Page 6 of 15
IM8.{8,10-12,16} | Hypertension Clinical Evaluation — SDL Guide (Part 2)
ECG Performance and Interpretation in Hypertension
The 12-lead ECG is a mandatory baseline investigation in every hypertensive patient and the most widely available tool for detecting cardiac target organ damage at the bedside or in the outpatient setting. It is inexpensive, non-invasive, reproducible, and provides information that physical examination and blood tests alone cannot supply — specifically, evidence of left ventricular hypertrophy with voltage criteria, the strain pattern that indicates subendocardial pressure-overload ischaemia, left atrial enlargement from diastolic dysfunction, arrhythmias including atrial fibrillation, and conduction system disease from hypertensive fibrosis. The ECG also serves as a longitudinal monitoring tool: regression of LVH voltage on serial ECGs is a validated marker of effective BP control and is associated with reduced cardiovascular event rates. Competency IM8.16 is a P-level (procedural) competency — theoretical knowledge of ECG interpretation is necessary but not sufficient; you must perform and interpret supervised ECGs in the clinical environment as well. This section covers both the practical technique of electrode placement and the systematic approach to ECG interpretation in the hypertensive patient.
Performing the 12-lead ECG — standard technique:
The patient lies supine, resting, skin dry and free of hair or cream at electrode sites. Limb electrodes are placed on the inner aspects of the wrists and inner aspects of the ankles (or the distal limbs). Chest (precordial) leads must be placed precisely:
- V1: 4th intercostal space (ICS), RIGHT sternal border
- V2: 4th ICS, LEFT sternal border
- V3: Between V2 and V4 (equidistant)
- V4: 5th ICS, mid-clavicular line
