Page 8 of 15
IM8.{13-15,17-19} | Hypertension Management and Follow-up — SDL Guide
Learning Objectives
- Develop an appropriate treatment plan for essential hypertension including lifestyle modifications and pharmacological therapy
- Recognise, prioritise, and manage hypertensive emergencies using appropriate IV agents and BP targets
- Communicate lifestyle modification advice on weight, alcohol, physical activity, and sodium intake to patients
- Counsel hypertensive patients and incorporate patient preferences in management decisions
- Describe the impact of hypertension on quality of life, wellbeing, work, and family
- Determine when specialist consultation is required in hypertension
INSTRUCTIONS
This module covers the full spectrum of hypertension management: the evidence basis for lifestyle modification, first-line drug classes and their compelling indications, combination therapy principles, hypertensive emergency recognition and acute management, patient counselling, and indications for specialist referral. Management decisions in hypertension are highly individualised — this module builds the framework for making those decisions systematically.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 271 — Treatment of Hypertension (textbook)
- API Textbook of Medicine, 10th ed., Ch. 12 — Management of Hypertension (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 19 — Management of Hypertension (textbook)
- ACC/AHA 2017 Guideline — Treatment Recommendations (guideline)
- Indian Guidelines on Hypertension (IGH-IV) 2019 — Drug Therapy (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Mohan is 48 years old when he is told he has hypertension — BP 156/98 mmHg — at a workplace health check. He is overweight (BMI 29 kg/m²), mildly active, drinks 4–5 beers on weekends, and eats a diet heavy in salted snacks. He has no symptoms. His serum creatinine is normal, his ECG is unremarkable, and his urine dipstick is negative for protein. He has no diabetes and no family history of cardiovascular disease. His 10-year ASCVD risk is 7%. Now consider Priya, 55 years old, who arrives in the emergency department with a severe headache, blurred vision, and confusion. Her BP is 214/138 mmHg. Her fundoscopy shows papilloedema. Her creatinine has risen acutely from a baseline of 0.9 to 2.1 mg/dL. Both patients have hypertension, but their management could not be more different: Mohan needs lifestyle modification with or without a single low-dose antihypertensive, education, and a 3-month follow-up; Priya needs an ICU bed, an intra-arterial line, IV nicardipine or labetalol, and a target to lower her mean arterial pressure by exactly 20–25% in the first hour — no more, no less. This module builds the framework to manage both.
WHY THIS MATTERS
Hypertension is the most prevalent condition you will manage throughout a medical career. Effective management — defined as achieving and sustaining BP below target — reduces the risk of stroke by 35–40%, myocardial infarction by 20–25%, and heart failure by >50%. Yet in India, only approximately 15% of hypertensive patients have their BP controlled, despite a growing array of effective, low-cost drugs. The gap between what is achievable and what is achieved is largely explained by barriers the final-year student must understand: patient non-adherence, prescriber hesitation, healthcare access, drug inertia, and inadequate counselling. Competencies IM8.13–IM8.19 span the full management arc: treatment planning (KH), emergency management (KH), lifestyle counselling (SH), patient communication (SH), quality-of-life impact (SH), and specialist referral criteria (KH). These are not isolated facts — they form an integrated management system.
RECALL
Before proceeding, activate the prior knowledge relevant to treatment. From the foundations module, recall: the four major antihypertensive drug classes — ACE inhibitors/ARBs (RAAS blockade), calcium channel blockers (CCBs, vasodilation), thiazide/thiazide-like diuretics (sodium excretion), and beta-blockers (heart rate + renin reduction). Recall the BP targets from ACC/AHA 2017: <130/80 mmHg for most patients with high cardiovascular risk; the JNC 7 / Indian guideline target of <140/90 mmHg. Recall the distinction between hypertensive urgency (no acute end-organ damage → oral agents, gradual reduction over 24–48 hours) and hypertensive emergency (acute end-organ damage → IV agents, MAP reduction ≤20–25% in 1 hour). Recall that hypertension management is lifelong — stopping medication causes BP to return to pre-treatment levels within weeks to months. This recall frame sets the context for the management decisions this module details.
