Page 5 of 15
IM8.{8,10-12,16} | Hypertension Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a structured hypertension history covering duration, symptoms, comorbidities, lifestyle, risk factors, family history, and psychosocial factors
- Generate a prioritised differential diagnosis for hypertension based on clinical features
- Select and interpret appropriate diagnostic workup investigations including CBC, urine routine, BUN, creatinine, electrolytes, uric acid, and ECG
- Perform and interpret a 12-lead ECG for hypertensive target organ damage
- Integrate history, examination, and investigations to confirm aetiology and stratify cardiovascular risk
INSTRUCTIONS
Accurate clinical evaluation of the hypertensive patient is a core clinical skill that integrates history-taking, examination, investigation selection, and ECG interpretation. This module takes you through each component systematically, teaching you how to elicit the right information, prioritise the differential diagnosis, choose the minimum necessary investigations, and interpret the findings to guide management.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 271 — Systemic Hypertension: History and Physical Examination (textbook)
- API Textbook of Medicine, 10th ed., Ch. 12 — Hypertension: Clinical Assessment (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 19 — Hypertension: Investigation (textbook)
- ACC/AHA 2017 High Blood Pressure Guideline — Clinical Evaluation (guideline)
- Indian Guidelines on Hypertension (IGH-IV) 2019 — Initial Assessment (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients attend the hypertension clinic on the same morning. The first, Suresh, is 42 years old. He mentions during routine enquiry that he has been having early-morning headaches for 6 months, snores heavily, and his wife says he stops breathing during sleep. His BMI is 34 kg/m². His BP is 158/96 mmHg on two readings. The second, Kavitha, is 28 years old, referred after a routine antenatal check showed persistent BP 162/104 mmHg. She is 28 weeks pregnant with her first child. Both patients have hypertension, but the history, examination findings, appropriate investigations, and likely differential diagnosis are entirely different. Suresh requires a sleep study and a metabolic panel; Kavitha needs immediate obstetric evaluation, urine protein quantification, and fetal wellbeing assessment. The clinical evaluation of hypertension is not a fixed protocol — it is a structured, patient-adapted inquiry that turns a blood pressure number into a diagnosis and a management plan. This module builds the framework to do that.
WHY THIS MATTERS
The clinical evaluation of hypertension is the gateway to every downstream decision — whether to treat, with which agents, how urgently, and whether to investigate for a secondary cause. In Indian outpatient medicine, a large proportion of hypertension is identified opportunistically or at first symptomatic presentation with a complication. Your ability to take a structured, targeted history — not just record a BP — is what separates competent care from a missed secondary cause, a delayed diagnosis of eclampsia, or an unrecognised hypertensive emergency. The NMC competencies IM8.8, IM8.10, IM8.11, IM8.12, and IM8.16 span the full clinical evaluation arc: from history-taking (SH) and differential diagnosis (SH) through investigation selection and interpretation (KH) to ECG performance and interpretation (P). This is a skill-heavy module — understanding the principles is necessary but not sufficient; you must practise each component in the clinical environment.
RECALL
Activate your prior knowledge before proceeding. Recall the components of a standard medical history: presenting complaint, history of presenting illness (duration, character, associated features, aggravating and relieving factors), past medical history, drug and allergy history, family history, social and occupational history, and systems review. For hypertension specifically, recall the major risk factor categories — non-modifiable (age, sex, ethnicity, family history) and modifiable (dietary sodium, obesity, physical inactivity, alcohol, smoking, psychological stress). Recall the RAAS and SNS pathways from the foundations module — these form the mechanistic basis for the clues in the history that point to specific secondary causes. Recall the 12-lead ECG lead placement and what each lead 'looks at' (inferior leads II, III, aVF; lateral leads I, aVL, V5-V6; anterior leads V1-V4; right ventricular leads V1, V2). Also recall that the normal QRS duration is <120 ms, PR interval 120–200 ms, QTc <440 ms in men and <460 ms in women.
