Page 4 of 11
SU1.3 | Basic Concepts of Perioperative Care — SDL Guide
Learning Objectives
- Define perioperative care and describe its three phases — preoperative, intraoperative and postoperative — and explain why structured care, not the operation alone, determines surgical outcome (SU1.3).
- Describe the core elements of preoperative assessment, including ASA physical-status grading, preoperative fasting, informed consent, optimisation of comorbidity and prophylaxis (SU1.3).
- Describe the principles of intraoperative safety (the WHO Surgical Safety Checklist, asepsis, normothermia and monitoring) and of postoperative recovery (analgesia, fluids, VTE prophylaxis and early mobilisation), and the place of ERAS pathways (SU1.3).
INSTRUCTIONS
An operation is only one moment in a much longer process. What happens in the days before surgery — how the patient is assessed, optimised, consented and prepared — and in the hours and days afterwards — how pain, fluids, clots and complications are managed — often matters more to the final outcome than the technical steps at the table. This module builds the foundation of perioperative care: a structured, checklist-driven discipline that turns a risky event into a safe, predictable journey. It draws directly on the metabolic response to injury you met earlier, because much of perioperative care is about blunting that response and supporting the patient through it.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients have the same hernia repaired by the same surgeon on the same day. The first arrives starved since the previous midnight, dehydrated and anxious, with an undiagnosed high blood sugar and no record of his blood thinners; nobody confirms which side is to be operated on. The second is assessed in a clinic a week earlier, told to drink clear fluids until two hours before surgery, has his diabetes optimised, signs an informed consent he actually understands, and — moments before the first incision — has the whole team pause to confirm his name, the procedure and the correct side. The operations are identical. The outcomes are not. The difference is everything that surrounds the operation: perioperative care. This module is about that surrounding care, and why it so often decides whether surgery helps or harms.
WHY THIS MATTERS
Perioperative care is the single most reliable lever a surgical team has over outcome, because most surgical harm happens not from the technical operation but from the care around it — wrong-site surgery, aspiration from inadequate fasting, untreated comorbidity, postoperative chest infection, venous thromboembolism, uncontrolled pain that stops a patient breathing deeply or mobilising. Every one of these is preventable by a structured, checklist-driven approach. For a final-year student this is foundational: you will clerk patients for theatre, confirm fasting and consent, recognise the deteriorating postoperative patient, and prescribe analgesia, fluids and thromboprophylaxis from your first week as an intern. It is also examined directly. Get the structure right and surgery becomes a safe, predictable journey; get it wrong and an excellent operation is undone by avoidable peri-procedural harm.
RECALL
Before going further, bring back three things you already know. First, the metabolic response to injury from earlier in this cluster: every operation triggers the ebb-and-flow stress response, and much of perioperative care exists to blunt its harmful excess through warmth, prompt resuscitation, good analgesia and early feeding. Second, basic haemostasis and coagulation physiology from your physiology course — the balance between clotting and bleeding that underlies why immobile surgical patients are at risk of venous thromboembolism and need prophylaxis. Third, the basic principles of asepsis and the chain of infection you met in microbiology, which underpin sterile technique in theatre. Perioperative care is essentially these familiar ideas applied systematically around the moment of operation, so keep them in mind as the structure unfolds.
Why Perioperative Care Decides Surgical Outcome
Perioperative care is the coordinated, structured management of a surgical patient across the whole episode of care — from the decision to operate, through the operation itself, to full recovery and discharge. It deliberately treats surgery not as an isolated technical event but as a journey with three connected phases, each with its own tasks and its own risks. The central insight, repeatedly borne out by large safety studies, is that the majority of preventable surgical harm arises outside the few minutes of cutting and suturing: in inadequate assessment, in failure to optimise a comorbidity, in a missed safety check, in poor postoperative analgesia, fluid management or thromboprophylaxis. A technically flawless operation can still end badly if the surrounding care is poor, and a routine operation becomes far safer when that care is systematic. This is why modern surgery is built on protocols, checklists and bundles rather than individual memory. For the surgeon, mastering perioperative care means thinking ahead — anticipating who will need extra optimisation, which checks must never be skipped, and which postoperative complications to actively watch for — so that risk is engineered out of the pathway before it can cause harm.
