Page 9 of 15
IM8.{13-15,17-19} | Hypertension Management and Follow-up — SDL Guide (Part 2)
Hypertensive Emergency: Recognition, Prioritisation, and Management
The recognition and management of hypertensive emergency is a critical clinical skill that must be executed correctly under time pressure. This section builds directly on the urgency/emergency distinction covered in the foundations module and translates that conceptual framework into a management protocol. Competency IM8.14 requires that the student can recognise, prioritise, and manage hypertensive emergencies — a KH-level competency that must be translated into clinical action.
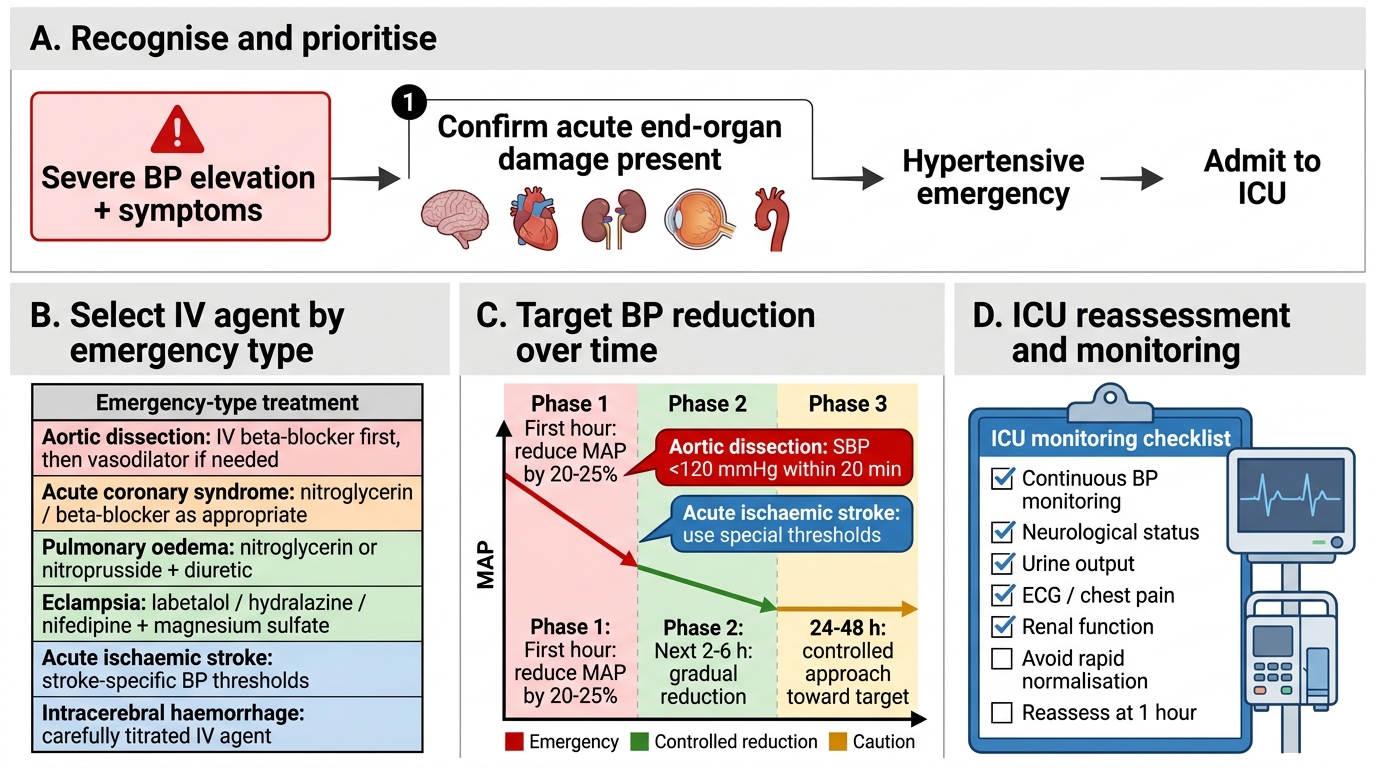
The overarching principle of managing hypertensive emergency is controlled, partial, and graded reduction of BP — not normalisation. The reason for this seemingly counterintuitive approach is cerebrovascular autoregulation: in patients with chronically elevated BP, the autoregulatory curve shifts rightward, meaning the brain's ability to maintain constant cerebral blood flow operates at higher perfusion pressures than in normotensive individuals. If BP is dropped rapidly to 'normal' levels, cerebral perfusion can fall catastrophically — even though the 'normal' BP is what we would target in a normotensive patient — resulting in cerebral ischaemia or infarction.
