Page 10 of 23
IM6.9-12 | HIV Diagnostic Testing — SDL Guide (Part 2)
Imaging in HIV: CXR, CT Chest, CT/MRI Brain
Imaging plays a critical role in the diagnosis and severity assessment of HIV-related opportunistic infections. Each OI has a characteristic imaging signature that, combined with clinical context (CD4 count, symptom duration, examination findings), narrows the differential before the specific laboratory results are available. The clinician managing HIV patients must be able to request the right imaging study, interpret the key findings, and understand the clinical implications of each pattern. Requesting the right imaging at the right time is itself a diagnostic skill: a CT brain must be performed before LP if there is papilloedema or focal neurological deficit (to exclude mass lesion and herniation risk); an HRCT chest is indicated when plain CXR is non-diagnostic in a hypoxic HIV patient with suspected PCP; MRI brain provides superior resolution for brainstem and posterior fossa lesions where CT may miss small ring-enhancing lesions in toxoplasmosis. Conversely, ordering a CT brain for every headache in an HIV patient when a clinical examination and LP are more informative reflects over-investigation. The framework below organises imaging by modality, with the key OI patterns for each.
Chest X-ray (CXR) in HIV: The CXR is the first-line imaging study for any HIV patient with respiratory symptoms. Interpretation requires correlating the pattern of opacification with the clinical and CD4 context:
- Bilateral perihilar interstitial ('ground-glass') infiltrates with a predominantly central and perihilar distribution, sparing the peripheral lung: PCP — the classic pattern. In early PCP, the CXR may be entirely normal despite significant hypoxia (hence, a normal CXR does not exclude PCP in a hypoxic HIV patient).
- Lobar or segmental consolidation (airspace opacification in a lung segment or lobe): bacterial pneumonia — typically acute onset, productive cough, fever response; or primary pulmonary TB in early HIV.
- Upper lobe cavitation ± apical infiltrates: Pulmonary TB at higher CD4 counts (>200). As CD4 falls, TB presentations become atypical — lower-lobe involvement, miliary pattern, hilar lymphadenopathy, no cavitation ('non-cavitatory TB' at low CD4).
- Miliary pattern (innumerable tiny nodules <2 mm distributed diffusely throughout both lung fields, like millet seeds): miliary TB — occurs at low CD4; also possible in disseminated fungal infections (histoplasmosis).
- Bilateral nodular shadows + pleural effusion: Pulmonary Kaposi sarcoma — the combination of bilateral nodular/perihilar infiltrates with pleural effusion in a patient with mucocutaneous KS is characteristic; also KS can produce a 'butterfly' perihilar distribution similar to PCP.
- Normal CXR with profound hypoxia: PCP in early stages; also consider PCP even with a normal CXR when the clinical syndrome and LDH are consistent.
CT Chest: Indicated when CXR is non-diagnostic or when the pattern needs characterisation. In PCP: HRCT shows bilateral ground-glass opacification with a geographic distribution (areas of normal lung adjacent to affected areas), sometimes with a 'crazy-paving' pattern (ground-glass superimposed on interlobular septal thickening). Pneumatoceles (thin-walled air cysts) may develop and carry a risk of pneumothorax. CT chest is also used for: lymph node sampling (mediastinal/hilar lymphadenopathy in TB or lymphoma), characterising pleural effusions (empyema, KS-related), and evaluating nodular lesions for bronchoscopic or CT-guided biopsy.
CT Brain: The first-line imaging for HIV patients with neurological symptoms. Non-contrast CT is adequate for urgent exclusion of raised ICP before LP. Contrast-enhanced CT is preferred for lesion characterisation:
- Multiple ring-enhancing lesions in the basal ganglia and corticomedullary junction with surrounding oedema and mass effect: cerebral toxoplasmosis — the most common pattern; multiple lesions are the rule (though occasionally single); predilection for basal ganglia distinguishes it from PCNSL.
- Single large ring-enhancing lesion, often in white matter or basal ganglia, with diffuse irregular rim and surrounding oedema: primary CNS lymphoma (PCNSL) — typically a single lesion (though multiple can occur); the periventricular white matter is a common site.
