Page 11 of 23
IM6.9-12 | HIV Diagnostic Testing — SDL Guide (Part 3)
Self-Assessment: Applying Diagnostic Reasoning in HIV
The scenarios below consolidate your ability to choose the right investigation for the right clinical context, interpret the result, and link it to the management decision. This is the 'choose and interpret' skill tested in IM6.9–IM6.12 at the SH level. For each scenario, select the most appropriate next investigation before reading the analysis, and explicitly state what result you are expecting and what that result will tell you about diagnosis and management.
Provided image
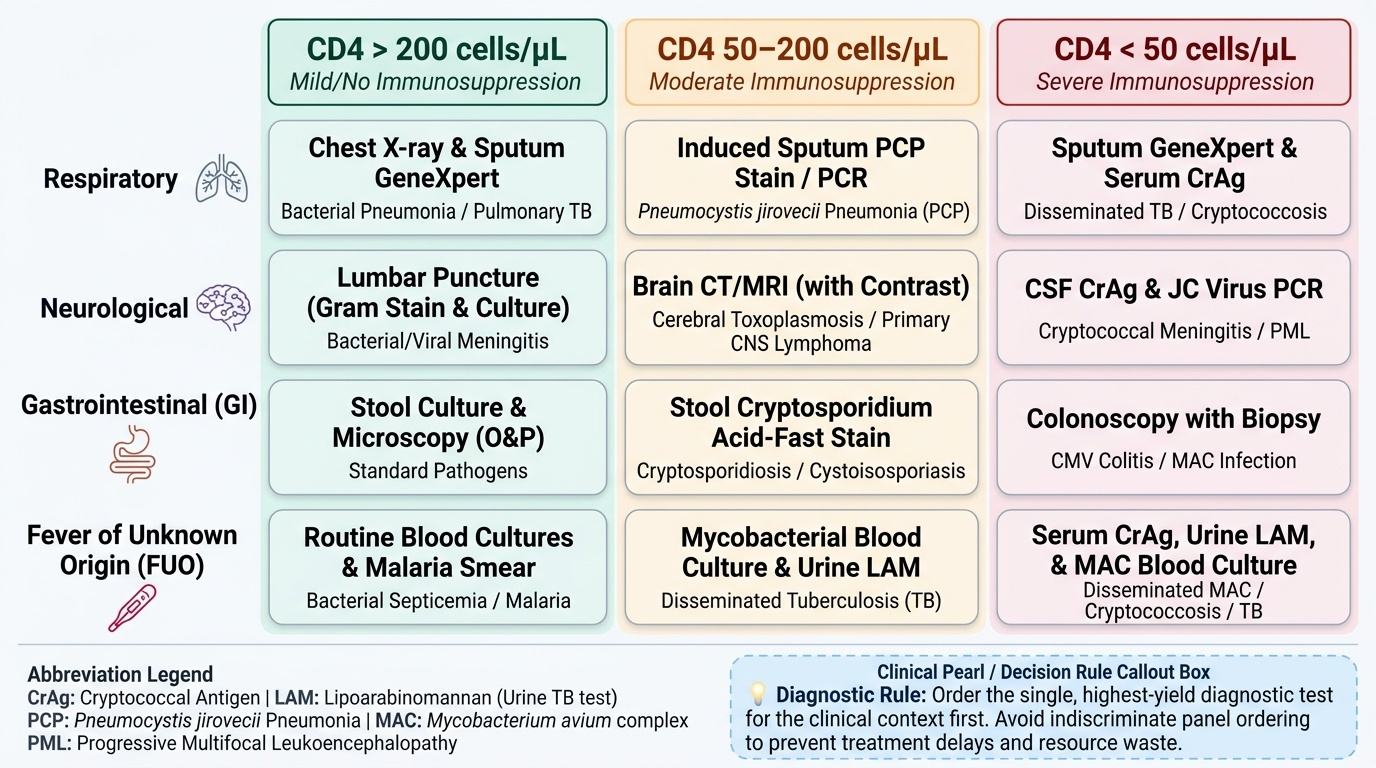
Applying diagnostic reasoning in HIV requires integrating three components: the presenting symptom, the estimated CD4 count (from history, clinical staging, or known result), and the sensitivity and specificity of available tests. The goal is not to order every test simultaneously, but to select the single most high-yield investigation that will either confirm or exclude the most likely diagnosis and change management. Over-investigation in resource-limited settings wastes resources and delays the clinical decision; under-investigation misses the diagnosis. The right choice requires knowing the sensitivity and specificity of each OI diagnostic test and the clinical context in which each is valuable.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
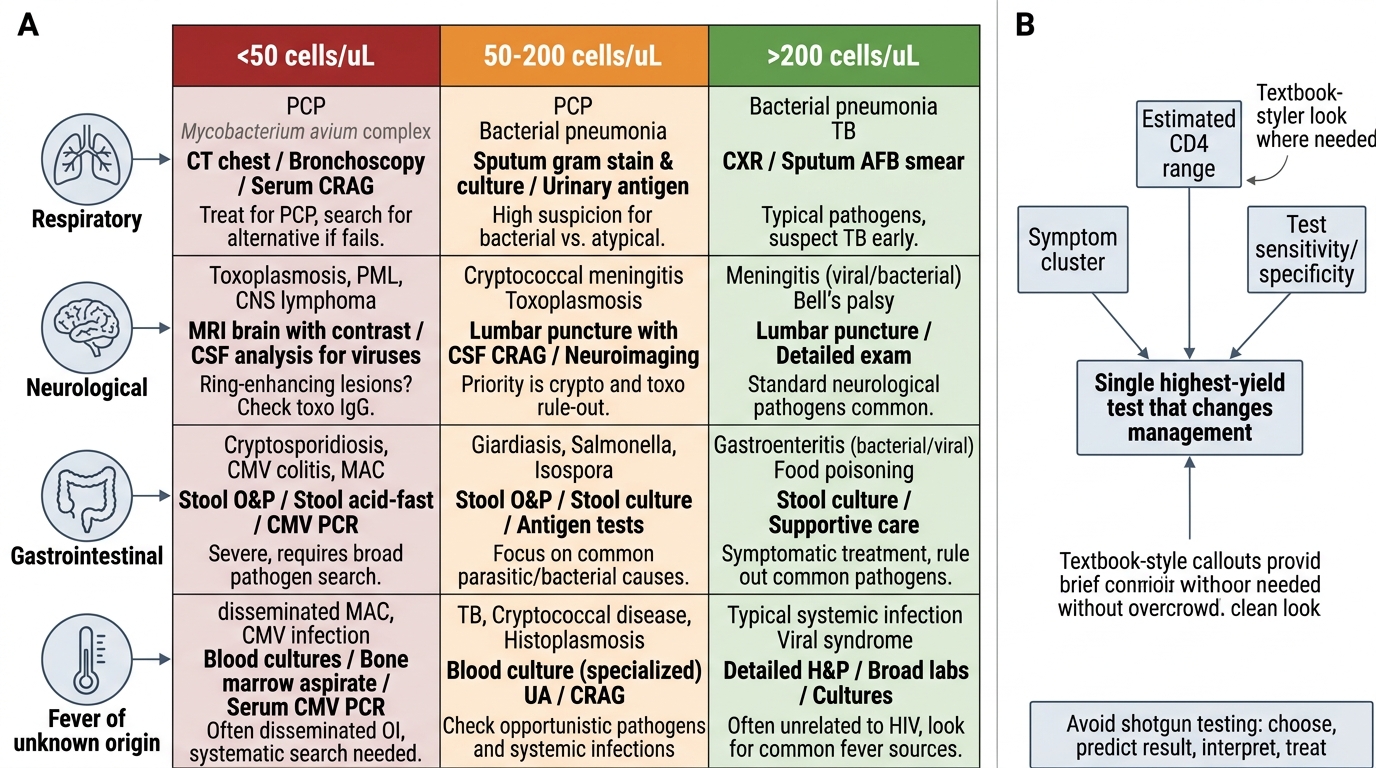
HIV OI Diagnostic Reasoning Grid
Scenario A: A 36-year-old HIV patient with CD4 count 44 cells/µL presents with 3 weeks of progressive exertional dyspnoea, dry cough, and fever. SpO₂ at rest is 89% on room air. CXR: bilateral perihilar ground-glass infiltrates. LDH: 820 IU/L. What is the single most important additional investigation to order immediately, and what management decision will the result guide?
Analysis: This is a clinical diagnosis of PCP (subacute onset, bilateral ground-glass, elevated LDH, CD4 <200). The most important additional investigation is ABG on room air — not to confirm PCP (which is a clinical diagnosis supported by the LDH, CXR, and clinical picture), but to determine whether adjunctive corticosteroids are indicated. PaO₂ <70 mmHg or A-a gradient >35 mmHg = corticosteroids mandatory. SpO₂ 89% at rest is already suggestive, but ABG provides the definitive threshold. Start high-dose TMP-SMX immediately (do not wait for BAL to confirm PCP).