Clinical Indication and Structured History-Taking in Hypertension
Every clinical encounter with a hypertensive patient — whether newly diagnosed, established on treatment, or presenting with a complication — requires a structured and comprehensive history. The history in hypertension is not merely a checklist; it is a targeted clinical enquiry designed to answer four specific questions: (1) How severe is the hypertension and how long has it been present? (2) Is there evidence of target organ damage from history and symptoms? (3) Are there features suggesting a secondary (potentially reversible) cause? (4) What is the global cardiovascular risk, and what modifiable factors are present? Competency IM8.8 specifies that the history must cover duration and levels, symptoms, comorbidities, lifestyle factors, risk factors, family history, psychosocial and environmental factors, dietary assessment, and previous and concomitant therapy — each component serves one or more of these four diagnostic and risk-stratification purposes.
1. Duration and BP levels: How long has the patient known about elevated BP? Has it been measured previously, and if so, what were the readings? Was hypertension discovered incidentally (most common in primary HTN) or because of symptoms? A history of BP readings over time provides trend data and allows estimation of cumulative organ exposure. Young patients with no family history and sudden onset should raise suspicion of a secondary cause.
2. Symptoms: Most patients with primary hypertension are asymptomatic — but symptom enquiry is essential because: (a) symptoms may point to target organ damage (exertional dyspnoea, ankle swelling → HFpEF/HFrEF; chest pain → CAD; focal neurological symptoms → TIA/stroke; haematuria → hypertensive nephropathy); (b) symptoms may point to a secondary cause (episodic headache + palpitations + sweating → phaeochromocytoma; nocturia + polyuria + muscle weakness → primary aldosteronism; snoring + daytime somnolence + witnessed apnoeas → obstructive sleep apnoea; weight gain, easy bruising, proximal muscle weakness → Cushing syndrome); (c) symptoms of the consequences of untreated hypertension help risk-stratify the patient.
3. Comorbidities: Actively ask about diabetes mellitus, dyslipidaemia, chronic kidney disease, coronary artery disease, stroke or TIA, heart failure, peripheral arterial disease, atrial fibrillation, and gout (relevant because uric acid-lowering agents interact with antihypertensives, and thiazides raise uric acid). Each comorbidity influences the choice of antihypertensive drug class — for example, ACE inhibitors or ARBs are strongly preferred in hypertension with diabetes or CKD; beta-blockers may be preferred when CAD or AF coexists.
4. Lifestyle factors: Diet — specifically sodium intake (estimated from dietary recall: frequency of salty snacks, pickles, papads, preserved foods; added salt at table; restaurant eating), saturated fat intake; alcohol consumption (units per week — recall that alcohol raises BP dose-dependently above 2 units/day); physical activity (sedentary vs active); tobacco use (smoking raises acute BP and is an independent cardiovascular risk factor); and sleep (screen for sleep-disordered breathing with Epworth Sleepiness Scale and Berlin questionnaire items).
5. Family history: First-degree relatives with hypertension, premature cardiovascular disease (men <55 years, women <65 years), stroke, CKD, or diabetes. A positive family history increases the pre-test probability of primary hypertension; a negative family history in a young patient increases suspicion for a secondary or monogenic cause.
6. Psychosocial and environmental factors: Chronic work stress, marital or financial stress, socioeconomic deprivation, occupational exposures (noise, shift work), neighbourhood safety (affects exercise opportunities), and food access all independently contribute to hypertension and its treatment adherence. The API guidelines and WHO HEARTS programme emphasise psychosocial risk assessment as a component of comprehensive hypertension management.
7. Dietary assessment: Specifically estimated daily sodium intake (Indian diets average 8–12 g/day salt vs WHO recommendation of <5 g/day), fruit and vegetable consumption (potassium intake: DASH diet evidence), and saturated fat and refined carbohydrate intake (dyslipidaemia and insulin resistance contribution).
8. Previous and concomitant therapy: What antihypertensives has the patient previously taken, at what doses, and why were they stopped? (Cough → ACE inhibitor; ankle oedema → CCB; metabolic effects → thiazide). What other medications are being taken? — NSAIDs raise BP and blunt the effect of ACE inhibitors, ARBs, and diuretics; sympathomimetic decongestants; combined oral contraceptives; glucocorticoids; calcineurin inhibitors. Herbal supplements (liquorice — raises BP via pseudoaldosteronism). Adherence history — non-adherence is the commonest cause of apparent treatment failure.