Perioperative Pathway: Three Phases of Surgical Care
The Three Phases of the Surgical Journey
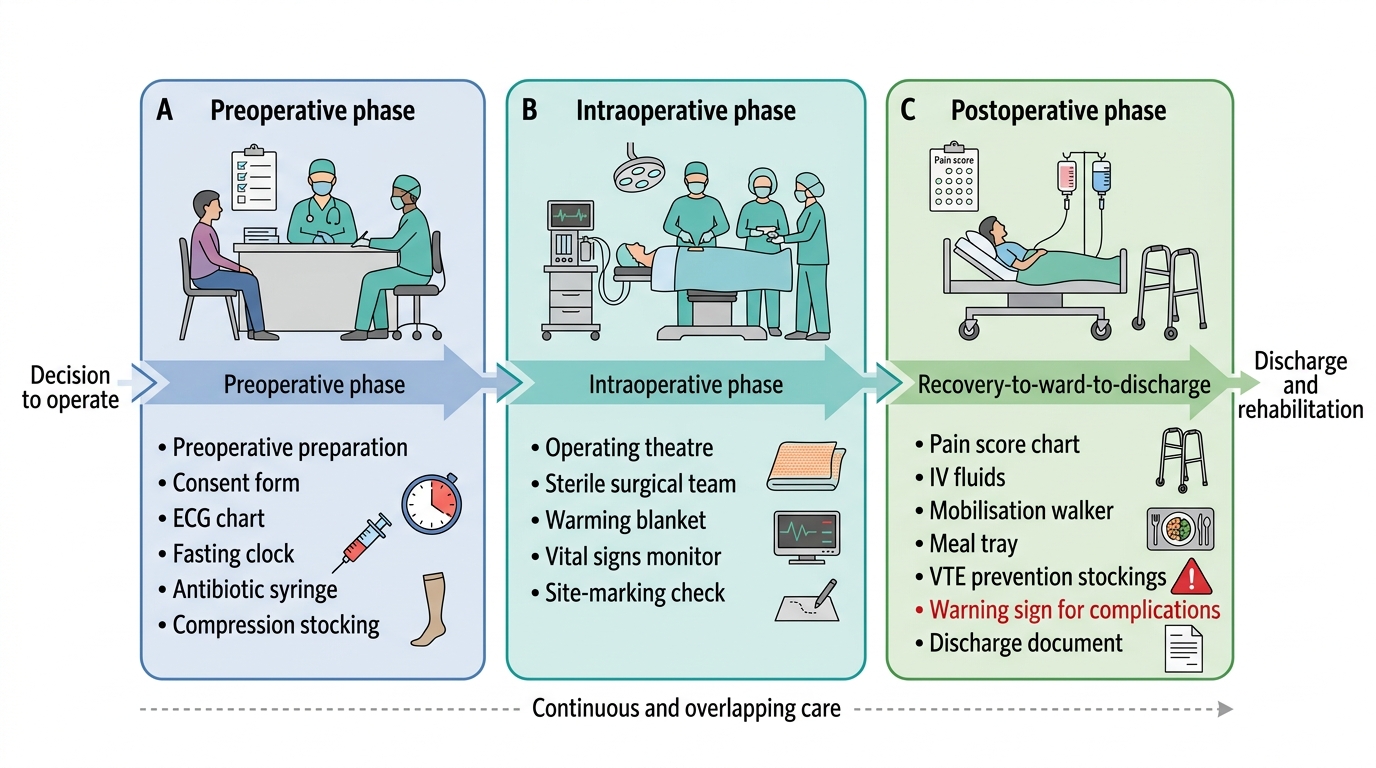
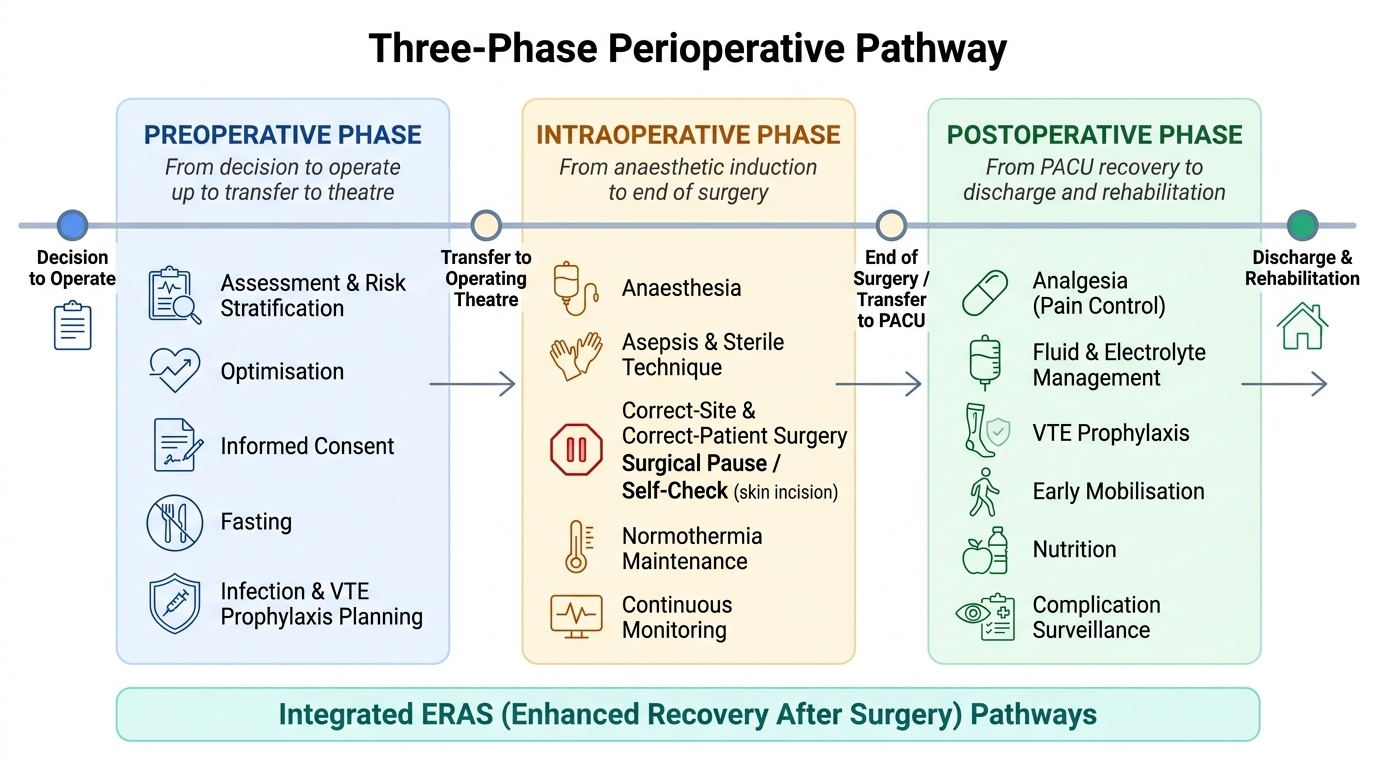
The surgical journey is conventionally divided into three temporal phases, and naming them precisely is the first step to managing each one well. The preoperative phase runs from the decision to operate up to transfer into the operating theatre; its tasks are assessment, risk stratification, optimisation of the patient's medical condition, informed consent, appropriate fasting, and prophylaxis against infection and clots. The intraoperative phase spans the time the patient is in the operating theatre, from anaesthetic induction to the end of surgery; its concerns are anaesthesia, sterile technique, correct-site and correct-patient surgery, maintenance of normothermia, and continuous physiological monitoring. The postoperative phase begins at the end of the operation and continues through immediate recovery in the post-anaesthesia care unit and onward through the ward stay to discharge and rehabilitation; its tasks are pain control, fluid and electrolyte management, prevention of venous thromboembolism, early mobilisation, nutrition, and vigilant surveillance for complications. These phases are continuous and overlapping rather than sealed compartments — a fasting decision made preoperatively affects intraoperative safety, and good intraoperative warming and analgesia shape postoperative recovery — which is exactly why integrated ERAS (Enhanced Recovery After Surgery) bundles span all three.
Provided image
- Preoperative: assessment, risk stratification, optimisation, consent, fasting, infection/VTE prophylaxis planning.
- Intraoperative: anaesthesia, asepsis, correct-site/correct-patient surgery, normothermia, monitoring.
- Postoperative: analgesia, fluids, VTE prophylaxis, early mobilisation, nutrition, complication surveillance.
SELF-CHECK
A surgical team pauses immediately before skin incision to confirm the patient's identity, the planned procedure and the correct operative site. To which phase of perioperative care does this safety step belong?
A. The preoperative phase
B. The intraoperative phase
C. The postoperative phase
D. The convalescent phase
Reveal Answer
Answer: B. The intraoperative phase
The pause before skin incision — the Time-Out of the WHO Surgical Safety Checklist — occurs in the operating theatre, so it is part of the intraoperative phase. Assessment and consent are preoperative; analgesia, fluids and mobilisation are postoperative.