Standard BP reduction targets in hypertensive emergency:
- Phase 1 (first hour): Reduce MAP by no more than 20–25%. Do not target a specific BP number; target a percentage reduction of the MAP. This prevents cerebrovascular and renal hypoperfusion.
- Phase 2 (next 2–6 hours): Reduce to approximately 160/100–110 mmHg.
- Phase 3 (next 24–48 hours): Gradually reduce toward the patient's individual BP target as guided by tolerance and organ function.
Exception — aortic dissection: This is the one hypertensive emergency where rapid reduction IS required. Target SBP <120 mmHg within 20 minutes because continued high BP drives dissection propagation. Use IV labetalol (combined alpha-1 + beta block reduces both BP and heart rate/dP/dt which is critical for aortic wall stress) or IV esmolol + nitroprusside.
Exception — acute ischaemic stroke: BP management in acute ischaemic stroke is nuanced and critical. In patients NOT eligible for thrombolysis: BP should generally NOT be lowered acutely unless BP is ≥220/120 mmHg — the penumbral zone depends on elevated BP for collateral perfusion. In patients eligible for IV tPA thrombolysis: BP must be brought below 185/110 mmHg before tPA administration (using IV labetalol or nicardipine), and maintained below 180/105 mmHg for 24 hours after tPA. In haemorrhagic stroke: target SBP <140 mmHg within 1 hour (INTERACT2 trial) using IV labetalol or nicardipine.
Intravenous antihypertensive agents for emergencies — selection by clinical context:
| Emergency Type | Preferred IV Agent(s) | Comments |
|---|---|---|
| Hypertensive encephalopathy / PRES | Nicardipine, labetalol | Smooth titration; avoid nitroprusside (ICP concern) |
| Acute pulmonary oedema | Nitroglycerin (IV) + furosemide | Venodilation reduces preload; loop diuretic for volume |
| Acute coronary syndrome (ACS) | Nitroglycerin, labetalol | Nitroglycerin for coronary vasodilation; avoid CCBs (reflex tachycardia with dihydropyridines can worsen ischaemia) |
| Aortic dissection | Labetalol OR esmolol + nitroprusside | Heart rate AND BP control; target SBP <120 mmHg within 20 min; NEVER start beta-blocker without first blocking heart rate |
| Acute ischaemic stroke (pre-tPA) | Labetalol, nicardipine | Target BP <185/110 before tPA; gradual, avoid hypotension |
| Haemorrhagic stroke | Labetalol, nicardipine | Target SBP <140 mmHg within 1 hour (INTERACT2) |
| Pre-eclampsia / eclampsia | IV hydralazine, IV labetalol; oral nifedipine | Avoid ACE inhibitors, ARBs (teratogenic); mag sulphate for seizures |
| Phaeochromocytoma crisis | Phentolamine (IV alpha-blocker) or nicardipine | Alpha-blockade FIRST; never beta-blocker alone |
| Malignant hypertension with AKI | Labetalol, nicardipine | Controlled BP reduction; avoid precipitous drop that worsens renal perfusion |
Pharmacology of key IV agents:
- Labetalol: combined alpha-1 and non-selective beta-blocker (alpha:beta ratio 1:7 IV); onset 5–10 min, duration 3–6 hours; can be given as IV boluses (20 mg every 10 min, max 300 mg) or infusion (1–2 mg/min); safe in aortic dissection, encephalopathy, eclampsia; avoid in severe HFrEF, acute bronchospasm, severe bradycardia.