- Normal CT with raised ICP (elevated opening pressure on LP): Cryptococcal meningitis — CT is often normal or shows minimal cerebral oedema; the CT is used to exclude mass lesion before LP, not to diagnose cryptococcal disease.
- White matter hypodensity (bilateral confluent white matter low density on CT): HIV leucoencephalopathy or progressive multifocal leucoencephalopathy (PML) due to JC virus — typically subcortical white matter.
MRI Brain: Provides superior anatomical detail and is the preferred modality when CT findings are inconclusive. MRI sequences and their OI applications:
- T1 post-gadolinium: Ring-enhancing lesions in toxoplasmosis and PCNSL — MRI is more sensitive than CT for small lesions, brainstem lesions, and posterior fossa lesions. The 'target sign' (three concentric rings on MRI — central enhancement, surrounding oedema, and outer enhancement ring) is more specific for toxoplasmosis than PCNSL.
- T2/FLAIR: White matter hyperintensities in PML (asymmetric, non-enhancing, U-fibres spared early); HIV encephalopathy (diffuse symmetric white matter changes); CMV ventriculoencephalitis (periventricular T2 hyperintensity ± subependymal enhancement).
- DWI (diffusion-weighted imaging): PML lesions show restricted diffusion at the leading edge; PCNSL typically shows homogeneous diffusion restriction in the enhancing component.
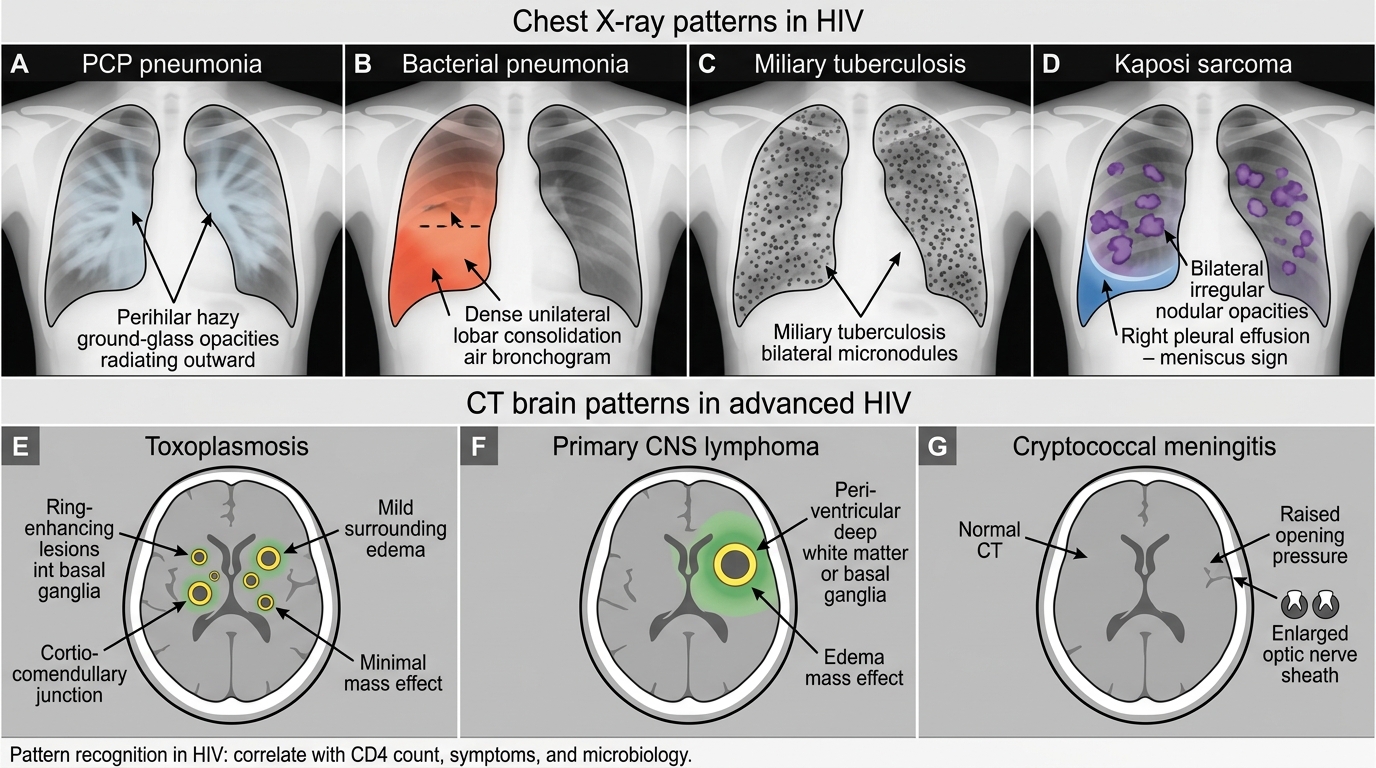
Imaging Patterns in Advanced HIV
SELF-CHECK
A 39-year-old HIV-positive man with CD4 count 58 cells/µL presents with 3 weeks of progressive headache and one episode of vomiting. SpO₂ is 98%. CT brain shows no mass lesion, no midline shift. LP is performed: opening pressure 36 cm H₂O; CSF has 12 lymphocytes, protein 68 mg/dL, glucose 48 mg/dL (blood glucose 90 mg/dL). India ink stain of CSF is positive. What does the SERUM CrAg test add in this patient's management going forward?