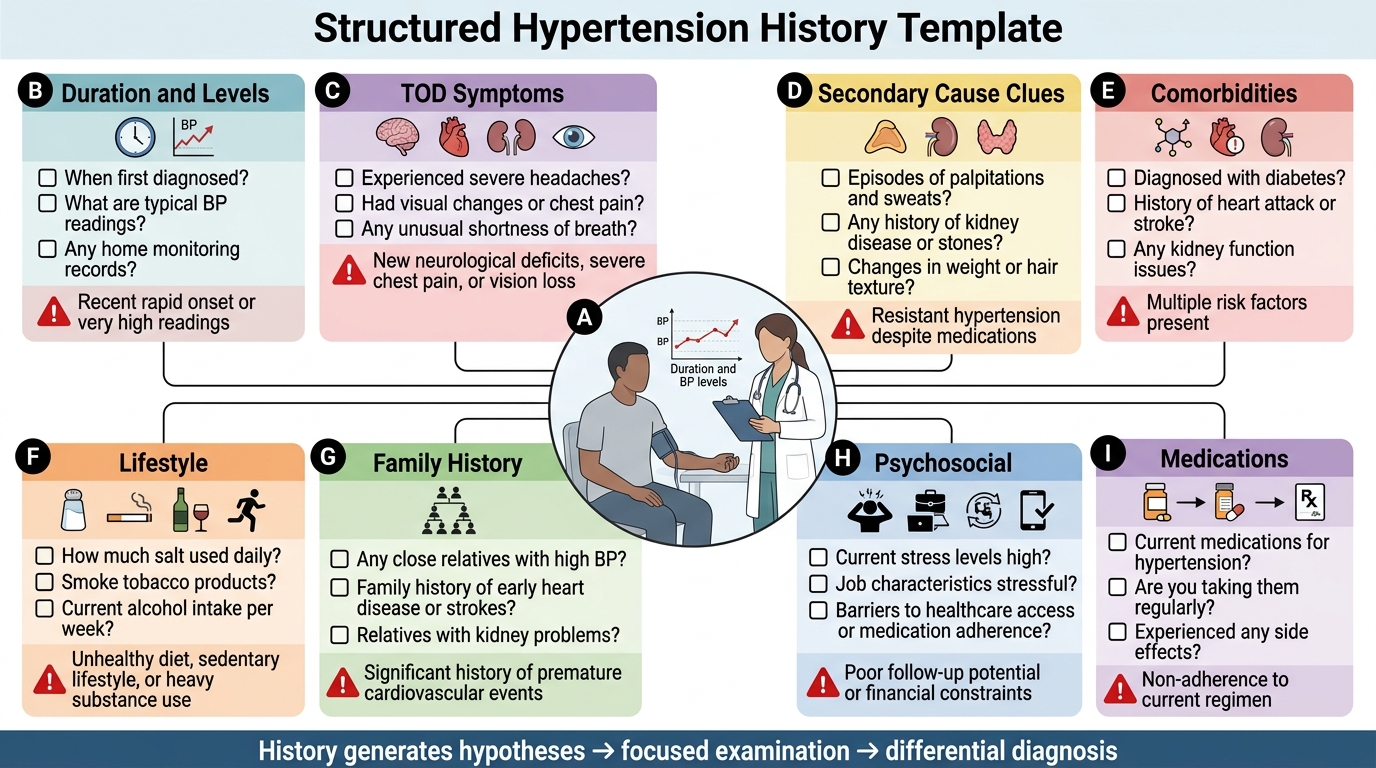
Structured Hypertension History Checklist
Physical Examination Principles and Generating the Differential Diagnosis
The physical examination in hypertension follows a focused protocol directed by the history, but always includes a standard set of components that assess BP severity, detect secondary cause signs, identify target organ damage, and estimate overall cardiovascular risk. The governing principle of the examination is that it tests clinical hypotheses generated by the history and adds findings that the history cannot provide — particularly anthropometric, cardiovascular, and fundoscopic data. Competency IM8.10 requires the student to generate a differential diagnosis and prioritise it based on clinical features that suggest a specific aetiology.
Standardised blood pressure measurement (both arms): Measure BP in both arms at least once — a difference of >15 mmHg between arms is significant and should raise suspicion for subclavian artery stenosis or, in younger patients, aortic coarctation. Always use the arm with the higher reading for subsequent monitoring. Measure in at least two positions (sitting, then standing after 1–2 minutes) to detect orthostatic hypotension, particularly important in elderly patients and those on diuretics or vasodilators.