- Nicardipine: dihydropyridine CCB; IV infusion only (5–15 mg/hr, titrated); smooth, predictable, titratable; onset 5–10 min; preferred in encephalopathy, perioperative hypertension, ischaemic stroke; side effects: reflex tachycardia, headache.
- Sodium nitroprusside: direct arteriovenous dilator (both arteriolar and venous); immediate onset (<1 min), short duration (1–2 min); very potent and titratable; monitor for cyanide/thiocyanate toxicity in renal failure or prolonged infusion (>24–48 hours); must be administered in ICU with intra-arterial BP monitoring; protects from light.
- Nitroglycerin (IV): primarily venodilator → reduces preload; modest arteriolar dilation at high doses; first choice in ACS with hypertension and acute pulmonary oedema; tolerance develops with continuous use after 24 hours.
- Hydralazine (IV): direct arteriolar vasodilator; used in pre-eclampsia; unpredictable dose-response; reflex tachycardia; avoid in aortic dissection.
- Furosemide (IV): loop diuretic; indicated when volume overload and pulmonary oedema are components of the emergency; alone is insufficient to control hypertensive emergency BP.
Monitoring in hypertensive emergency:
All patients require: continuous BP monitoring (intra-arterial line if available, or 15-minute automatic cuff in less critical cases), ICU or high-dependency unit admission, continuous cardiac monitoring (ECG), urine output (urinary catheter), 2-hourly neurological assessment, repeat urea, creatinine, and electrolytes at 2–4 hours, and target organ reassessment (repeat fundoscopy if papilloedema, repeat ECG for evolving changes).
Hypertensive Emergency Management Algorithm
SELF-CHECK
A 62-year-old man presents with hypertensive emergency (BP 204/128 mmHg). His MAP at presentation is 153 mmHg. After 1 hour of IV nicardipine, what is the upper limit of MAP reduction that is generally appropriate (in mmHg)?
A. MAP should be reduced to 80 mmHg (normal MAP) as quickly as possible
B. MAP should be reduced by a maximum of 20–25%, i.e., to approximately 115–122 mmHg
C. MAP should be reduced by exactly 30 mmHg, to 123 mmHg
D. MAP should be reduced until the patient's BP is below 140/90 mmHg
Reveal Answer
Answer: B. MAP should be reduced by a maximum of 20–25%, i.e., to approximately 115–122 mmHg
The standard management principle for hypertensive emergency (except aortic dissection) is to reduce MAP by no more than 20–25% in the first hour. Starting MAP is 153 mmHg. 20% of 153 = 30.6 mmHg reduction → target MAP approximately 122 mmHg (153 - 30.6). 25% reduction = 38.25 mmHg reduction → target MAP approximately 115 mmHg (153 - 38.25). So the acceptable range is MAP 115–122 mmHg at 1 hour. Reducing to normal MAP (~80 mmHg) risks cerebral and renal ischaemia because the autoregulatory curve has reset at higher pressures. A fixed 30 mmHg reduction is not the standard; percentage reduction is the correct metric. Targeting <140/90 mmHg is appropriate long-term, not at 1 hour.
Patient Counselling, Adherence, Quality of Life, and Specialist Referral
Effective hypertension management extends far beyond writing a prescription — it requires ongoing communication, shared decision-making, and an understanding of how hypertension and its treatment affect a patient's daily life. Competencies IM8.15 (lifestyle communication), IM8.17 (counselling and incorporating patient preferences), IM8.18 (impact on quality of life), and IM8.19 (specialist referral) are all SH- or KH-level skills that require practice in clinical communication. The content here provides the conceptual framework; clinical skills training sessions and supervised outpatient encounters are required to operationalise them.