A. It confirms the CSF India ink result and no further action is needed
B. A positive serum CrAg indicates disseminated (non-CNS) cryptococcosis requiring additional antifungal agents
C. A positive serum CrAg at baseline, once CNS disease is treated, guides the NACO pre-emptive fluconazole strategy for future patients screened at CD4 <100
D. Serum CrAg has no role once CSF India ink is positive and treatment has started
Reveal Answer
Answer: C. A positive serum CrAg at baseline, once CNS disease is treated, guides the NACO pre-emptive fluconazole strategy for future patients screened at CD4 <100
In this patient, the India ink stain has already confirmed cryptococcal meningitis and treatment should start immediately. The clinical relevance of serum CrAg in future management is its role in the NACO pre-emptive treatment programme: at CD4 <100, serum CrAg screening can detect cryptococcal antigenemia before CNS disease develops — a positive serum CrAg without meningitis triggers pre-emptive fluconazole therapy to prevent progression to meningitis. This patient has already progressed to meningitis, so the serum CrAg confirms systemic dissemination but does not change the immediate antifungal plan (Amphotericin B + flucytosine). However, understanding the serum CrAg screening programme is directly tested in IM6.9 competency.
Pulse Oximetry and ABG in HIV Respiratory Presentations
Pulse oximetry and arterial blood gas (ABG) analysis are critical tools for assessing the severity of respiratory compromise in HIV patients, particularly in the context of suspected PCP. Their role goes beyond simple oxygen saturation measurement — they determine the threshold for adjunctive corticosteroid therapy in PCP and guide oxygen supplementation decisions. Every HIV patient presenting with respiratory symptoms should have a pulse oximetry reading recorded at rest and on exertion (the exertion desaturation test).