- V5: Anterior axillary line, same horizontal level as V4
- V6: Mid-axillary line, same horizontal level as V4 and V5
Standard settings: paper speed 25 mm/sec, amplitude calibration 10 mm = 1 mV (so 1 small box = 0.04 s, 1 large box = 0.2 s). Common pitfalls: misplaced precordial leads (V1/V2 too high — poor R wave progression); limb lead reversal (right arm/left arm swap — inverts lead I, aVR, creates apparent LBBB pattern); patient movement or electrical interference causing artefact.
What to look for on the ECG in a hypertensive patient:
The ECG reading should follow a systematic sequence: Rate → Rhythm → Axis → P waves → PR interval → QRS duration → QRS morphology → ST segments and T waves → QT interval → Overall impression.
1. Left ventricular hypertrophy (LVH) — the key target organ damage finding:
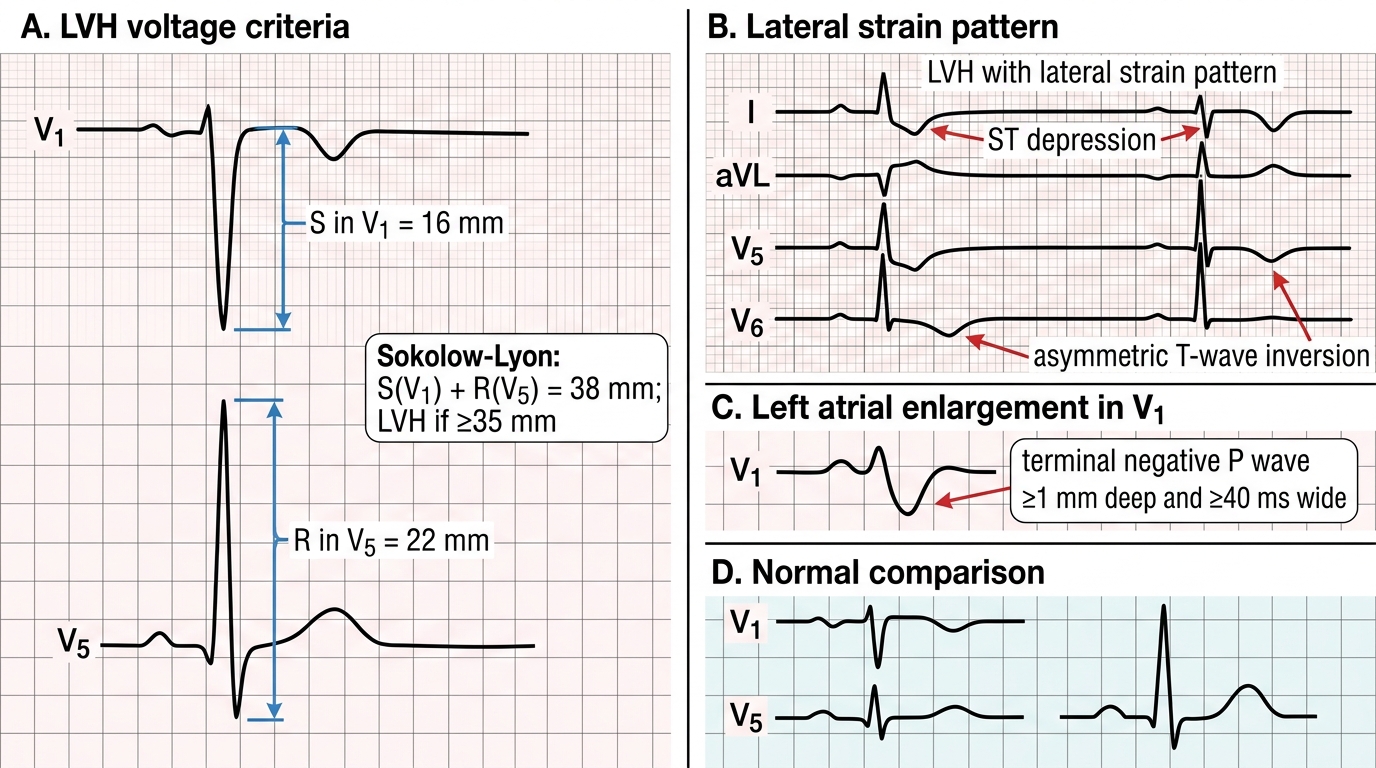
Voltage criteria:
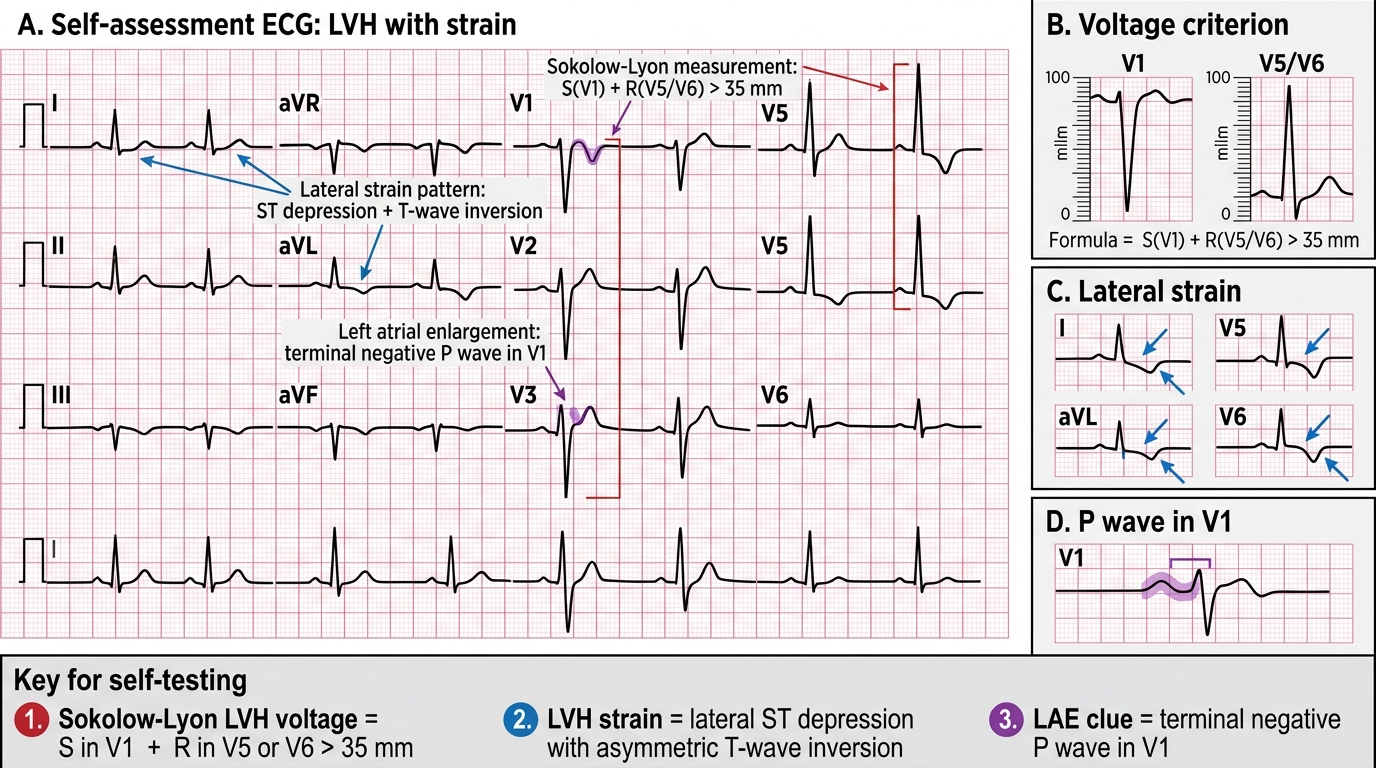
- Sokolow-Lyon criteria: S in V1 + R in V5 or V6 ≥35 mm. Sensitivity ~50%, specificity ~90%. Most commonly used.
- Cornell voltage criteria: R in aVL + S in V3 >28 mm in men; >20 mm in women.
- Romhilt-Estes point score: a composite scoring system incorporating voltage, repolarisation, and axis — score ≥5 points = definite LVH; 4 points = probable LVH.
Strain pattern: ST depression with T wave inversion (asymmetric, downsloping) in lateral leads (I, aVL, V5, V6) in the presence of LVH voltage criteria is called LVH with strain — it indicates subendocardial ischaemia from pressure-overload and significantly increases cardiovascular risk beyond LVH alone. It must be distinguished from ischaemic ST-T changes (which are typically symmetric and may occur in leads without LVH voltage).
Sensitivity limitation: ECG LVH criteria have only ~50% sensitivity for detecting anatomical LVH as confirmed by echocardiography. A normal ECG does NOT exclude LVH — echocardiography is the gold standard for LV mass measurement.