Adherence — the central challenge of hypertension management:
Hypertension is asymptomatic in most patients. The paradox of treating a condition the patient cannot feel, with medications that have side effects the patient can feel, is the fundamental adherence challenge. In India, non-adherence to antihypertensive therapy accounts for the majority of uncontrolled hypertension. Key determinants of non-adherence include: perceived lack of symptoms ('I feel fine, so the tablet must not be needed'), fear of lifelong dependency, cost of medications, tablet burden (pill fatigue), side effects (especially ACE inhibitor cough, beta-blocker fatigue/erectile dysfunction, CCB ankle swelling), lack of understanding of why treatment is needed, and healthcare access issues (long queues, irregular supply).
Strategies to improve adherence:
- Explicitly explain that hypertension is almost always asymptomatic — the risk is silent organ damage, not symptoms
- Use simple, jargon-free language: 'The pressure in your blood vessels is too high. Even though you don't feel it, it is quietly damaging your heart, kidneys, and brain every day. The tablet reduces that pressure and protects those organs.'
- Address the 'lifelong treatment' concern honestly: 'For most people, hypertension requires long-term medication. Stopping the tablet will bring the pressure back up. But lifestyle changes can sometimes reduce the dose needed.'
- Prescribe once-daily formulations and fixed-dose combinations wherever possible to reduce pill burden
- Use lowest effective doses to minimise side effects
- Actively ask about side effects at every follow-up — do not assume the absence of complaint means absence of side effects
- Involve the patient's family (especially for elderly patients where family support improves adherence)
Incorporating patient preferences (IM8.17):
Shared decision-making is a core principle of modern evidence-based medicine. For hypertension, this means: involving the patient in setting BP targets (especially in the elderly where lower targets must be weighed against fall risk); discussing the relative merits of different drug classes (e.g., patient with erectile dysfunction should receive ACE/ARB or CCB rather than beta-blocker); respecting cultural and religious considerations (e.g., gelatine-coated tablets may not be acceptable); discussing cost and availability of generic vs branded formulations (in India, ASHA-distributed generic antihypertensives under the Jan Aushadhi programme provide access at reduced cost); and respecting the patient's right to decline pharmacological therapy and choose lifestyle-only management when guidelines permit (Stage 1 HTN, low risk).
Quality of life and psychosocial impact of hypertension (IM8.18):
Hypertension has both direct and indirect impacts on quality of life (QoL):
- Direct disease impacts: complications of uncontrolled hypertension (stroke causing disability, MI, CKD requiring dialysis) cause profound QoL impairment. The fear of these outcomes also contributes to anxiety in diagnosed patients.
- Drug side effects: fatigue (beta-blockers), dry cough (ACE inhibitors), ankle swelling (CCBs), sexual dysfunction (beta-blockers, thiazides), frequent urination (diuretics) — each impacts wellbeing and work capacity.
- Occupational and economic impact: hypertension is a disqualifying or monitoring-required condition for certain high-stakes occupations (commercial vehicle drivers, pilots, armed forces). Shift workers have higher hypertension prevalence. Sustained BP control may be required for occupational clearance.
- Family dynamics: chronic medication taking, dietary modification, and restriction of alcohol can affect family eating habits and social dynamics. Involving the family in education sessions improves both adherence and lifestyle change.
- Mental health: newly diagnosed hypertension increases anxiety ('I now have a chronic disease'). Depression is more common in hypertensive patients — bidirectional relationship where depression impairs adherence and hypertension may impair mood through vascular mechanisms. Screening for depression (PHQ-2) and anxiety is appropriate at diagnosis and follow-up visits.