Anthropometry: Height, weight, and waist circumference. Calculate BMI. Central obesity (waist circumference >90 cm in South Asian men, >80 cm in South Asian women) is a key marker of metabolic syndrome and insulin resistance. South Asian cut-offs are lower than WHO universal thresholds because South Asians have higher visceral fat at any given BMI.
Cardiovascular examination: Heart rate (tachycardia → sympathetic excess, thyrotoxicosis, phaeochromocytoma; bradycardia → check for beta-blocker, hypothyroidism); pulse character (large volume, bounding → aortic regurgitation or wide pulse pressure from severe hypertension; collapsing → aortic regurgitation); radio-femoral delay (coarctation); peripheral pulses (PAD); ankle oedema. Praecordial examination: apex beat displaced laterally (LV dilation) or forceful/heaving (LVH); heart sounds (S4 gallop = non-compliant LV, diastolic dysfunction; S3 gallop = dilated LV with systolic dysfunction, HFrEF); murmurs (aortic stenosis raises afterload).
Abdominal examination: Renal bruits (best heard para-umbilically, 2 cm lateral to midline) suggest renovascular hypertension. Palpable kidneys (polycystic kidney disease, hydronephrosis). Palpable abdominal aortic aneurysm (AAA) — found in elderly hypertensive males with a prominent pulsatile epigastric mass; confirm with ultrasound.
Neurological examination: Focal deficits (prior TIA or stroke), cognitive assessment (vascular dementia), papilloedema (emergency, KWB grade IV), retinal examination (KWB grades I–IV — essential in every hypertensive patient).
Endocrine examination: Truncal obesity, striae (Cushing); goitre (thyroid disease); moon face, proximal myopathy (Cushing); virilisation (adrenal tumour).
Generating and prioritising the differential diagnosis (IM8.10): After history and examination, the clinician should have a primary hypothesis and a ranked differential. The framework is:
- Primary (essential) hypertension — the default hypothesis when: middle-aged or older, positive family history, no specific secondary cause clues, obesity, high dietary sodium, sedentary. This accounts for 90–95% of cases.
- Secondary causes (elevated clinical priority when):
- Young age (<30–35) + no family history → Renovascular (FMD), Liddle syndrome, GRA, coarctation
- Hypokalaemia + spontaneous or diuretic-exacerbated → Primary aldosteronism (must screen in ALL hypertensive patients — prevalence 5–10%)
- Episodic BP spikes + headache + sweating + palpitations → Phaeochromocytoma/paraganglioma
- Cushingoid features → Cushing syndrome
- Snoring + daytime sleepiness + obesity → Obstructive sleep apnoea