Scenario B: A 28-year-old woman presents with three days of severe headache, fever, and vomiting. She is known HIV-positive with poor ART adherence. CD4 is 55 cells/µL. CT brain: no mass lesion. LP performed: opening pressure 38 cm H₂O; CSF clear; lymphocytes 8/mm³; protein 72 mg/dL; glucose 44 mg/dL (blood 88 mg/dL). India ink stain result is pending. What investigation should be ordered in parallel and what constitutes a positive result?
Analysis: While India ink stain is 70% sensitive, CSF cryptococcal antigen (CrAg) by LFA or ELISA should be ordered simultaneously — sensitivity >95%. A positive CrAg in CSF confirms cryptococcal meningitis definitively. Additionally, serum CrAg should be checked. The clinical picture (subacute meningitis + markedly raised ICP 38 cm H₂O + CD4 55 + mildly elevated protein + minimal pleocytosis) is already strongly suggestive — do not delay Amphotericin B + flucytosine pending all results; start therapy and perform therapeutic LP to lower the ICP.
Scenario C: A 3-month-old infant born to an HIV-positive mother is brought to the outpatient clinic. The mother is concerned about the baby's HIV status. A standard fourth-generation HIV Ag/Ab ELISA is performed and is negative. What is the CORRECT interpretation, and what is the appropriate test to order?
Analysis: Maternal anti-HIV IgG antibodies cross the placenta and persist in the infant for up to 18 months — therefore, a negative antibody test in a 3-month-old born to an HIV-positive mother does NOT exclude HIV infection. The correct test is HIV DNA PCR from dried blood spot (DBS) at 6 weeks, repeated at 9 months, and antibody test at 18 months for final diagnosis. NACO PPTCT guidelines specify this infant testing algorithm for all HIV-exposed infants.
CLINICAL PEARL
Three diagnostic pearls for HIV testing that are frequently tested. First: a normal CXR does not exclude PCP — in early or mild PCP, the CXR can be entirely normal while the patient has significant hypoxia; always perform a SpO₂ at rest and on exertion, and check LDH, in any HIV patient with unexplained dyspnoea. Second: standard stool bacterial cultures are negative in Cryptosporidium — you must specifically request modified acid-fast stain of stool; missing this instruction means missing the diagnosis. Third: maternal antibodies invalidate HIV antibody tests in infants up to 18 months — the infant diagnostic pathway uses DNA PCR, not ELISA.