2. Left atrial enlargement (P-mitrale pattern): P-wave duration >120 ms (>3 small boxes), notched bifid P wave in lead II, negative terminal deflection of P wave in V1 >1 mm deep and >40 ms wide. Reflects elevated LA pressure from diastolic dysfunction or mitral regurgitation secondary to LVH — both common in hypertensive heart disease.
3. Atrial fibrillation: Absent P waves, irregularly irregular RR intervals, fibrillatory baseline. Hypertension is the commonest risk factor for AF (accounts for >40% of AF population-attributable risk). New AF in a hypertensive patient requires rate control, anticoagulation assessment using CHA₂DS₂-VASc score (HTN = 1 point), and investigation for structural heart disease.
4. Conduction abnormalities: Left bundle branch block (LBBB: QRS ≥120 ms, broad notched R in I, aVL, V5-V6; deep S in V1; T waves discordant) may result from hypertensive fibrosis of the conduction system. New LBBB in the context of chest pain should be treated as STEMI equivalent. Left anterior fascicular block (LAFB: left axis deviation ≥-45°, small q in I/aVL, small r in II/III/aVF, normal QRS duration) is the commonest conduction abnormality in LVH.
5. Ischaemic changes: Horizontal or downsloping ST depression, T wave inversion, Q waves, or ST elevation may reflect coexisting CAD — hypertension accelerates atherosclerosis. Differentiate from LVH strain by distribution and morphology.
6. QTc prolongation: QTc >440 ms in men, >460 ms in women. May occur in hypertensive patients with LVH (increased spatial dispersion of repolarisation); increased risk of ventricular arrhythmias. Monitor QTc when prescribing drugs that prolong QT (macrolides, antifungals, Class Ia/III antiarrhythmics).