When to Treat: Thresholds, Targets, and the Treatment Decision
The decision to initiate pharmacological antihypertensive therapy is a clinical judgement that integrates BP level, cardiovascular risk, the presence of target organ damage, comorbidities, and patient preference. It is emphatically not a purely threshold-based binary decision — the same blood pressure number in two different patients may mandate immediate drug therapy in one and a 3–6 month lifestyle trial in the other, based entirely on their individual cardiovascular risk profile. A patient with Stage 1 hypertension by ACC/AHA 2017 (130–139/80–89 mmHg) who also has diabetes, CKD, or established cardiovascular disease carries a very high 10-year event risk and should start drug therapy immediately alongside lifestyle modification; a patient with the identical BP level but no additional risk factors and a 10-year ASCVD risk below 10% can safely attempt lifestyle change first and be reassessed at 3 months. This risk-stratified approach avoids both under-treatment (failing to medicate high-risk patients promptly) and over-treatment (medicalising low-risk individuals who could achieve BP control without drugs). Understanding this framework is the entry point into competency IM8.13 — developing an appropriate treatment plan.
ACC/AHA 2017 guidance on when to start drug therapy:
- Stage 1 HTN (130–139/80–89 mmHg) with ASCVD risk <10%: lifestyle modification for 3 months first, then reassess
- Stage 1 HTN with ASCVD risk ≥10%, or known CVD/diabetes/CKD/HF: start drug therapy immediately alongside lifestyle modification
- Stage 2 HTN (≥140/≥90 mmHg): start drug therapy in all patients regardless of ASCVD risk, alongside lifestyle modification
- BP ≥160/100 mmHg: most guidelines recommend combination therapy from the outset
Indian guideline (IGH-IV 2019) treatment thresholds:
- Initiate therapy at ≥140/90 mmHg in most patients
- High-risk or very-high-risk patients: initiate at ≥130/80 mmHg
- Targets: <140/90 mmHg for most; <130/80 mmHg for high-risk patients (diabetes, CKD, established CVD)
BP targets — a nuanced view:
The question 'how low is low enough' has been addressed by major trials. The SPRINT trial (SBP target 120 vs 140 mmHg) showed significant reductions in cardiovascular events and mortality with intensive treatment — but SPRINT excluded diabetics, used automated office BP (which reads ~5–15 mmHg lower than conventional clinic BP), and showed increased AKI and hypotension in the intensive arm. The ACC/AHA 2017 guideline used SPRINT data to support a <130/80 target for high-risk patients. The ACCORD trial (diabetes patients) showed no additional cardiovascular benefit of targeting <120 vs <140 mmHg systolic — hence, in diabetic patients, the established target remains <130/80 mmHg. In elderly patients (≥65 years), the 2019 ACC/AHA guidelines recommend a SBP target of <130 mmHg for community-dwelling older adults without significant frailty; for frail elderly or those with multiple comorbidities, individualised targets (130–140 mmHg) are appropriate, prioritising avoidance of orthostatic hypotension and falls over aggressive BP reduction.
The concept of treatment urgency versus routine: As established in the foundations module, acute BP elevation with end-organ damage = emergency (immediate IV therapy); without end-organ damage = urgency (oral therapy over 24–48 hours) or routine (start on oral therapy, follow up in 1–4 weeks). The 'fire-drill instinct' to lower all high BP numbers immediately is one of the most common clinical errors; in urgency, precipitous lowering of BP in a patient whose cerebrovascular autoregulation has reset to higher pressures can cause ischaemic stroke or MI.