Provided image
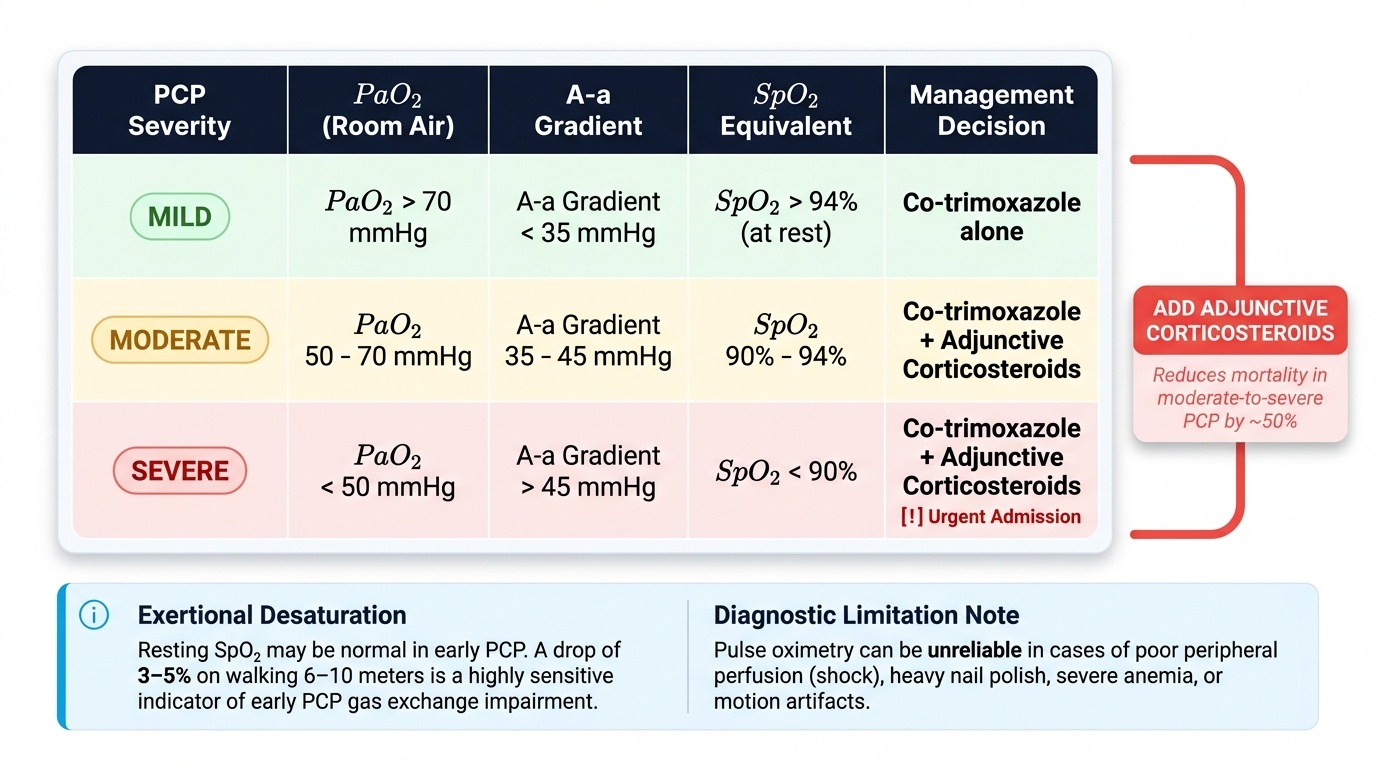
Pulse oximetry: SpO₂ at rest and on exertion. In PCP, resting SpO₂ may be near-normal (92–95%) in mild disease but falls markedly on minimal exertion — a SpO₂ drop of >3–5% on walking 6–10 metres is a sensitive early indicator of PCP-related gas exchange impairment. This exertional desaturation can be elicited at the bedside with a 6-minute walk test or simply by asking the patient to walk to the toilet while monitoring SpO₂. A resting SpO₂ <90% indicates severe PCP and mandates urgent intervention. Limitations of pulse oximetry: unreliable in motion, poor peripheral perfusion (septic shock), nail polish, or severe anaemia (falsely elevated SpO₂ in methaemoglobinaemia).
Arterial blood gas (ABG): The ABG provides three critical parameters for PCP severity assessment:
- PaO₂ on room air: The primary determinant of PCP severity. PaO₂ <70 mmHg on room air (or SpO₂ <90% equivalently) defines moderate-to-severe PCP, which mandates adjunctive corticosteroids. Corticosteroids reduce the mortality from moderate-to-severe PCP by approximately 50% — the most important adjunctive treatment decision in HIV respiratory medicine.
- Alveolar-arterial (A-a) gradient: Calculated as A-a gradient = (FiO₂ × 713 − PaCO₂/0.8) − PaO₂. A-a gradient >35 mmHg on room air also defines moderate-to-severe PCP requiring corticosteroids. The A-a gradient reflects the degree of ventilation-perfusion mismatch in PCP (the alveoli fill with frothy exudate but are still perfused, creating shunting). It is a more sensitive indicator of severity than PaO₂ alone in patients who are already on supplemental oxygen.
