HIV:
- S — Setting: Ensure privacy (closed room, no family present unless the patient specifically requests it); ensure the patient has time (do not disclose at the end of a busy clinic); have a counsellor or support person present if available. Switch off or silence your phone.
- P — Perception: Assess the patient's current awareness. 'Before I share your result, can I ask — what were you expecting or hoping the test might show?' This opens a dialogue, identifies prior fears or denials, and prepares the patient for the information.
- I — Invitation: Ask explicitly: 'Would it be alright if I share your test result with you now?' This gives the patient a moment of agency before the disclosure.
- K — Knowledge (the disclosure itself): Use clear, non-technical language. Avoid medical jargon. 'Your HIV test has come back positive. This means the HIV virus is present in your blood.' Pause. Allow silence. Do not rush to fill the silence with information. Watch the patient's reaction.
- E — Emotions: After a brief silence, acknowledge the emotion: 'I can see this is very difficult to hear. Take your time.' Listen actively. Do not immediately launch into the treatment plan — wait until the patient signals readiness to hear more ('What do I do now?', 'Is there a treatment?').
- S — Summary: Once the patient is ready, provide a clear, simple summary of next steps: 'The good news is that HIV is now a treatable condition. With the right medicines — which are free through the government programme — people with HIV live long, healthy lives. The next step is some blood tests to check your immune system, and then we'll talk about starting treatment.'
Communicating the treatment plan: The treatment plan communication covers: the name and purpose of ART (NACO TLD), the need for daily adherence, common initial side effects, what to do if a dose is missed, and the follow-up schedule (CD4, viral load at 6 months). Use teach-back ('Can you tell me in your own words what the first tablet is for?') to verify understanding. Provide written information where available. Arrange a follow-up appointment before the patient leaves.
Communicating the follow-up plan: A clear follow-up plan reduces loss-to-follow-up — one of the most common causes of treatment failure. The plan should include: date of next appointment; what tests will be done (CD4, viral load at 6 months); what to do if side effects are experienced before the appointment; and the clinic contact number.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
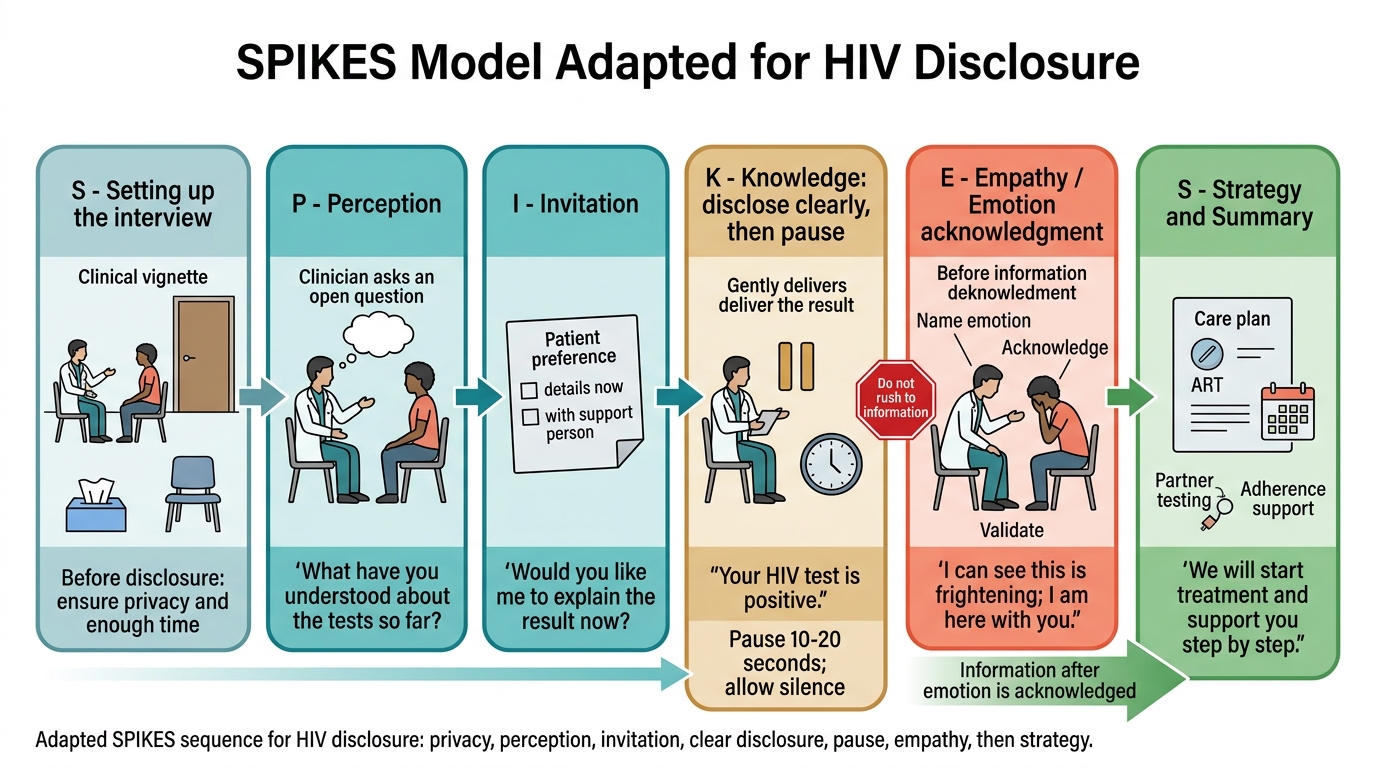
SPIKES Model for HIV Disclosure
Adherence Counselling: Evidence and Technique
Medication adherence is the single most important modifiable predictor of HIV treatment outcomes. Viral suppression requires >95% adherence — defined as missing no more than 1 dose per week on a once-daily regimen. At adherence below 90%, viral replication occurs with sub-therapeutic drug concentrations present, which is the ideal condition for selection of drug-resistant mutants. HIV reverse transcriptase is inherently error-prone (one replication error per cycle) and produces 10⁹–10¹⁰ virions daily; even short periods of inadequate drug coverage allow resistance mutations to accumulate and become dominant in the viral population. Preventing virological failure through adherence counselling is therefore a pharmacological intervention, not merely a communication courtesy.