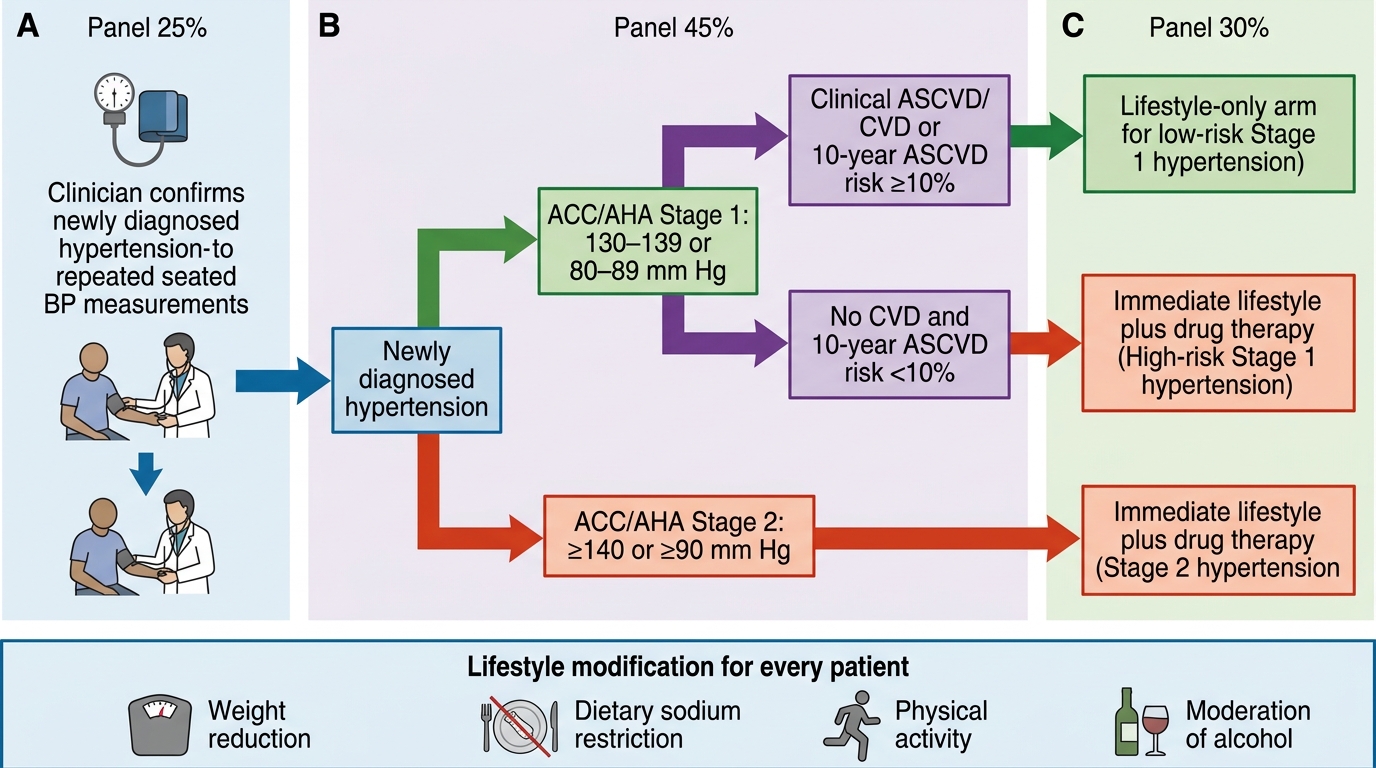
Decision Tree for Initiating Antihypertensive Treatment
Lifestyle Modification: Evidence, Quantified Benefits, and Patient Communication
Lifestyle modification is the cornerstone of hypertension management for every patient at every stage. It is not merely 'advice to give while waiting to prescribe drugs' — it has quantified, mechanism-based BP-lowering effects, addresses cardiovascular risk beyond BP alone, and in many Stage 1 patients can achieve BP control without drug therapy. Competency IM8.15 requires the student to develop and communicate specific lifestyle modification advice to patients: weight reduction, moderation of alcohol, physical activity, and dietary sodium. The word 'communicate' is deliberate — the SH-level competency requires not just knowledge but the ability to translate evidence into patient-accessible language that motivates behaviour change.