Resistant hypertension — definition and management:
Resistant hypertension is defined as office BP consistently above goal despite the use of ≥3 antihypertensive agents at optimal doses, including a diuretic. The evaluation should first exclude: (a) pseudoresistance — inaccurate measurement (white-coat effect, inadequate cuff size), medication non-adherence, inadequate drug doses; and (b) drug-induced causes (NSAIDs, OCP, decongestants, steroids). After excluding these, all patients with truly resistant hypertension should be systematically evaluated for secondary causes (primary aldosteronism, sleep apnoea, renovascular disease, phaeochromocytoma, Cushing). Aldosterone antagonists (spironolactone 25–50 mg/day) as a fourth agent have the best evidence for treating resistant hypertension — the PATHWAY-2 trial showed spironolactone to be significantly more effective than bisoprolol or doxazosin as fourth-line therapy.
Specialist referral criteria (IM8.19):
Most hypertension is managed in primary or general medicine settings. Specialist referral (cardiologist, nephrologist, endocrinologist, or hypertension specialist) is indicated when:
- Suspected or confirmed secondary hypertension (primary aldosteronism → endocrinologist, renovascular → vascular/interventional, phaeochromocytoma → endocrine/surgical, Cushing → endocrinologist, coarctation → cardiology/vascular surgery)
- Resistant hypertension (uncontrolled on ≥3 optimally dosed agents) after excluding pseudoresistance
- Hypertensive emergency (admit to hospital/ICU; may require specialist support)
- Hypertension in pregnancy (obstetric and medicine shared care)
- CKD with heavy proteinuria (eGFR <30 mL/min/1.73m² or ACR >300 mg/g) — nephrology
- Hypertension with significant cardiac target organ damage (HFrEF, significant LVH, AF) — cardiology
- Difficult-to-treat hypertension with multiple comorbidities requiring complex drug management
- Hypertension in children or adolescents (paediatric cardiology / nephrology)
- Need for ambulatory BP monitoring interpretation if not available at primary care level
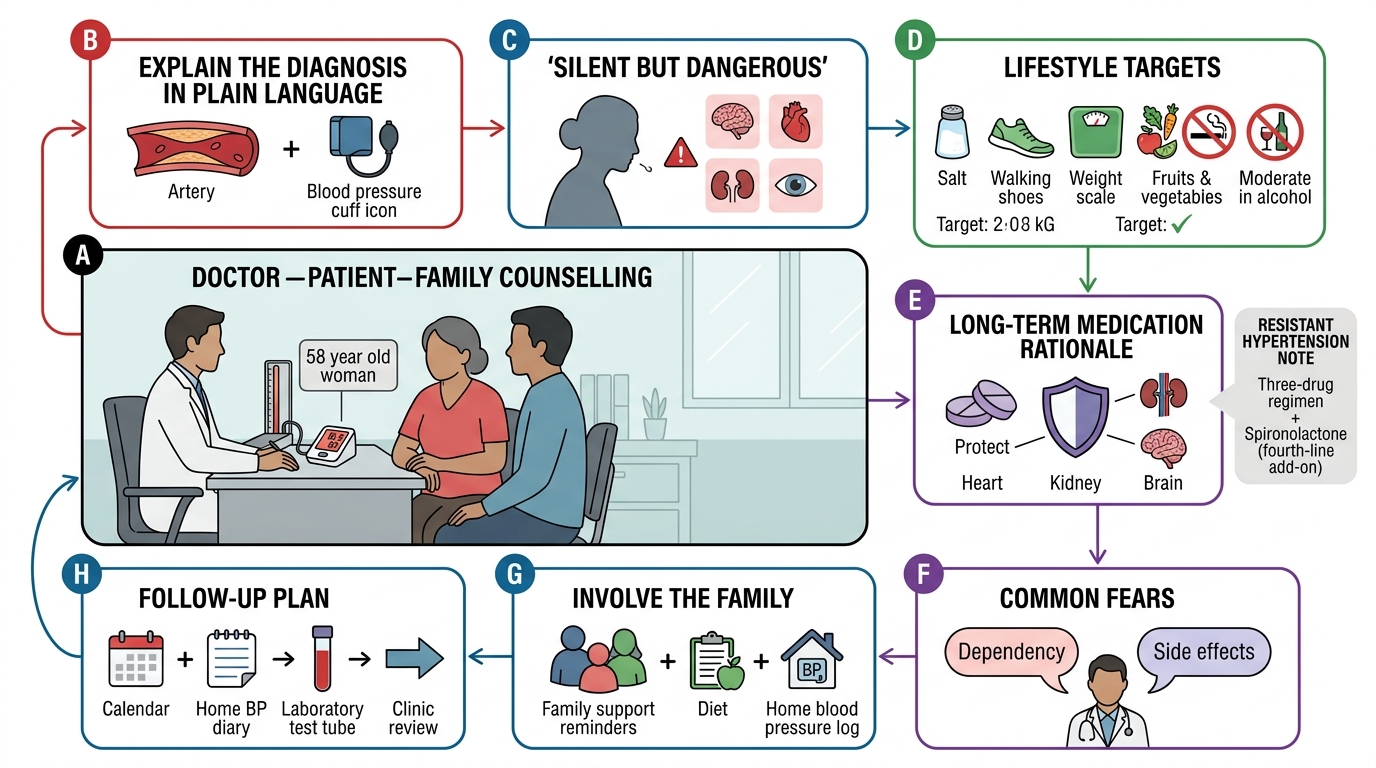
Patient Counselling Framework for Hypertension
SELF-CHECK