The evidence base for adherence interventions in HIV is extensive. Key findings from systematic reviews and NACO programme evaluations: counselling at initiation and each follow-up (discussing barriers, problem-solving) doubles adherence compared with one-time education; fixed-dose combinations (like TLD — a single tablet once daily) improve adherence compared with multiple separate tablets; mobile phone reminders improve adherence by 12–15% in RCTs in low- and middle-income countries; peer support groups and treatment supporters (a trusted person who knows the diagnosis and can support daily dosing) are endorsed by NACO; directly observed therapy (DOT) is reserved for patients with severe psychiatric illness or extreme social disorganisation.
The structured adherence counselling encounter at each ART centre visit follows a five-step process:
Step 1 — Non-judgemental adherence assessment: Use normalising language and specific recall: 'Taking tablets every day can be challenging — how have you been managing? Thinking back to the last week, were there any days when you missed a dose? Which ones?' The 3-day recall (last 3 days) and 30-day recall (how many doses missed this month) are the two evidence-based self-report methods endorsed by NACO. Avoid 'compliance' language (which implies blame) — use 'adherence' or 'taking your medicines.'
Step 2 — Identify the barrier: The specific barrier to adherence determines the solution. Common barriers and their targeted responses:
- Forgetfulness: Set a daily phone alarm; link tablet-taking to a fixed daily activity (morning tea, brushing teeth); use a pill box.
- Side effects: Identify the specific side effect; counsel on expected transient vs serious side effects (e.g., mild nausea in first 2 weeks vs tenofovir-related cramp); adjust timing if appropriate (take with or without food based on the drug); do not stop ART without medical advice.
- Stigma and concealment: Many patients cannot take their tablet in front of family or colleagues who do not know their status; problem-solve with the patient: taking the tablet in private, storing in plain unmarked container, linking to another tablet (e.g., a vitamin).
- Pill fatigue: Acknowledge and validate; highlight the single-tablet convenience of TLD; review total pill burden (co-trimoxazole, IPT, ART).
- Hopelessness or depression: Screen for depression (PHQ-9 in Indian primary care settings); refer to mental health support; address the belief that 'there is no point' — explicitly share that undetectable viral load means normal life expectancy and inability to transmit HIV (U=U).
- Travel and work schedule disruption: Counsel on carrying medicines safely while travelling; ensure sufficient supply for travel periods; plan ahead for shift work.
Step 3 — Problem-solve collaboratively: Do not instruct — negotiate. 'What do you think would work best for you?' The patient who generates their own adherence strategy is more likely to implement it than one who receives instructions.