1. Dietary sodium restriction:
Mechanism: excess dietary sodium expands extracellular fluid volume, increases cardiac preload and output, and in salt-sensitive individuals (common in South Asian and Black populations, the elderly, and CKD patients) raises BP directly. Sodium exerts its hypertensive effect through volume-dependent and RAAS-blunting mechanisms. Evidence: the DASH-Sodium trial showed that reducing sodium intake from 3.5 g/day to 1.5 g/day (as sodium; equivalent to reducing salt from ~9 g to ~4 g/day) lowered systolic BP by 8.9 mmHg in hypertensives and 7.0 mmHg in normotensives. The WHO recommends <5 g salt/day (<2 g sodium/day); the average Indian diet contains 8–12 g salt/day — more than double the recommended level. Practical communication: advise reducing cooking salt by half; avoiding pickles, papads, and preserved/canned foods; limiting restaurant eating; not adding salt at the table. A useful metric: one teaspoon of salt ≈ 5–6 g; reducing to half a teaspoon per day is the practical target for cooking salt alone. Expected BP reduction: approximately 4–6 mmHg systolic.
2. Weight reduction:
Mechanism: central obesity activates the SNS, RAAS, and adipokines (leptin) that raise BP. Even modest weight loss reduces SNS activity, improves insulin sensitivity, reduces aldosterone levels, and lowers BP through multiple mechanisms. Evidence: a reduction of 1 kg of body weight is associated with an average SBP fall of approximately 1 mmHg. A 10 kg weight loss can reduce SBP by 5–20 mmHg. Target: achieving a BMI of 18.5–24.9 kg/m² or, pragmatically, a 5–10% reduction in body weight in overweight/obese patients. Waist circumference targets for South Asians: <90 cm in men, <80 cm in women. Practical communication: combine dietary calorie restriction with increased physical activity; avoid crash diets (they raise renin and aldosterone, blunting BP benefit); sustainable incremental reductions are more durable.
3. Physical activity:
Mechanism: regular aerobic exercise reduces cardiac output by lowering resting heart rate, improves baroreflex sensitivity, reduces SNS tone, and promotes NO-mediated vasodilation, all of which lower resting BP. Evidence: 30–45 minutes of moderate-intensity aerobic exercise (brisk walking, cycling, swimming) on most days of the week (≥5 days) reduces SBP by approximately 4–9 mmHg. The ACSM recommends 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic activity per week for hypertensive patients. Resistance training also provides a modest (∼2 mmHg) additional BP reduction. Practical communication: activities accessible to most patients include brisk walking, cycling, and yoga. Framing matters: 'Walk for 30 minutes every day, five days a week — that is the equivalent of taking a tablet that reduces your BP by 5 mmHg with no side effects.' Isometric exercise (extended static gripping) also has RCT evidence for BP reduction.
4. Moderation of alcohol:
Mechanism: alcohol raises BP dose-dependently above 2 standard drinks (20 g ethanol) per day, primarily through SNS activation, cortisol-mediated vasoconstriction, and interference with baroreceptor sensitivity. Heavy alcohol use is also associated with secondary hypertension and resistance to antihypertensive drugs. Evidence: reducing alcohol intake from heavy use (>3 drinks/day) to moderate use (<2 drinks/day) reduces SBP by approximately 2–4 mmHg. Abstinence in heavy drinkers can reduce SBP by up to 7–8 mmHg. Practical communication: express the limit in tangible units — in India, a standard unit = 10 g ethanol ≈ 30 mL of whisky/brandy ≈ 330 mL beer ≈ 150 mL wine; no more than 2 units/day for men, 1 unit/day for women.
5. Dietary pattern — DASH diet:
The DASH diet (Dietary Approaches to Stop Hypertension) emphasises: increased fruits and vegetables (potassium-rich), low-fat dairy, whole grains, lean protein, nuts and seeds, and reduced red meat, sweets, and sodium. The DASH diet reduces SBP by 8–14 mmHg in hypertensives — an effect comparable to a single antihypertensive drug. The mechanism is multifactorial: increased potassium (opposing sodium), increased magnesium and calcium, dietary fibre, and reduced saturated fat.