Hypertensive ECG Findings: LVH, Strain, and Left Atrial Enlargement
SELF-CHECK
A 50-year-old hypertensive man has an ECG showing: S in V1 = 16 mm, R in V5 = 22 mm. There is ST depression with asymmetric T-wave inversion in leads I, aVL, V5, and V6. Which of the following best describes the ECG interpretation?
A. Anterior myocardial infarction — STEMI equivalent
B. Left bundle branch block (LBBB)
C. Left ventricular hypertrophy with strain pattern
D. Right ventricular hypertrophy
Reveal Answer
Answer: C. Left ventricular hypertrophy with strain pattern
Sokolow-Lyon criteria: S in V1 (16 mm) + R in V5 (22 mm) = 38 mm — this exceeds the threshold of ≥35 mm, meeting LVH voltage criteria. ST depression with asymmetric downsloping T-wave inversion in lateral leads (I, aVL, V5, V6) in the context of LVH voltage is the strain pattern, indicating subendocardial pressure-overload ischaemia from LVH — not primary CAD. STEMI would show ST elevation. LBBB requires QRS ≥120 ms and a broad notched R in lateral leads — not described here. Right ventricular hypertrophy causes right axis deviation and tall R in V1, not seen here. LVH with strain is a significant marker of hypertensive target organ damage and predicts adverse cardiovascular events.
Integrating Findings: Cardiovascular Risk Stratification and Applied Clinical Evaluation
The clinical evaluation of hypertension does not end with collecting individual data points — the history, examination, and investigation results must be synthesised into an integrated clinical picture that determines treatment urgency, drug selection, and follow-up intensity. This integration step is the highest-order skill in hypertension evaluation and represents the transition from data-gathering to clinical reasoning. A student who can recite BP staging, name the secondary causes, and list investigation findings has completed the foundation; a competent clinician additionally combines these to answer three critical questions: How severe is this patient's hypertension burden and cardiovascular risk? Is there a specific aetiology requiring targeted treatment or reversal? What should happen next — today, in 4 weeks, and in 6 months? The remaining competencies in this module (IM8.10 — differential diagnosis, IM8.11 — investigation selection) converge here in applied clinical decision-making. Competency IM8.10 specifically requires generation and prioritisation of a differential diagnosis from clinical features. This section applies the framework built across the preceding steps to real-world clinical integration.
Cardiovascular risk stratification in hypertension combines BP level, additional cardiovascular risk factors, the presence of comorbidities (diabetes, CKD), and evidence of target organ damage or established cardiovascular disease. The European Society of Hypertension (ESH 2023) and ACC/AHA 2017 frameworks both use this multi-factorial approach:
- Low risk: Stage 1 HTN only, no additional risk factors, no TOD, no diabetes, no CVD
- Moderate risk: Stage 1-2 HTN + 1-2 risk factors
- High risk: Stage 1-2 HTN + ≥3 risk factors, OR metabolic syndrome, OR TOD (LVH, microalbuminuria, retinopathy grade I-II)
- Very high risk: Stage 2-3 HTN + established CVD, CKD stage ≥3, diabetes with TOD, OR any patient with hypertensive emergency or BP ≥180/110
The risk category drives treatment decisions: low-risk patients may have a 3–6 month lifestyle trial before drug initiation; high- and very-high-risk patients require immediate pharmacological treatment.
Applied clinical decision-making — the integrated evaluation framework:
Step 1 — Confirm the diagnosis: Is this truly hypertension (two or more readings on two or more occasions)? Could this be white-coat hypertension (elevated in clinic but normal out-of-clinic)? Consider home BP monitoring (HBPM) or 24-hour ambulatory BP monitoring (ABPM) when clinic readings are borderline or inconsistent.
Step 2 — Assess urgency: Is there acute target organ damage (→ emergency) or no acute damage (→ urgency or routine)? This has already been covered in the foundations module but must be re-evaluated at every clinical encounter.