A 58-year-old woman is on lisinopril 10 mg, amlodipine 10 mg, and indapamide 2.5 mg, all at maximum doses, for 6 months. Her BP remains 162/98 mmHg. She is adherent (pill count confirmed). She has no cushingoid features, no abdominal bruit, no episodic symptoms. Her serum K+ is 3.7 mEq/L. What is the most appropriate next step in management?
A. Add a beta-blocker (bisoprolol) as the fourth agent
B. Add spironolactone 25–50 mg as the fourth agent
C. Increase lisinopril to 20 mg (double dose above maximum)
D. Refer immediately for renal artery stenting
Reveal Answer
Answer: B. Add spironolactone 25–50 mg as the fourth agent
This patient meets the definition of resistant hypertension (BP above goal on ≥3 optimally dosed agents including a diuretic, with confirmed adherence). Pseudoresistance and common secondary causes are not suggested by the clinical picture (no cushingoid features, no bruit, no episodic symptoms, normal K+). The PATHWAY-2 trial demonstrated that spironolactone (aldosterone antagonist) is the most effective fourth agent for resistant hypertension, significantly superior to bisoprolol or doxazosin. Primary aldosteronism is common and often biochemically occult (normokalemic) — spironolactone treats volume-dependent resistant hypertension regardless of whether aldosterone is formally elevated. Beta-blockers are less effective as fourth-line agents and are not the guideline-recommended choice. Doubling lisinopril beyond licensed maximum is not appropriate and increases adverse effect risk. Renal artery stenting is not indicated without evidence of renovascular disease.
Self-Assessment: Applying the Complete Management Framework
The following scenarios integrate the full management arc: treatment decision, lifestyle advice, drug selection, emergency management, and counselling. Work through each before reading the analysis. These exercises consolidate competencies IM8.13–IM8.19.
Scenario A — Treatment Planning (IM8.13):
Ajay, 52 years old, has BP 146/92 mmHg on three visits, type 2 diabetes with HbA1c 7.2%, eGFR 64 mL/min/1.73m² (CKD stage G2), and urine ACR of 85 mg/g (microalbuminuria). He smokes 10 cigarettes/day. He is not on any antihypertensive. What is the target BP and preferred first-line drug class?