- pH and PaCO₂: In mild-to-moderate PCP, respiratory alkalosis (low PaCO₂) is common from tachypnoea-driven hyperventilation. Respiratory acidosis (rising PaCO₂) in PCP indicates impending respiratory failure and may signal the need for non-invasive ventilation or ICU transfer.
Indications for ABG in HIV patients:
1. Any HIV patient with respiratory symptoms and SpO₂ <94% on room air
2. Suspected PCP — to assess severity and determine if corticosteroids are indicated
3. Monitoring response to PCP treatment (improvement in PaO₂ and A-a gradient expected by day 3–5 on TMP-SMX)
4. Any HIV patient with altered consciousness and respiratory symptoms (excludes hypercapnic respiratory failure)
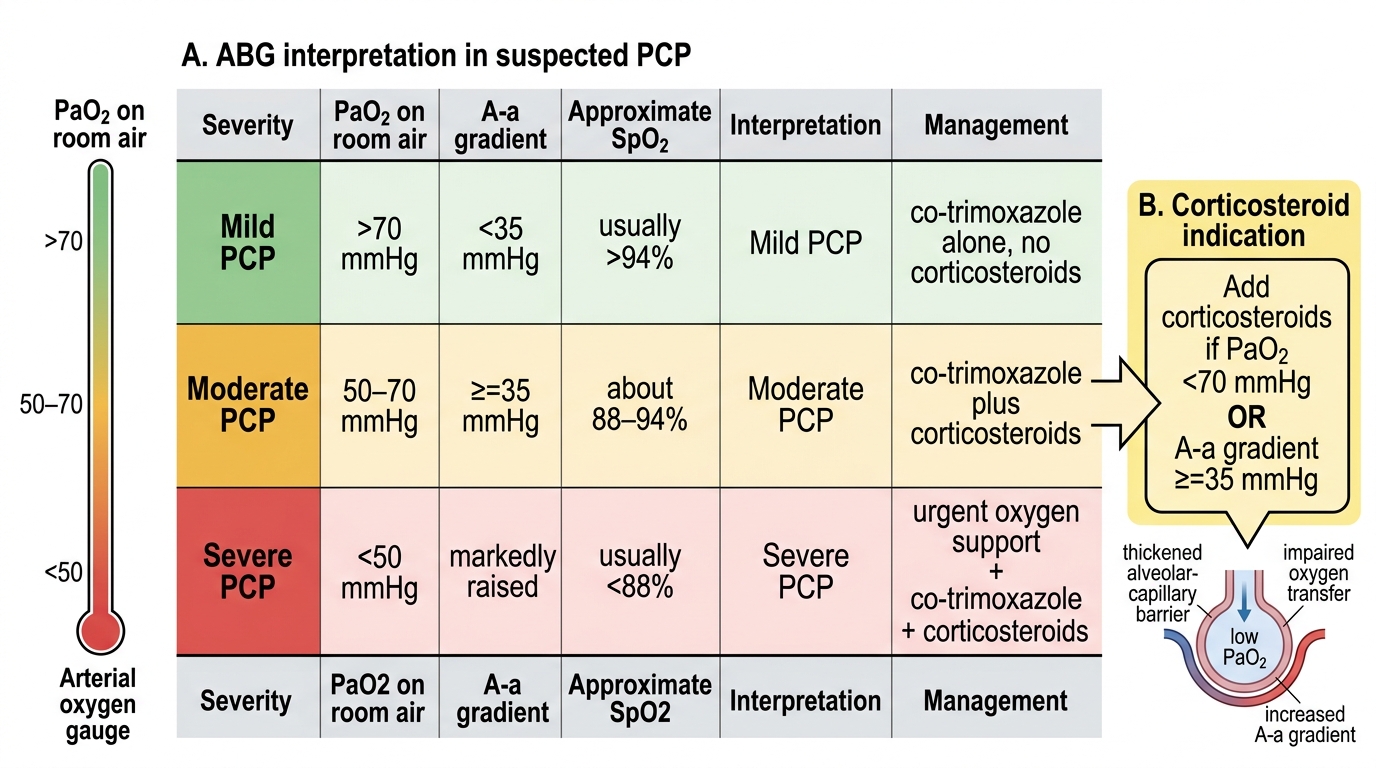
ABG Severity Guide for PCP in HIV
SELF-CHECK
A 31-year-old HIV-positive man with CD4 count 82 cells/µL presents with 2 weeks of insidious dry cough and exertional dyspnoea. His resting SpO₂ on room air is 91%. CXR shows bilateral perihilar ground-glass infiltrates. LDH is 745 IU/L. An ABG on room air shows: pH 7.46, PaO₂ 62 mmHg, PaCO₂ 32 mmHg. Which management decision is DIRECTLY determined by the ABG result in this patient?