Step 3 — Identify secondary cause: Use the clinical clues from history and examination to determine whether targeted secondary cause investigations are indicated. Do not wait for the full workup to treat severe hypertension — treatment and investigation proceed in parallel.
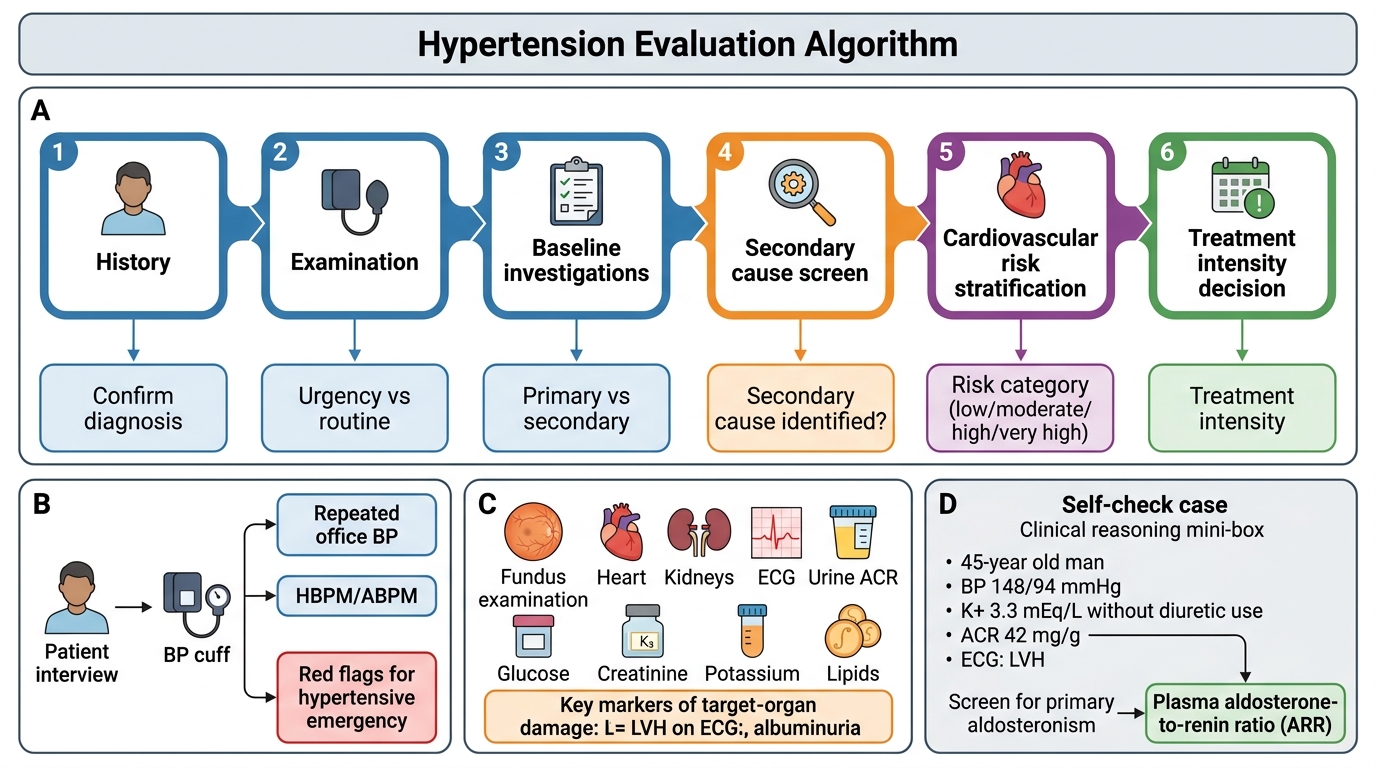
Step 4 — Quantify baseline organ function and risk factors: Minimum panel (CBC, urine ACR, BUN/Cr/eGFR, electrolytes, uric acid, fasting glucose, lipids, ECG). Add targeted tests as directed by clinical clues.
Step 5 — Stratify cardiovascular risk: Combine BP stage + risk factors + comorbidities + TOD to assign risk category and determine treatment threshold and target.