- Pulse disparity arm-to-arm or arm-to-leg → Coarctation, subclavian stenosis
- Drug exposure: OCP, NSAIDs, steroids, calcineurin inhibitors → Drug-induced
- Resistant hypertension (uncontrolled on ≥3 drugs) → Always investigate for all secondary causes
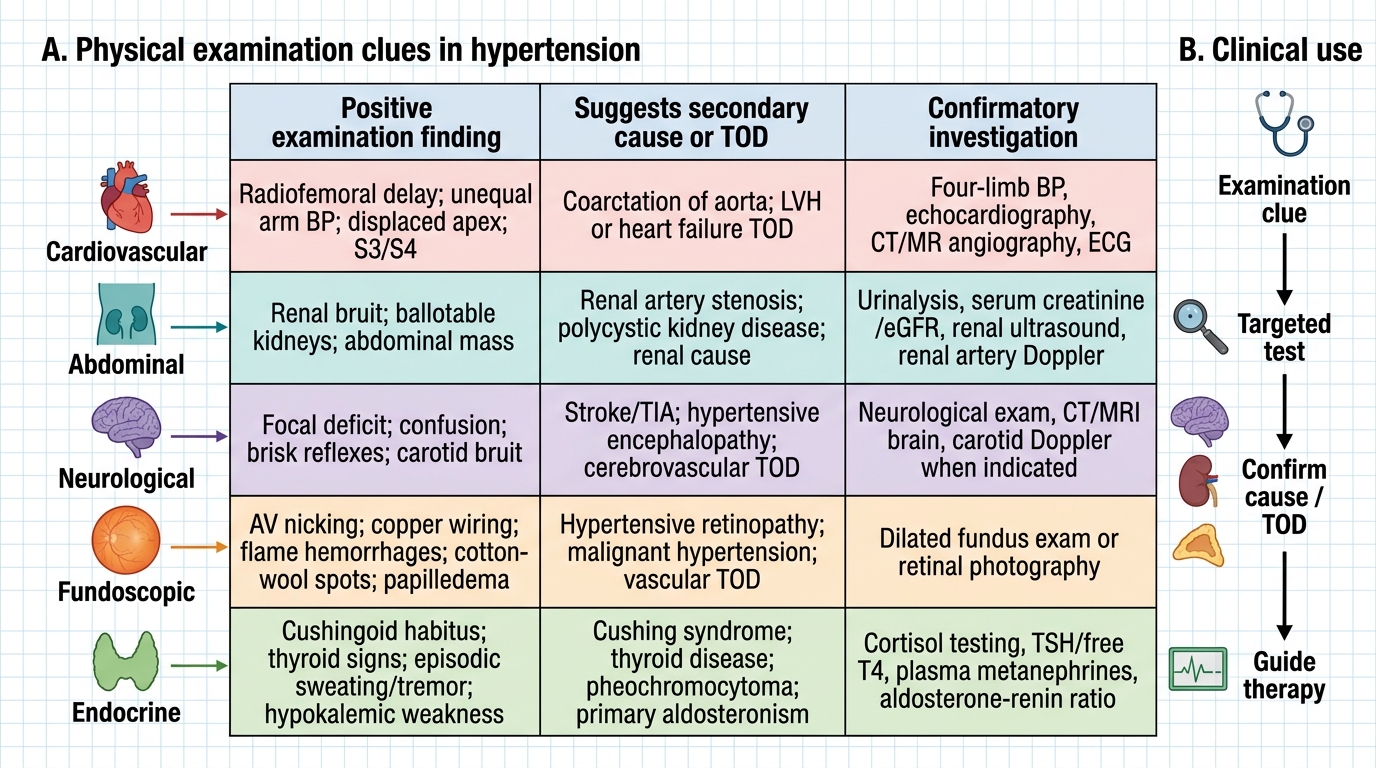
Physical Examination Clues in Hypertension
Diagnostic Workup: Investigations and Their Indications
The diagnostic workup in hypertension is the third major pillar of clinical evaluation, following history-taking and physical examination. It converts clinical hypotheses into quantitative evidence, establishes baselines for monitoring, and screens for treatable secondary causes and coexisting metabolic abnormalities that directly influence drug selection. A well-chosen, parsimonious investigation panel provides maximum diagnostic yield without unnecessary cost or patient burden — the ability to select and interpret these tests is the core of NMC competencies IM8.11 and IM8.12. The minimum mandatory panel is codified in guidelines and should be ordered in every newly diagnosed hypertensive patient, with additional targeted investigations layered on top based on clinical suspicion from the history and examination. Understanding the rationale for each investigation — not merely its name — is what allows the clinician to interpret an unexpected result correctly and take appropriate action. The investigations serve three concurrent purposes: (1) to identify end-organ damage at baseline and stratify cardiovascular risk; (2) to detect common secondary causes or metabolic abnormalities that modify drug selection; and (3) to provide a baseline for monitoring the effects of therapy over time. Competency IM8.11 requires selection of appropriate investigations based on the presumed aetiology; IM8.12 specifies the minimum mandatory panel and its interpretation. These investigations should be ordered in every newly diagnosed hypertensive patient, and some are repeated at follow-up to monitor organ function on treatment.
Complete blood count (CBC):
- Indications: Screen for anaemia (which can worsen cardiac loading and mask hypertension), polycythaemia (raises blood viscosity → raised SVR), and microangiopathic haemolytic anaemia (in malignant hypertension, thrombotic microangiopathy causes fragmented red cells and thrombocytopenia on blood film).
- Relevant findings: Low haemoglobin → anaemia (address separately, may worsen cardiac output demands); elevated haematocrit → polycythaemia vera or secondary polycythaemia; fragmented red cells (schistocytes) + low platelets + raised LDH → microangiopathic haemolytic anaemia (malignant hypertension or HUS/TTP overlap).