A. Whether to start co-trimoxazole or IV pentamidine
B. Whether to add adjunctive corticosteroids (prednisolone) to co-trimoxazole
C. Whether to perform bronchoalveolar lavage before starting treatment
D. Whether to start antiretroviral therapy immediately
Reveal Answer
Answer: B. Whether to add adjunctive corticosteroids (prednisolone) to co-trimoxazole
The ABG shows PaO₂ 62 mmHg on room air, which is <70 mmHg — this meets the threshold for moderate-to-severe PCP that mandates adjunctive corticosteroids (prednisolone 40 mg BD for 5 days, tapering over 21 days). The corticosteroid decision is directly determined by PaO₂ <70 mmHg (or A-a gradient >35 mmHg) on room air. The choice between co-trimoxazole and IV pentamidine is based on clinical severity and intolerance, not the ABG alone. BAL can be performed but treatment should not be delayed awaiting biopsy confirmation in a hypoxic patient. ART timing in OIs follows specific guidelines but is not determined by the ABG value.
Applied Practice: Selecting Investigations in Resource-Limited Settings
The practical application of HIV diagnostics in India demands a tiered approach that matches investigation choice to the level of available resources, the clinical urgency, and the impact of the result on immediate management. A district hospital, a secondary care HIV clinic, and a tertiary ART referral centre each have a different investigation menu — the skilled clinician adapts the diagnostic strategy to the setting without compromising the quality of the clinical decision. This section synthesises the principles covered in preceding blocks into a practical decision-making framework for the three most common high-urgency HIV presentations in India.
Provided image