Step 6 — Select treatment: Drug choice is individualised based on comorbidities, contraindications, side-effect profiles, cost, and adherence considerations.
Step 7 — Define follow-up: Frequency of BP monitoring, repeat laboratory tests (electrolytes, creatinine — especially after starting ACE inhibitor/ARB or diuretic), urine ACR annually, ECG at 1 year to assess LVH regression, ophthalmology referral for fundoscopy.
Special populations:
- Elderly patients (≥65 years): Isolated systolic hypertension predominates; orthostatic hypotension must be checked; targets may be less aggressive (SBP 130–140 mmHg in frail elderly); check for polypharmacy and drug interactions; thiazide-like diuretics (indapamide, chlorthalidone) preferred over thiazide (hydrochlorothiazide) for better outcome data.
- Young patients (<40 years): Secondary cause workup essential; FMD and coarctation are important; reproductive implications (ACE inhibitors/ARBs are teratogenic — switch before conception).
- Pregnant women: Hypertension in pregnancy = systolic ≥140 or diastolic ≥90; emergency threshold = ≥160/110 (IV labetalol or IV hydralazine); safe oral agents: methyldopa, labetalol, nifedipine; contraindicated: ACE inhibitors, ARBs, renin inhibitors (all teratogenic); magnesium sulphate for seizure prophylaxis in eclampsia.
- Diabetes + CKD: ACE inhibitor or ARB is the preferred antihypertensive (nephroprotective beyond BP effect); target BP <130/80 mmHg; monitor potassium and creatinine closely.
Integrated Hypertension Evaluation Algorithm
SELF-CHECK
A 45-year-old man with BP 148/94 mmHg has: fasting glucose 118 mg/dL, urine ACR 42 mg/g, serum creatinine 1.0 mg/dL, LDL 142 mg/dL, ECG showing Sokolow-Lyon criteria met (38 mm). Serum K+ is 3.3 mEq/L on no diuretic. What is the most important NEXT investigation?
A. 24-hour ambulatory blood pressure monitoring (ABPM)
B. Echocardiography for LV mass quantification
C. Plasma aldosterone-to-renin ratio (ARR)
D. Renal Doppler ultrasound for renovascular disease
Reveal Answer
Answer: C. Plasma aldosterone-to-renin ratio (ARR)
The combination of hypertension with spontaneous hypokalaemia (K+ 3.3 mEq/L without diuretic use) is the strongest clinical trigger for primary aldosteronism — the most commonly missed secondary cause of hypertension, with a prevalence of 5–10% among hypertensive patients. The plasma ARR is the first-line screening test; an elevated ratio (high aldosterone, suppressed renin) indicates autonomous aldosterone excess. All other investigations listed are relevant but secondary: ABPM is for diagnosing white-coat or masked hypertension; echocardiography is appropriate given ECG LVH but not the most urgent next test; renal Doppler is appropriate if there is an abdominal bruit or young patient without family history, neither specified here. The hypokalaemia takes diagnostic priority and must be investigated before selecting drug therapy.
Self-Assessment: Clinical Evaluation Integration
This section consolidates the clinical evaluation skills covered across this module. For each scenario, apply the structured evaluation framework — history components, examination priorities, investigation selection, ECG interpretation, and differential diagnosis — before reading the analysis. These exercises target the SH-level competencies (IM8.8 and IM8.10) and the KH-level interpretation skills (IM8.11, IM8.12) required in a supervised clinical encounter.
Scenario A — History-Directed Investigation:
Ananya, 36 years old, presents with newly discovered hypertension (BP 168/104 mmHg). She has gained 12 kg in the past year, has prominent striae on her abdomen, and her face appears round and plethoric. She reports easy bruising and difficulty climbing stairs. She is on no medications. Her serum glucose is 148 mg/dL (fasting). What secondary cause should you prioritise, and which is the most appropriate first-line investigation?