6. Tobacco cessation:
Smoking causes acute BP elevation (by 5–15 mmHg per cigarette for 20–30 minutes) through nicotine-mediated catecholamine release. Chronic smoking does not appear to cause sustained hypertension directly but dramatically amplifies cardiovascular risk in hypertensive patients — a hypertensive smoker has 3–5× the cardiovascular risk of a hypertensive non-smoker. Cessation is a mandatory cardiovascular risk reduction intervention in all hypertensive patients.
7. Stress management:
Chronic psychological stress activates the HPA axis and SNS, raising BP and contributing to FHA-related weight gain, alcohol use, and physical inactivity. Structured stress reduction (mindfulness, breathing exercises, progressive muscle relaxation) can lower SBP by 2–5 mmHg in some patients.
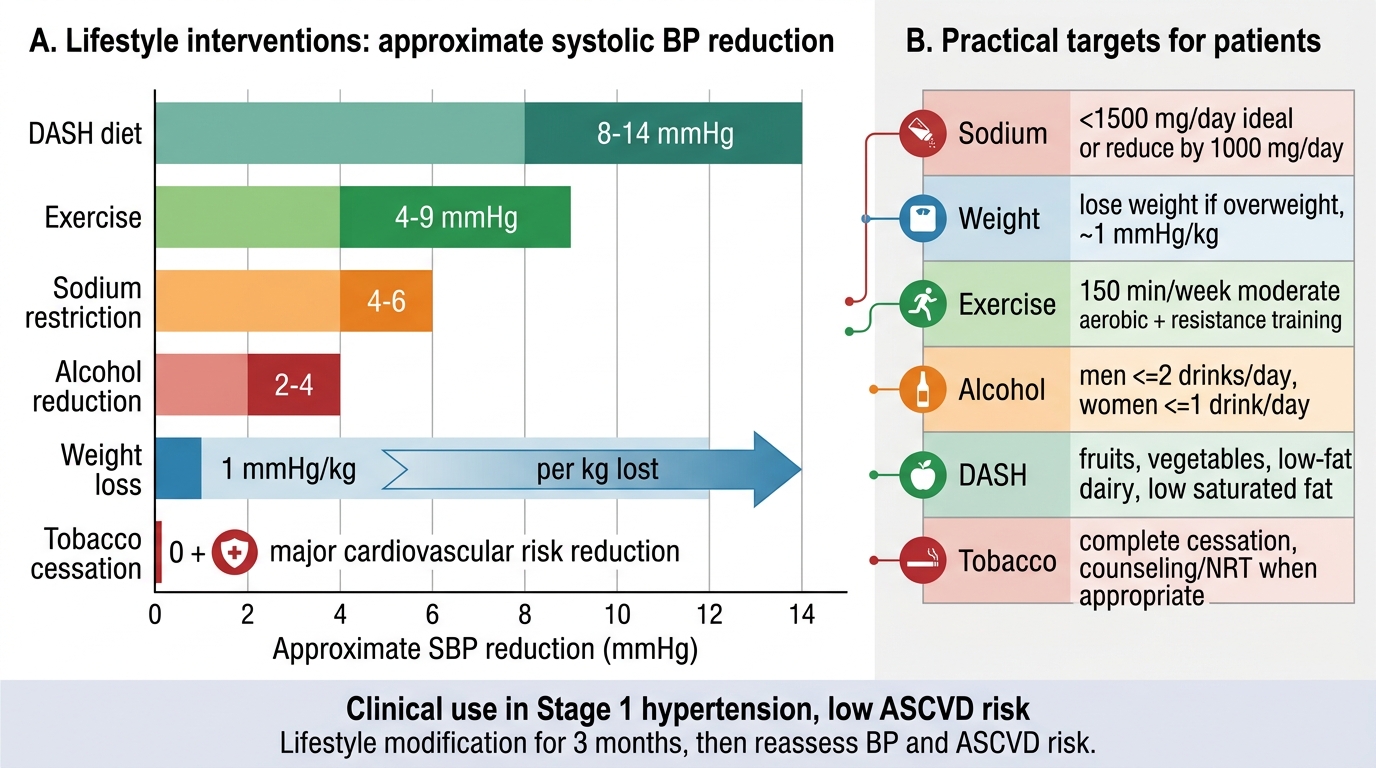
Lifestyle Modification Targets for Hypertension
SELF-CHECK
A 44-year-old man has Stage 1 hypertension by ACC/AHA 2017 (BP 136/86 mmHg), no diabetes, no CKD, no established CVD. His 10-year ASCVD risk is 6%. Which management approach is most appropriate at this visit?