Urine routine (urinalysis and microscopy):
- Indications: The single most important non-blood test in initial hypertension evaluation. Detects early renal target organ damage and may reveal clues to secondary renal causes.
- Relevant findings: Proteinuria — even 1+ protein on dipstick warrants quantification with spot albumin-to-creatinine ratio (ACR); ACR 30–300 mg/g = microalbuminuria (earliest renal TOD); ACR >300 mg/g = overt proteinuria. Haematuria — suggests glomerulonephritis, IgA nephropathy, or other parenchymal renal disease as cause or consequence of hypertension; always exclude malignancy. Red cell casts — glomerulonephritis. Glucose — diabetes screen. Specific gravity and osmolality — renal concentrating capacity.
Blood urea nitrogen (BUN) and serum creatinine:
- Indications: Assess renal function (GFR) — both baseline and for monitoring; detect CKD (a cause and consequence of hypertension); identify AKI in hypertensive emergency. Always calculate eGFR using CKD-EPI or MDRD formula — creatinine alone is insufficient because serum creatinine underestimates GFR loss in patients with reduced muscle mass (elderly, women, malnourished).
- Relevant findings: Elevated creatinine / reduced eGFR → CKD (hypertensive nephrosclerosis, renovascular disease, diabetic nephropathy, or intrinsic renal disease); acute rise in creatinine after starting ACE inhibitor or ARB → bilateral renal artery stenosis (efferent arteriolar dilation drops GFR — a rise of ≤30% is acceptable; >30% or any rise in bilateral RAS → stop ACE inhibitor/ARB).
Serum electrolytes (sodium and potassium):
- Indications: Potassium is the key electrolyte in hypertension evaluation — it screens for primary aldosteronism and monitors the effects of diuretic therapy.
- Relevant findings: Hypokalaemia (<3.5 mEq/L) — if spontaneous (without diuretic), strongly suggests primary aldosteronism, renal tubular acidosis type 1, or Liddle syndrome; if on thiazide, may be drug-induced but still warrants ARR screening if severe or persistent. Hyperkalaemia (>5.5 mEq/L) — suggests CKD, Type IV RTA (hyporeninaemic hypoaldosteronism, common in diabetes), or from ACE inhibitor/ARB/potassium-sparing diuretic. Hyponatraemia — may follow thiazide therapy (especially in elderly women).
Serum uric acid:
- Indications: Elevated uric acid (hyperuricaemia) is associated with hypertension, metabolic syndrome, and CKD; it is elevated by thiazide diuretics. Important to document baseline before starting thiazide therapy, particularly in patients with a history of gout.
- Relevant findings: Hyperuricaemia (>7 mg/dL in men, >6 mg/dL in women) — increases risk of gout with thiazide use; may indicate CKD or metabolic syndrome; losartan (an ARB) has a mild uricosuric effect and is preferred in hypertensive patients with gout.
Fasting blood glucose and HbA1c:
- Indications: Diabetes is present in approximately 30–40% of hypertensive patients in India; fasting glucose is part of the routine metabolic panel. HbA1c is preferred for diagnosis and monitoring.
- Relevant findings: Fasting glucose ≥126 mg/dL or HbA1c ≥6.5% on two occasions = diabetes; fasting 100–125 mg/dL or HbA1c 5.7–6.4% = pre-diabetes. Hypertension + diabetes mandates ACE inhibitor or ARB as preferred antihypertensive (RAAS blockade reduces proteinuria and delays CKD progression).
Fasting lipid profile (total cholesterol, LDL, HDL, triglycerides):
- Indications: Dyslipidaemia is very commonly co-present with hypertension (metabolic syndrome). Lipid profile is required to calculate 10-year cardiovascular risk (e.g., Framingham risk score or PCE — pooled cohort equations).
- Relevant findings: LDL >130 mg/dL in a hypertensive patient without diabetes suggests statin therapy in addition to antihypertensives. Triglycerides >150 mg/dL + low HDL + central obesity = metabolic syndrome.
ECG (12-lead): Covered in the dedicated section below (IM8.16).