Analysis: The history and examination are highly suggestive of Cushing syndrome — weight gain, centripetal obesity, abdominal striae (typically violaceous), easy bruising, proximal myopathy (difficulty climbing stairs), and hypertension + hyperglycaemia. The most appropriate first-line investigation is either a 24-hour urinary free cortisol or late-night salivary cortisol or overnight dexamethasone suppression test — any one of these is acceptable as a first-line screen per Endocrine Society guidelines; the overnight DST (1 mg dexamethasone at 11 PM → measure cortisol at 8 AM next day: >50 nmol/L = abnormal) is the most practical in outpatients.
Scenario B — ECG Interpretation:
The ECG of a 55-year-old hypertensive man shows: S in V1 = 14 mm, R in V6 = 18 mm (Sokolow-Lyon = 32 mm — just below threshold). Axis is -40°. P wave in lead II is 130 ms wide with a notch. There is a small negative terminal deflection in V1. HR 78, rhythm regular. PR 170 ms. QRS 90 ms. No ST changes.
Analysis: Sokolow-Lyon voltage (32 mm) does not meet the ≥35 mm threshold — so this does NOT meet ECG LVH by Sokolow-Lyon. However, the axis of -40° meets left anterior fascicular block (LAFB) criteria (left axis deviation ≥-45° is strict cut-off; -40° is borderline — some guidelines use ≥-30°). The P wave in lead II (130 ms, notched) and negative terminal deflection in V1 meet criteria for left atrial enlargement (P-mitrale pattern) — a sign of elevated LA pressure from diastolic dysfunction, even without LVH voltage. This patient should have echocardiography to look for LVH (which ECG may miss in ~50% of cases) and diastolic function assessment.
Scenario C — Investigation Interpretation:
A hypertensive patient on hydrochlorothiazide 12.5 mg/day returns for review. His serum creatinine has risen from 0.9 to 1.2 mg/dL (eGFR from 82 to 59 mL/min/1.73m²) and serum K+ is now 5.8 mEq/L. He was started on ramipril (an ACE inhibitor) 4 weeks ago. How should you interpret these changes and what action is required?
Analysis: A rise in creatinine after starting an ACE inhibitor is expected because ACE inhibitors dilate the efferent arteriole, reducing intraglomerular pressure and thus GFR. A rise of ≤30% from baseline is acceptable and does not require drug cessation. Here, creatinine rose from 0.9 to 1.2 mg/dL — approximately 33% rise — which is marginally above the 30% acceptable threshold. The hyperkalaemia (K+ 5.8 mEq/L) is also a concern with combined ACE inhibitor + CKD progression. Actions: (1) Recheck creatinine and K+ in 1–2 weeks — if the creatinine rise has stabilised and K+ is below 6.0 mEq/L, cautious continuation is reasonable with dietary potassium restriction; (2) If K+ rises further or creatinine continues to climb, consider dose reduction or switch to a CCB-based regimen; (3) Importantly: if bilateral renal artery stenosis was not excluded prior to starting ACE inhibitor, this scenario mandates renal Doppler imaging to rule it out.
ECG Self-Assessment: LVH With Strain Pattern
CLINICAL PEARL
The 12-lead ECG is both a minimum mandatory baseline and a direct window into hypertensive cardiac damage — but its limitations must be respected. Sokolow-Lyon criteria miss approximately 50% of patients with anatomical LVH proven on echocardiography; a 'normal ECG' does not mean 'no cardiac damage'. Always escalate to echocardiography when the history (exertional dyspnoea, orthopnoea) or examination (displaced apex, S4 gallop) suggests hypertensive heart disease, even if the ECG is unremarkable. Conversely, do not attribute ECG voltage criteria of LVH to hypertension in a thin young patient with a narrow chest — isolated voltage LVH without strain or other features may reflect athletic remodelling or constitutional variance.
For the history: the triad of episodic severe headache + palpitations + diaphoresis in a hypertensive patient should trigger immediate consideration of phaeochromocytoma. This triad is both highly specific and potentially life-threatening — measuring 24-hour urinary metanephrines or plasma metanephrines before any surgical procedure in such a patient is mandatory. Starting a beta-blocker without prior alpha-blockade in a patient with phaeochromocytoma can precipitate a lethal hypertensive crisis.