A. Start an ACE inhibitor immediately, as all hypertension requires drug therapy
B. Recommend lifestyle modification for 3 months, then reassess BP and ASCVD risk
C. Start two antihypertensive agents in combination, as monotherapy is insufficient
D. Recommend only sodium restriction as the sole lifestyle modification needed
Reveal Answer
Answer: B. Recommend lifestyle modification for 3 months, then reassess BP and ASCVD risk
Under ACC/AHA 2017, Stage 1 hypertension (130-139/80-89 mmHg) with ASCVD risk <10% and no compelling indications (CVD, diabetes, CKD, HF) warrants lifestyle modification for 3 months before initiating drug therapy. This patient's risk is 6% (<10%), meeting the criteria for a lifestyle-first trial. Immediate drug initiation is reserved for Stage 1 HTN with ASCVD risk ≥10% or high-risk conditions, and for all Stage 2 HTN (≥140/≥90 mmHg). Under JNC 7 / Indian guidelines, a BP of 136/86 mmHg does not even meet the hypertension threshold (140/90), further supporting lifestyle modification only at this stage. Combination therapy is for Stage 2 or BP ≥160/100 mmHg. A single lifestyle modification is inadequate — all applicable components should be addressed.
Pharmacological Treatment: Drug Classes, Compelling Indications, and Combination Principles
Pharmacological treatment of hypertension is highly effective, and the choice of drug class is one of the most individualisable decisions in all of medicine — because the same BP reduction can be achieved by several different drug classes, but their additional effects on target organs, comorbidities, and metabolic parameters vary substantially. This section builds the framework for rational drug selection by covering the four major first-line classes, their mechanisms, their specific indications (including compelling indications where evidence of outcome benefit beyond BP lowering has been proven), and the principles of combination therapy.
The four first-line antihypertensive drug classes (A, C, D, B):
A — ACE Inhibitors and ARBs (RAAS blockers):
ACE inhibitors (enalapril, ramipril, lisinopril, perindopril) block the conversion of angiotensin I to angiotensin II. ARBs (losartan, telmisartan, olmesartan, valsartan) block the AT1 receptor. Both classes lower BP by reducing angiotensin II-mediated vasoconstriction and aldosterone-mediated sodium retention. ADDITIONAL organ-protective effects beyond BP lowering: (a) nephroprotection — reduce proteinuria and slow progression of diabetic nephropathy and hypertensive nephrosclerosis by dilating the efferent arteriole, lowering intraglomerular pressure; (b) cardiac remodelling reversal — reduce LVH regression, reduce HFrEF mortality (proven in CONSENSUS, SOLVD trials); (c) post-MI benefit — ramipril (HOPE trial) and perindopril (EUROPA trial) reduce cardiovascular events in patients with established vascular disease. Compelling indications: diabetes with microalbuminuria or proteinuria, CKD with proteinuria, HFrEF (LVEF ≤40%), post-MI, high cardiovascular risk. Contraindications: bilateral renal artery stenosis (acute kidney injury risk), pregnancy (teratogenic — causes renal dysgenesis and oligohydramnios), prior ACE inhibitor angioedema. Key side effects: ACE inhibitor dry cough (bradykinin accumulation, affects 10–20% of patients; switch to ARB — ARBs do not cause cough as they do not affect bradykinin metabolism); hyperkalemia (monitor K+ especially with CKD, diabetes, or potassium-sparing diuretic); first-dose hypotension (start low, warn patient).