Analysis: Ajay has high-risk hypertension (diabetes + microalbuminuria + Stage G2 CKD). Under ACC/AHA 2017, the target BP is <130/80 mmHg (high-risk category). Under IGH-IV 2019, target is <130/80 mmHg for hypertension + diabetes + CKD. Preferred drug class: ACE inhibitor or ARB — the only class with proven nephroprotective benefit (reducing proteinuria, slowing CKD progression) beyond BP lowering. Start ramipril or perindopril (ACE inhibitor) or telmisartan (ARB). Monitor creatinine and K+ in 2 weeks after initiation. Additional actions: Smoking cessation counselling (mandatory); target HbA1c <7.0%; start statin (LDL >70 mg/dL in very-high-risk atherosclerotic CVD equivalent CKD + diabetes + HTN).
Scenario B — Emergency Management (IM8.14):
Preethi, 66 years old, presents with acute-onset severe headache, vomiting, and confusion. BP 218/136 mmHg. CT brain (plain): normal, no haemorrhage, no infarct. Fundoscopy: grade IV changes (papilloedema). Troponin: normal. Creatinine: 2.4 mg/dL (baseline unknown). What is the diagnosis, and what is the BP target at 1 hour?
Analysis: Hypertensive encephalopathy / PRES — severe hypertension with acute neurological dysfunction (confusion) and papilloedema, in the absence of haemorrhagic or ischaemic stroke on CT. This is a hypertensive emergency. MAP at presentation = (218 + 2×136)/3 = 163 mmHg. Target at 1 hour: reduce MAP by 20–25% → target MAP 122–130 mmHg → approximate target BP 155–165/95–105 mmHg. Use IV nicardipine (infusion, titratable) or IV labetalol. Admit to ICU, intra-arterial BP monitoring, urinary catheter for urine output, repeat neurological assessment every 30–60 minutes. If CT changes or MRI FLAIR shows posterior white matter changes, confirms PRES.
Scenario C — Counselling and Adherence (IM8.15, IM8.17, IM8.18):
Vijay, 45 years old, returns to clinic on ramipril 5 mg + amlodipine 5 mg. His BP today is 154/96 mmHg (unchanged from 3 months ago). He admits he often forgets his evening tablet and has continued his habit of daily salted snacks and 3 units of alcohol/day. He says he doesn't understand why he needs tablets when he feels perfectly healthy. Outline a brief structured counselling approach.