Preoperative Assessment, Risk and Optimisation
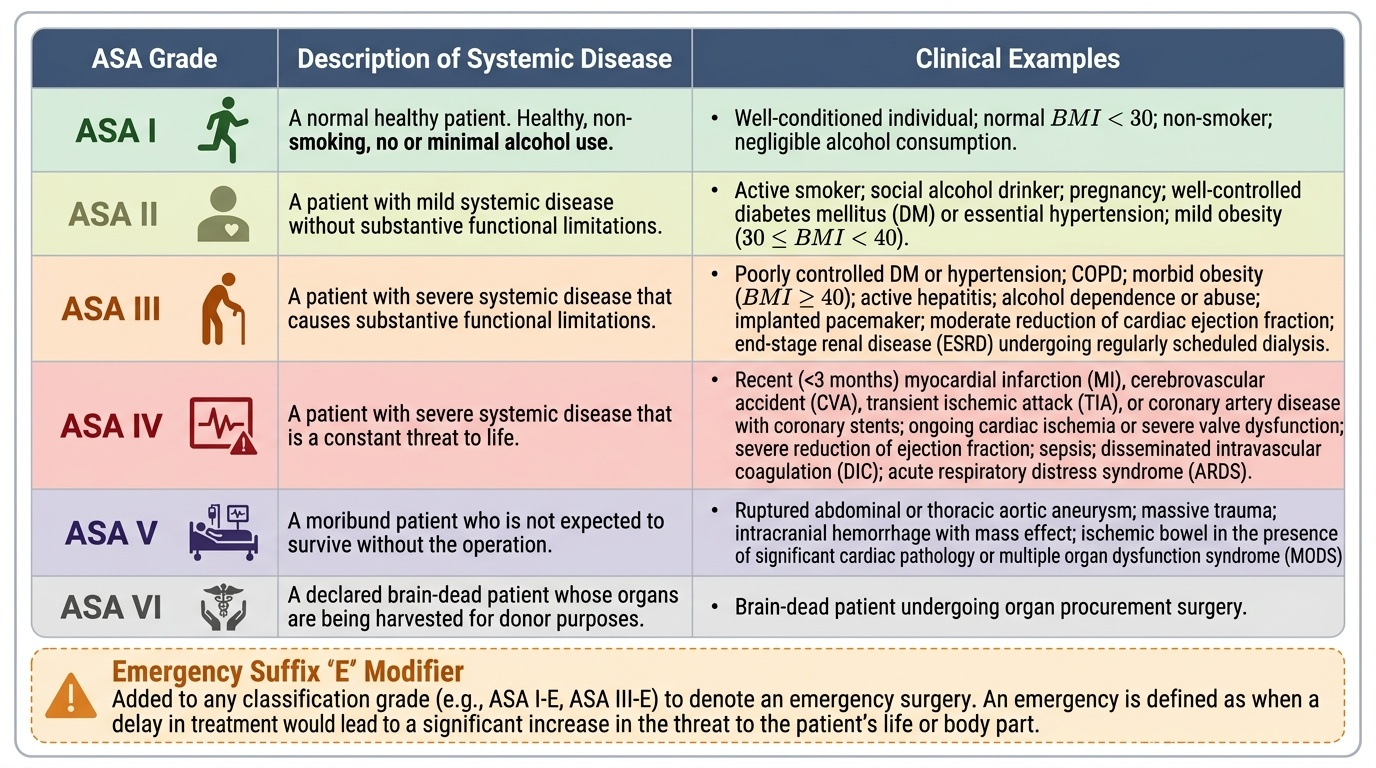
Good surgery begins long before the incision, with a structured preoperative assessment whose purpose is to identify and reduce risk. The cornerstone of risk communication is the ASA physical status classification, which grades the patient from I (a normal healthy patient) through VI (a brain-dead organ donor), with an E suffix added for emergencies. It is essential to understand what this scale does and does not measure: ASA grades the patient's systemic disease, not the difficulty or magnitude of the proposed operation. It is also a different tool from the Mallampati classification (I–IV), which grades the view of the oropharynx to predict difficult intubation — the two must never be conflated. Assessment also covers airway evaluation, cardiorespiratory and metabolic comorbidity, a drug and allergy history (including anticoagulants and diabetic medication), and relevant investigations. Identified problems are then optimised — blood sugar controlled, anaemia corrected, blood pressure and cardiac or respiratory disease stabilised — so the patient meets surgery in the best achievable state. Two further preoperative pillars are informed consent, a genuine shared understanding of the procedure, its benefits, risks and alternatives, and preoperative fasting to minimise the risk of pulmonary aspiration on induction. Finally, prophylaxis is planned: appropriately timed antibiotics for the surgical wound and a venous-thromboembolism risk assessment (using a tool such as the Wells or Caprini score) to decide on mechanical and pharmacological clot prevention.
Provided image
The ASA-recommended "2-4-6-8" fasting rule replaces the old blanket "nil by mouth after midnight", which needlessly dehydrated patients:
| Intake | Minimum fasting time before anaesthesia |
|---|---|
| Clear fluids (water, clear juice, black tea/coffee) | 2 hours |
| Breast milk | 4 hours |
| Infant formula / light meal (toast, non-human milk) | 6 hours |
| Fatty or fried food, meat | 8 hours |