Step 4 — Treatment supporter involvement: With patient consent, involve a trusted person (spouse, sibling, friend) who can support daily dosing — the NACO 'treatment supporter' model has good evidence from Indian ART programme data.
Step 5 — Follow up on the adherence plan: At the next visit, review the strategy agreed: 'How did the phone alarm work? Were there any days when it was still difficult?' Reinforce success, problem-solve new barriers.
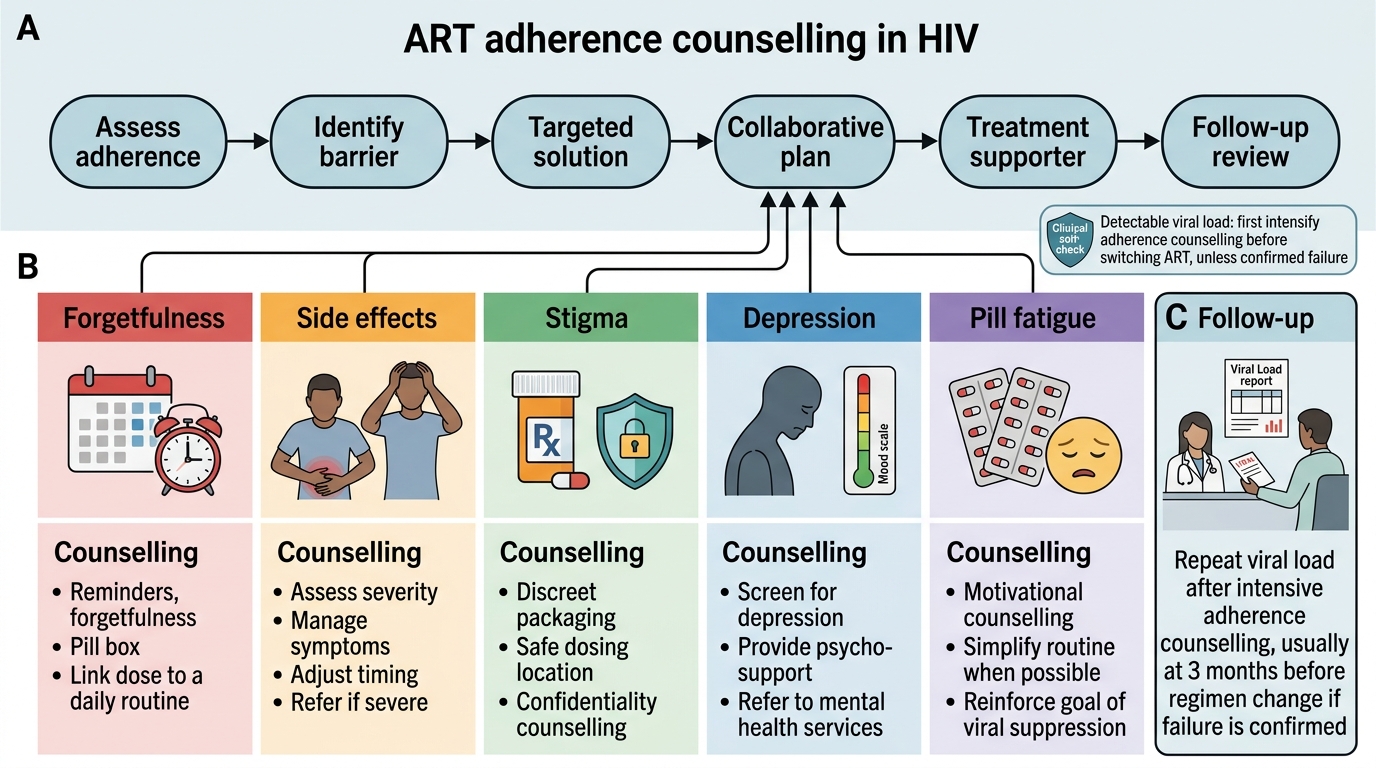
ART Adherence Counselling Flowchart in HIV
SELF-CHECK
A 45-year-old man with HIV has been on ART for 2 years. At his follow-up visit, his viral load is detectable at 3,200 copies/mL. When you ask about missed doses, he says: 'I take it most days — maybe I miss one or two a week because of shift work.' Which is the MOST evidence-based next step in managing his adherence?