Additional investigations based on clinical suspicion:
- Plasma aldosterone-to-renin ratio (ARR): all patients with spontaneous hypokalaemia, resistant hypertension, or adrenal incidentaloma
- 24-hour urinary metanephrines: suspected phaeochromocytoma
- 24-hour urinary free cortisol or overnight DST: suspected Cushing syndrome
- Renal Doppler / CT angiography: suspected renovascular HTN (abdominal bruit, young patient, rapid-onset resistant HTN)
- Thyroid function tests (TSH, T4): all patients with unexplained weight change, palpitations, or cold/heat intolerance
- Echocardiography: to assess LVH (more sensitive than ECG), diastolic function, LVEF, and valve pathology — recommended when ECG shows LVH or patient has symptoms of HF
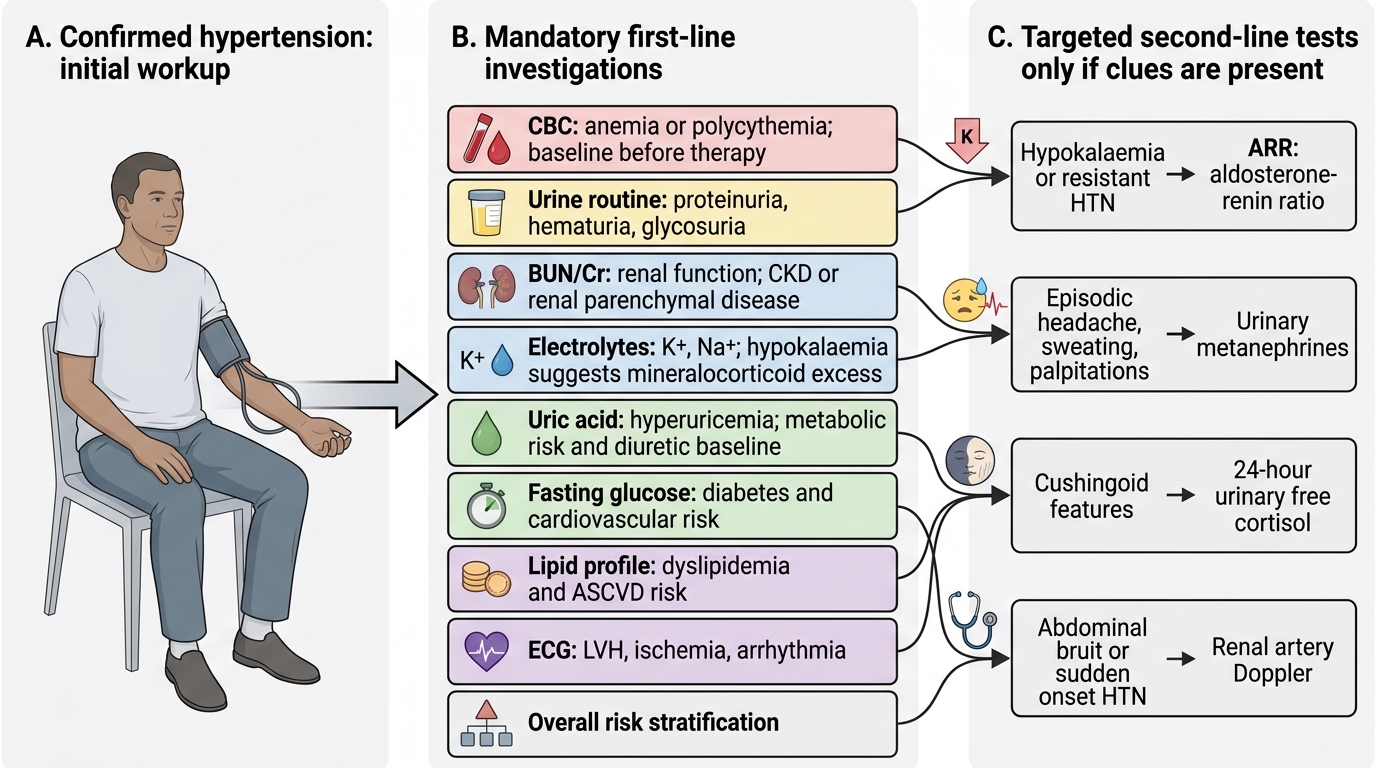
Initial Diagnostic Workup in Hypertension