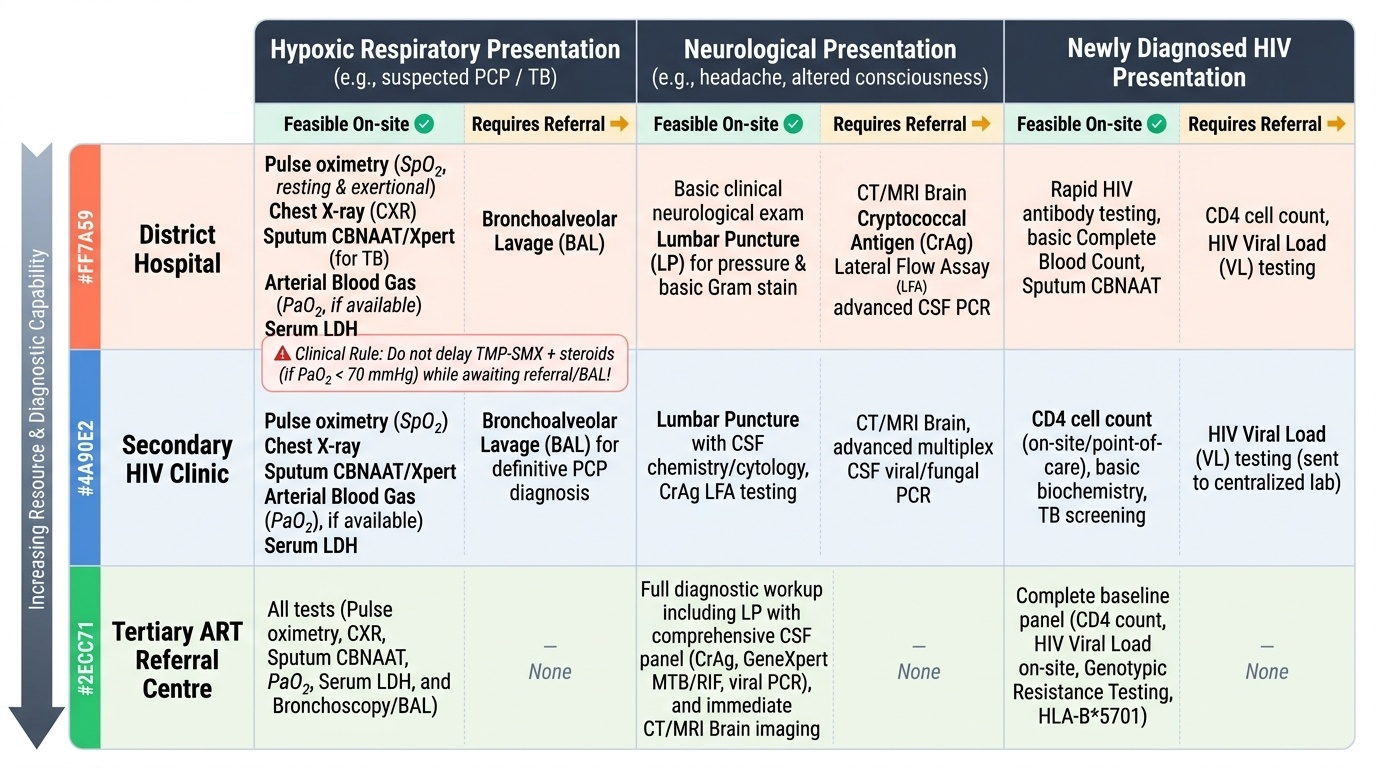
Applied framework 1 — The hypoxic HIV patient in a district hospital: When a patient presents with SpO₂ <94%, bilateral infiltrates on CXR, and elevated LDH in a setting where BAL is unavailable, the clinical diagnosis of PCP is made empirically. The investigations that are feasible and decision-changing are: (1) pulse oximetry — resting and exertional — to establish severity; (2) ABG if available — to determine whether corticosteroids are indicated (PaO₂ <70 mmHg threshold); (3) sputum CBNAAT/Xpert to exclude TB (critical in India, where TB-PCP co-infection occurs and both can produce bilateral infiltrates); (4) serum LDH as a PCP severity surrogate. Do not delay TMP-SMX while awaiting BAL — start treatment, add corticosteroids if ABG indicates severity, refer for BAL if no improvement at 48–72 hours.
Applied framework 2 — The HIV patient with neurological symptoms: Any HIV patient with headache, fever, altered consciousness, or focal neurological deficit requires urgent evaluation. The minimum diagnostic set is: (1) CT brain (urgent, before LP) — to exclude mass lesion and raised ICP from a space-occupying lesion; (2) if CT shows no mass lesion, perform LP with opening pressure; (3) send CSF for India ink stain and CrAg LFA simultaneously (do not wait for India ink result before ordering CrAg); (4) CSF routine analysis (cell count, protein, glucose) and bacterial culture; (5) if focal lesion is seen on CT (ring-enhancing, basal ganglia), start empirical toxoplasmosis therapy and arrange MRI brain for characterisation. The practical rule is: LP first (after CT), CrAg and India ink simultaneously, empirical treatment based on the most likely diagnosis by CD4 and clinical pattern.