A. Immediately switch to second-line ART as this indicates virological failure
B. Prescribe directly observed therapy (DOT) for all ART doses
C. Apply intensive adherence counselling: use 3-day recall, identify the specific shift-work barrier, problem-solve with patient, and involve a treatment supporter — reassess viral load in 3 months before considering regimen change
D. Simply reinforce that missing doses causes resistance and instruct strict compliance
Reveal Answer
Answer: C. Apply intensive adherence counselling: use 3-day recall, identify the specific shift-work barrier, problem-solve with patient, and involve a treatment supporter — reassess viral load in 3 months before considering regimen change
Detectable viral load after ≥6 months on ART is virological failure if confirmed on two measurements — but the first step when a detectable viral load is found is ALWAYS intensive adherence counselling and a repeat viral load in 3 months. Shifting to second-line ART without confirming true adherence-supported virological failure risks unnecessarily exposing the patient to second-line drugs with more side effects and higher cost. DOT is reserved for severe psychiatric illness or social disorganisation — not the appropriate first step for shift-work non-adherence. Simply instructing 'don't miss doses' without addressing the specific barrier (shift work schedule) is ineffective. The correct approach is: specific adherence assessment (3-day recall), identify the shift-work barrier, problem-solve together (pre-dosing before shift, phone alarm, colleague as supporter), then repeat viral load in 3 months. If still detectable, then consider resistance testing and second-line switch.
Self-Assessment: Ethical Scenarios and Communication Practice
The following scenarios consolidate your understanding of the ethical-legal framework and communication skills covered in this module. Each scenario presents a realistic ethical dilemma drawn from the Indian clinical context. Apply the HIV Act 2017 framework and the counselling principles before reading the analysis. Note that these scenarios do not have simple right answers — they are designed to reveal the tensions between competing ethical obligations (autonomy vs harm prevention, confidentiality vs partner protection) and to train you to reason through them rather than apply a rigid rule. The ability to navigate these tensions thoughtfully — weighing the law, ethics, and clinical context — is what the SH-level IM6.21 competency requires: 'demonstrate understanding of ethical and legal issues,' which means more than reciting the provisions of the Act.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
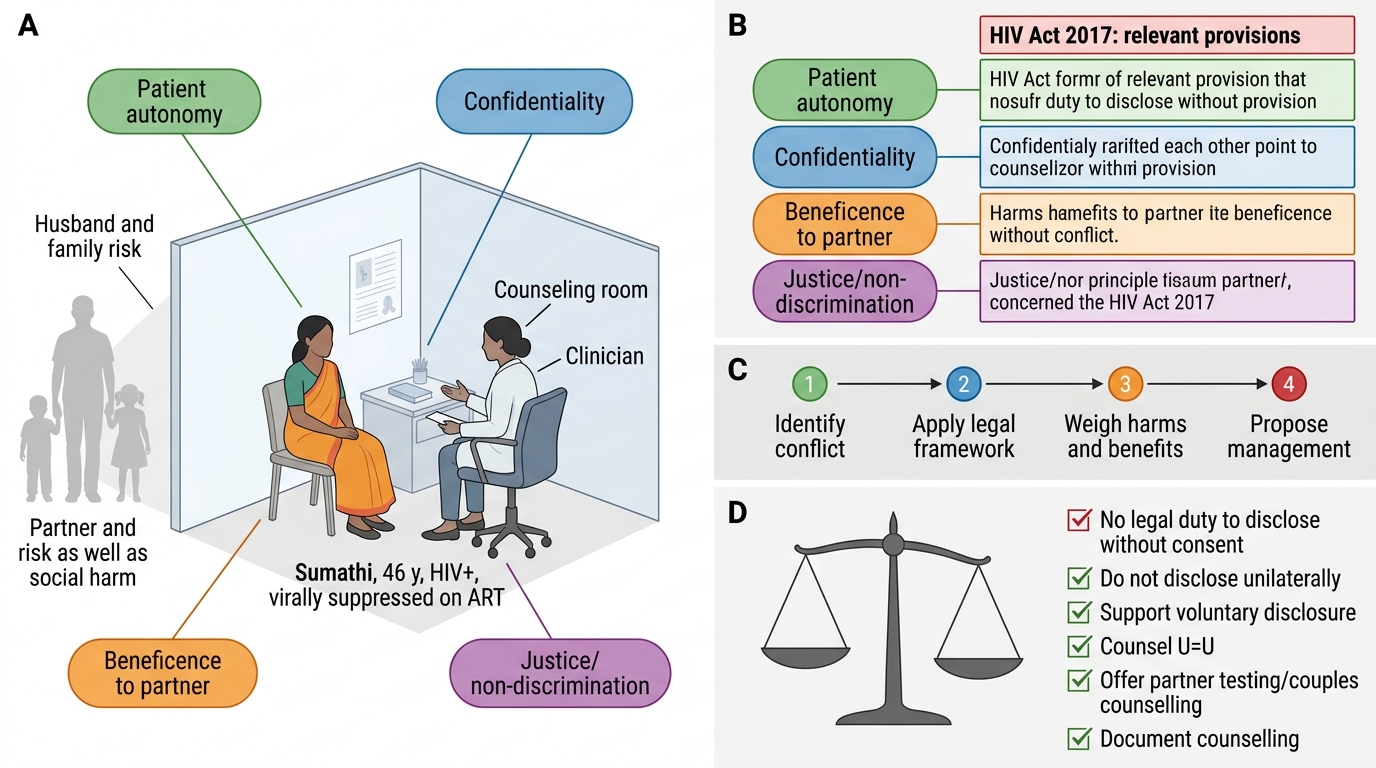
Ethical Reasoning in HIV Confidentiality
Scenario A — Confidentiality and partner risk: Sumathi, 46 years old, has been virally suppressed on ART for three years. Her husband does not know her HIV status. She tells you she will not disclose to him because he will leave her and take their children. You know her husband is not on ART and has not been tested. Do you have a legal duty to disclose her HIV status to her husband without her consent?