Analysis: The counselling approach should address four elements: (1) Explanation of silent risk — explain that hypertension damages blood vessels slowly and silently; by the time symptoms appear (stroke, heart attack), the damage is already done. (2) Linking behaviour to BP — specifically link his salted snacks (sodium excess) and alcohol (3 units/day — above the 2-unit limit) to his persistent high BP. (3) Simplifying the regimen — switch to a once-daily fixed-dose combination (e.g., ramipril + amlodipine fixed combination) to reduce missed doses. (4) Follow-up commitment — set a 4-week return appointment with a specific BP target to review: if he reduces sodium and alcohol and takes tablets daily, BP should fall by 5–10 mmHg. Involve his spouse or a family member in the counselling if possible.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
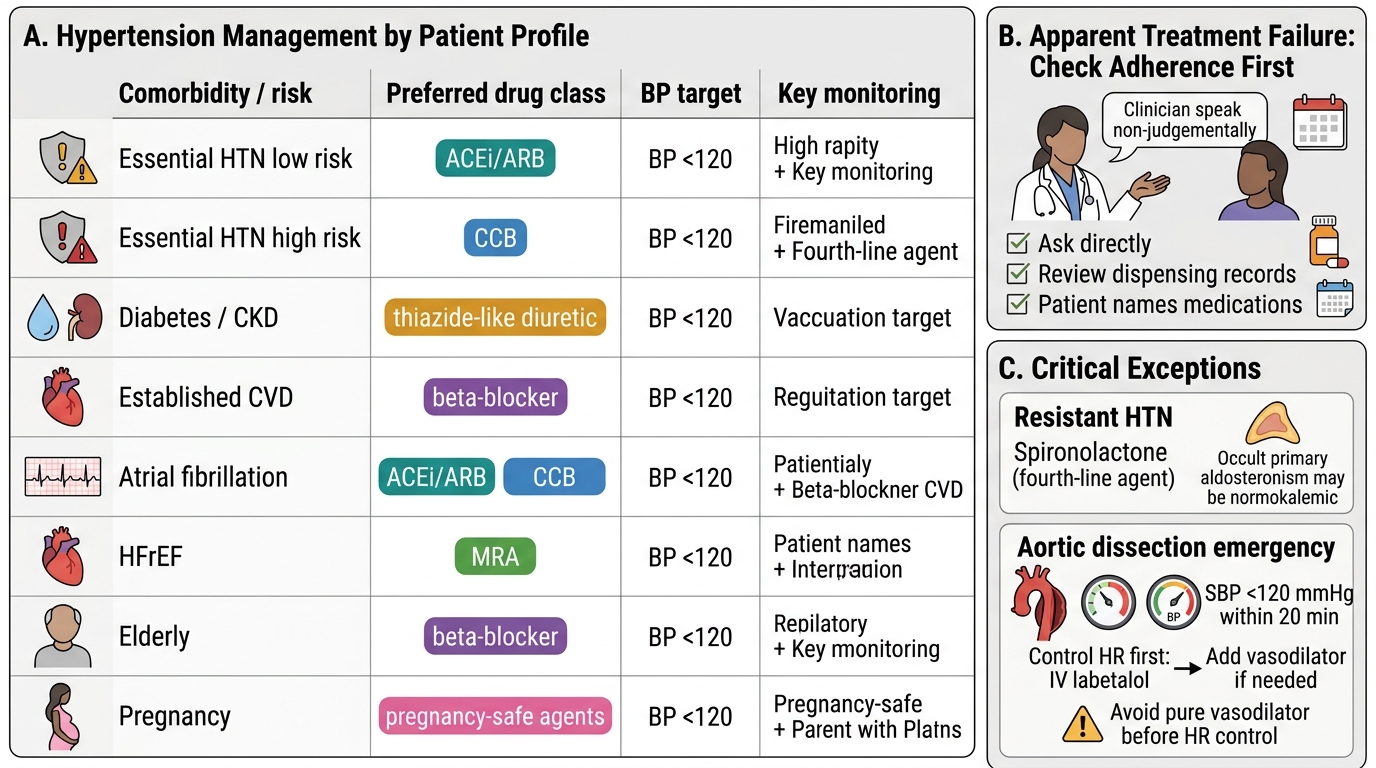
Hypertension Management by Patient Profile
CLINICAL PEARL
The most common cause of apparent treatment failure in hypertension is patient non-adherence — before escalating therapy or investigating for resistant hypertension, always check adherence by asking the patient directly (non-judgementally: 'Many people find it difficult to remember their tablets every day — has that been a challenge for you?'), reviewing dispensing records, and checking whether the patient can name their medications. The PATHWAY-2 trial finding that spironolactone is the best fourth agent for resistant hypertension is not merely an academic result — it reflects the reality that primary aldosteronism is commonly occult (normokalemic) and underlies a significant proportion of cases labelled 'resistant hypertension'.
For aortic dissection: the BP target is SBP <120 mmHg within 20 minutes — this is the one true hypertensive emergency where faster is better. The combination of IV labetalol (to reduce heart rate and BP simultaneously, lowering dP/dt and aortic wall stress) with or without sodium nitroprusside is standard. Starting a pure vasodilator (nitroprusside alone) without controlling the heart rate first increases dP/dt and can worsen dissection propagation — always control heart rate first (or use labetalol which does both).