C — Calcium Channel Blockers (CCBs):
Two subclasses: dihydropyridines (amlodipine, nifedipine, felodipine) — primarily vascular (reduce SVR); non-dihydropyridines (verapamil, diltiazem) — primarily cardiac (reduce heart rate and contractility, reduce AVN conduction). Dihydropyridine CCBs (particularly amlodipine) are among the most commonly used first-line agents worldwide. Evidence from ASCOT-BPLA trial: amlodipine-based regimen reduced cardiovascular events more than atenolol-based regimen despite similar BP lowering — suggesting outcome benefits beyond BP. Compelling indications: elderly patients (well tolerated), isolated systolic hypertension, angina pectoris (dihydropyridines provide coronary vasodilation), Raynaud phenomenon, in Black patients (who show relatively less response to ACE inhibitors alone due to low-renin status). Verapamil/diltiazem: useful when AF rate control is also needed. Contraindications: verapamil and diltiazem are contraindicated with HFrEF (negative inotropy worsens systolic dysfunction) and should not be combined with beta-blockers (AV nodal block risk). Key side effects: peripheral ankle oedema (arteriolar dilation with preserved venous tone → dependent fluid accumulation; responds to ACE inhibitor co-prescription); flushing, headache, palpitations (dihydropyridines); constipation (verapamil).
D — Thiazide and Thiazide-Like Diuretics:
Thiazides (hydrochlorothiazide, HCTZ) inhibit the Na-Cl cotransporter (NCC) in the distal convoluted tubule; their BP-lowering effect in the long term is primarily through vascular mechanisms (after initial volume reduction, long-term SVR falls through mechanisms including K-channel activation). Thiazide-LIKE diuretics (indapamide, chlorthalidone) have longer half-lives and superior cardiovascular outcome evidence compared to HCTZ in meta-analyses — chlorthalidone is the preferred thiazide-type for outcome evidence (ALLHAT trial). Compelling indications: elderly, isolated systolic hypertension, prevention of recurrent calcium-containing kidney stones (thiazides reduce urinary calcium excretion), Black patients (volume-dependent hypertension is common; good response to thiazides + CCBs). Contraindications: gout (thiazides raise uric acid); use cautiously in diabetes (mild glucose intolerance effect); avoid in patients with severe hyponatraemia history (thiazides aggravate hyponatraemia in susceptible patients, especially elderly women). Key side effects: hypokalaemia (potassium wasting; supplement K+ or add potassium-sparing agent if needed); hyperuricaemia/gout (use losartan — uricosuric effect); glucose intolerance; hyponatraemia; dyslipidaemia (mild, short-term).
B — Beta-Blockers:
Beta-1 selective (bisoprolol, metoprolol, atenolol, nebivolol) or non-selective (propranolol, carvedilol). Reduce heart rate, cardiac output, and renin release. Less effective than A, C, D for primary BP lowering outcomes in uncomplicated hypertension — large meta-analyses (particularly the LIFE study comparing atenolol vs losartan) showed beta-blockers (specifically atenolol) to be inferior for stroke prevention. Therefore, beta-blockers are NOT first-line for uncomplicated hypertension in current guidelines. Compelling indications: angina (reduce myocardial O2 demand), HFrEF (carvedilol, bisoprolol, metoprolol succinate — proven mortality benefit), post-MI (reduce infarct extension and arrhythmia), AF rate control, essential tremor, hyperthyroidism (control symptoms), anxiety-related hypertension. Contraindications: asthma and COPD (non-selective — may cause bronchospasm; use with caution even cardioselective), severe bradycardia or heart block (without pacemaker), acute decompensated HF (initiate only when stable). Special agent note: Nebivolol has nitric oxide-mediated vasodilatory properties in addition to beta-1 blockade — it causes less erectile dysfunction than other beta-blockers and has a more neutral metabolic profile.