Analysis: Under the HIV Act 2017, you do NOT have a legal duty to disclose without consent — in fact, disclosure without written consent is prohibited and constitutes a criminal offence. Your clinical obligation is to: (1) provide ongoing counselling supporting voluntary disclosure — explain the benefit to her husband (early diagnosis, treatment, prevention of transmission); (2) counsel on U=U — if she remains virally suppressed, her risk of transmitting to her husband is effectively zero, which changes the risk calculus; (3) offer to facilitate partner testing or couples counselling; (4) document your counselling interventions in the medical record. You cannot and must not disclose without her consent. The long-term goal is to enable her to make the voluntary decision to disclose — or to maintain viral suppression such that transmission risk is negligible.
Scenario B — Disclosure and family pressure: A 28-year-old man newly diagnosed with HIV is in the ward. His mother demands to know 'what is wrong with him.' She is his primary caregiver. He has not given consent for disclosure of his HIV status. What do you tell her?
Analysis: You must protect confidentiality absolutely. Tell the mother: 'Your son has a medical condition that requires treatment — he is in the best hands and is receiving appropriate care. For details of his diagnosis, he is the right person to discuss this with you — it is his information to share.' You must not disclose his HIV status, even to his mother, without his explicit written consent. Privately, counsel the patient: acknowledge the difficulty, explain that his mother's support could help his recovery, explore whether he wishes to disclose and offer support in doing so, but make clear the decision is entirely his.
Scenario C — Non-judgement and gender identity: A 22-year-old transgender woman presents to the ART centre for HIV testing. The registration staff are visibly uncomfortable and ask her to wait in a separate area. The doctor asks her to 'just answer the medical questions' and avoids eye contact throughout the encounter. What are the clinical and legal problems with this encounter?
Analysis: The behaviour of the registration staff (segregation) and the doctor (disengagement, avoidance) constitutes stigmatising behaviour and possible discrimination, violating: (1) the HIV Act 2017 anti-discrimination provisions; (2) the NMC professional conduct standards; (3) the clinical principle that non-judgemental care is a determinant of patient outcomes (patients who experience stigma in healthcare disengage from care). The correct approach: transgender patients should be addressed by their preferred name and pronouns, receive care without discrimination or segregation, and be counselled in the same private, respectful manner as any other patient. The clinician's own discomfort is their professional responsibility to manage, not the patient's.
CLINICAL PEARL
Three counselling pearls that clinicians routinely underuse. First: U=U changes the prevention conversation — instead of 'use a condom always,' the message for a virally suppressed patient on ART is 'you are protecting your partner by staying on treatment; condoms also protect against STIs.' This shifts the framing from restriction to empowerment and dramatically improves treatment motivation. Second: confidentiality is absolute under the HIV Act 2017 — even telling a patient's spouse, parent, or employer without written consent is a criminal offence, not merely an ethical breach; document every counselling session where disclosure was discussed. Third: the most effective adherence intervention is identifying the specific barrier — 'take your medicines' repeated louder is not adherence counselling; the shift-worker who misses doses during night shifts needs a different solution than the patient who misses doses from depression, who needs a different solution than the patient concealing tablets from family.