Applied framework 3 — Routine workup of newly diagnosed PLHIV: At the NACO ART centre, all newly diagnosed PLHIV should have the following baseline investigations: CD4 count; HIV viral load; full blood count (anaemia, leucopaenia); renal function (creatinine, eGFR — TDF contraindicated if eGFR <50 mL/min/1.73m²); liver function tests (hepatitis B co-infection, transaminase elevation with some ARVs); hepatitis B surface antigen (HBsAg) and hepatitis C antibody; chest X-ray (TB screening); sputum CBNAAT if WHO 4-symptom TB screen positive; syphilis serology (RPR/TPHA); blood glucose; urine albumin-to-creatinine ratio (TDF nephrotoxicity baseline). Serum CrAg is added if CD4 <100 cells/µL. This baseline investigation set drives ART regimen selection (TDF component requires renal safety), prophylaxis decisions (CD4 threshold for co-trimoxazole), and detection of subclinical co-infections.
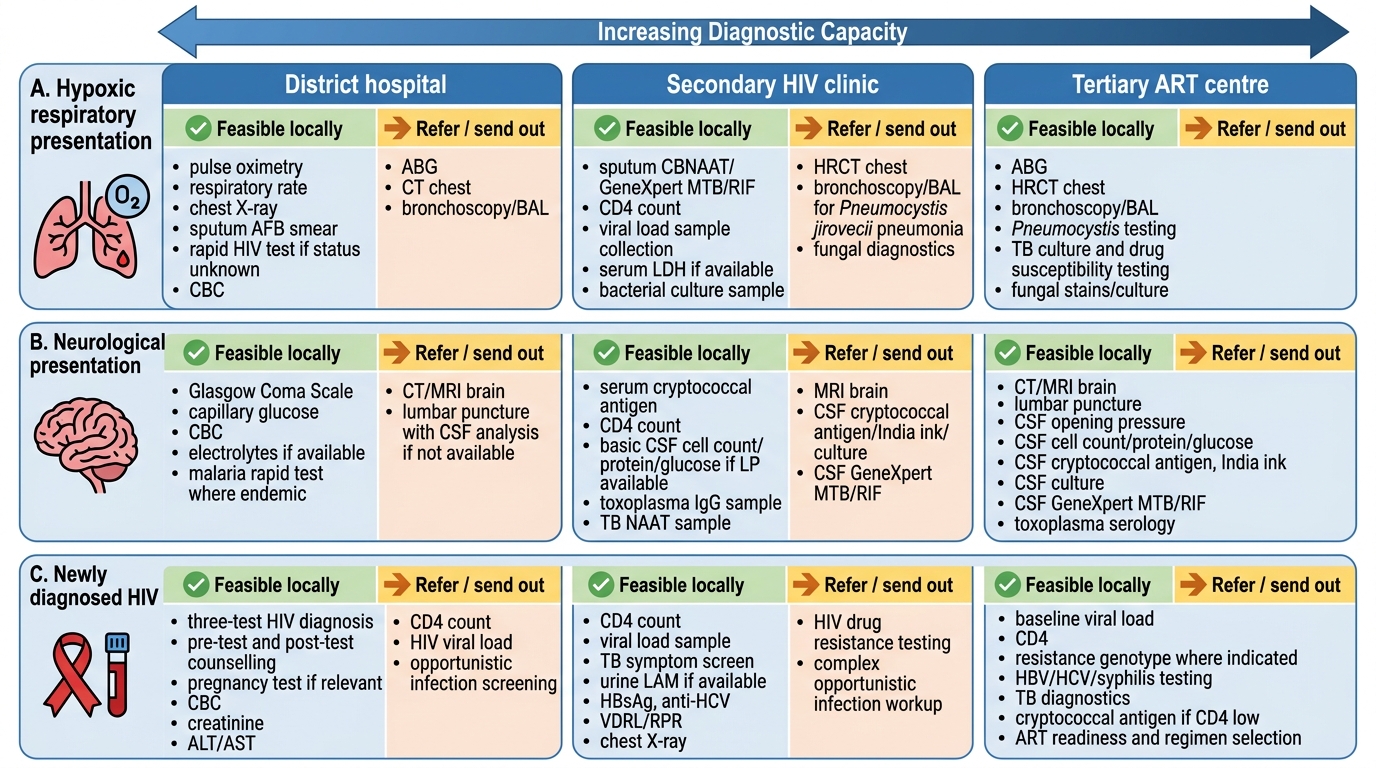
Tiered HIV Investigations by Setting and Presentation