Combination therapy principles:
The majority of hypertensive patients require two or more drugs to achieve BP targets. Starting combination therapy (fixed-dose combinations preferred for adherence) is recommended for all Stage 2 HTN (≥140/90 by JNC7 or ≥140/90 by ACC/AHA Stage 2) and for patients with Stage 1 HTN who are high/very-high risk. The preferred first-line combination is A (ACE/ARB) + C (CCB) — shown in ACCOMPLISH trial (amlodipine + benazepril) to be superior to ACE/ARB + diuretic for cardiovascular outcomes. A + D (ACE/ARB + thiazide) is the standard alternative combination. Avoid A + A (ACE inhibitor + ARB) — the ONTARGET trial showed increased renal adverse effects without additional cardiovascular benefit. B + D (beta-blocker + thiazide) is considered metabolically unfavourable (additive glucose intolerance and dyslipidaemia) — avoid unless both have compelling individual indications.
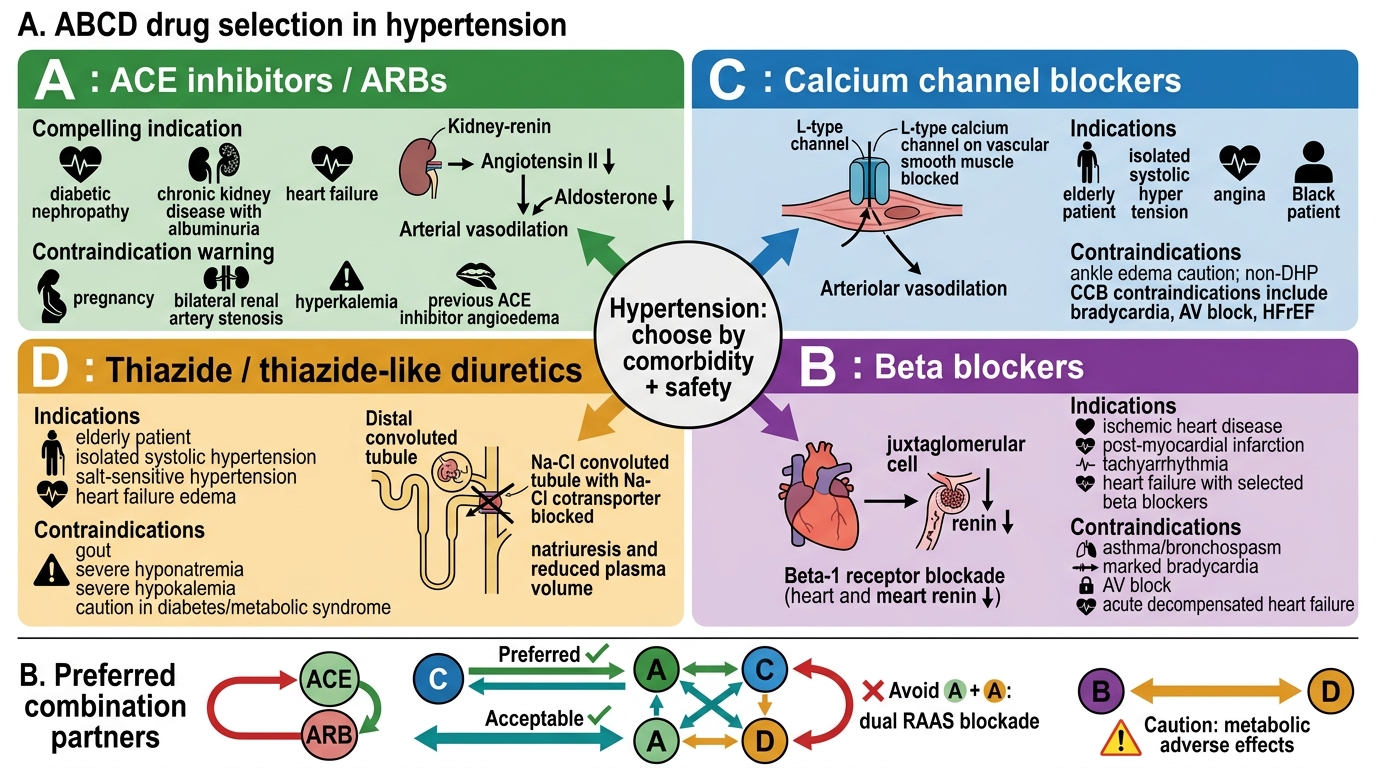
ABCD Drug Selection in Hypertension