Page 5 of 11
SU1.3 | Basic Concepts of Perioperative Care — SDL Guide (Part 2)
Intraoperative Safety and Postoperative Recovery
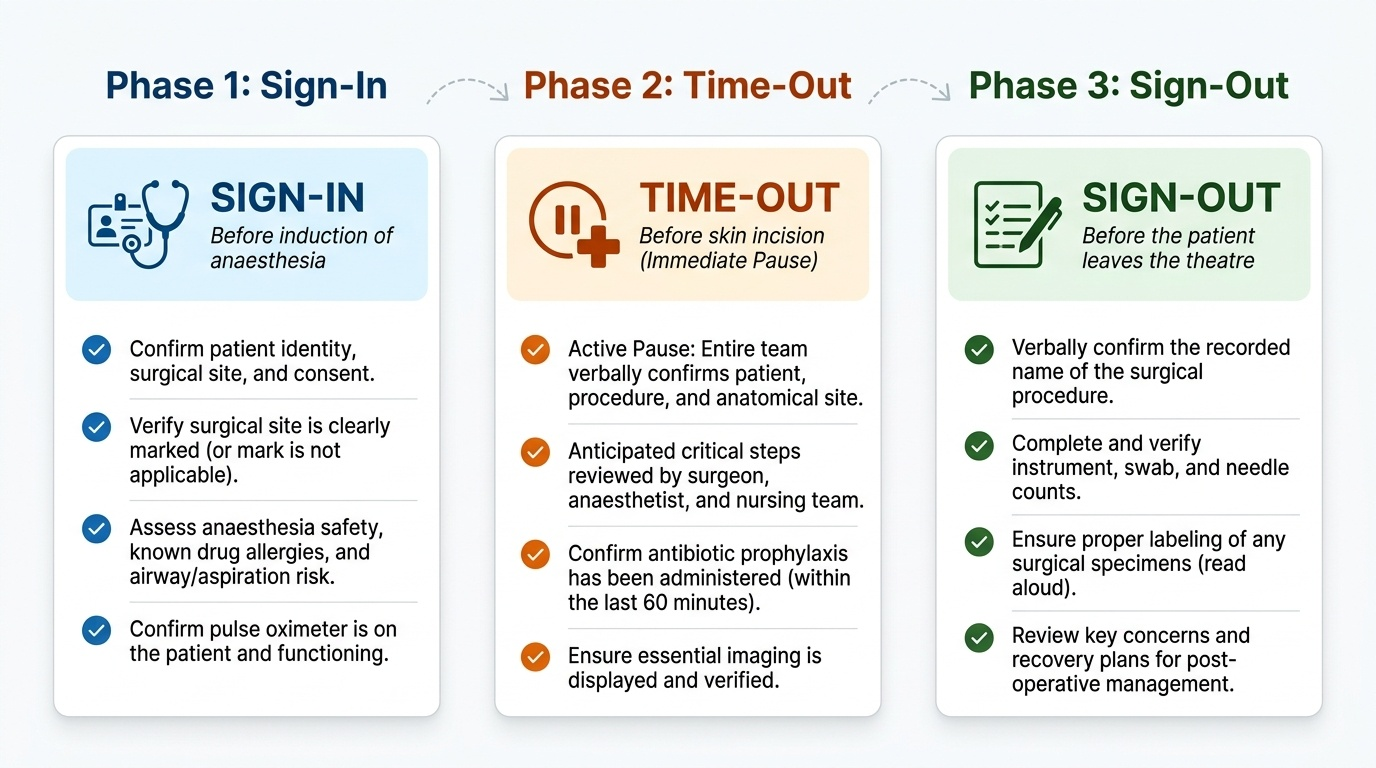
Once the patient enters theatre, safety becomes a matter of disciplined, shared routines rather than individual vigilance. The WHO Surgical Safety Checklist structures this through three formal pauses: a Sign-In before induction of anaesthesia (confirming identity, site, consent, allergies, airway and aspiration risk), a Time-Out before skin incision (the whole team confirms patient, procedure and site, anticipated critical steps, and antibiotic timing), and a Sign-Out before the patient leaves theatre (instrument, swab and needle counts, specimen labelling, and key recovery concerns). Alongside the checklist, intraoperative care maintains strict asepsis to prevent surgical site infection, preserves normothermia because hypothermia worsens bleeding, infection and the stress response, and relies on continuous physiological monitoring of oxygenation, ventilation, circulation and temperature. Recovery then begins immediately in the post-anaesthesia care unit (PACU), where airway, breathing and circulation are watched until the patient is awake and stable. On the ward the priorities are effective multimodal analgesia (often combining regional techniques, paracetamol and opioids, since good pain control lets a patient breathe deeply and mobilise), careful fluid and electrolyte management that respects the salt-and-water-retaining metabolic response, VTE prophylaxis, early mobilisation and nutrition, and active surveillance for complications such as bleeding, infection and the deteriorating patient. The integrating framework for all of this is ERAS (Enhanced Recovery After Surgery) — evidence-based bundles, first validated in colorectal surgery and now spread across specialties, that combine these measures to speed recovery and shorten hospital stay.
Provided image
CLINICAL PEARL
The single most powerful tool against catastrophic surgical error costs nothing and takes a minute: the Time-Out. Before every skin incision the entire team stops and verbally confirms the right patient, the right procedure and the right site — this is the proven defence against wrong-site, wrong-procedure and wrong-patient surgery. Never let a list run so fast that the Time-Out is skipped or mumbled. Equally, never accept a blanket 'nil by mouth from midnight': clear fluids are permitted until two hours before anaesthesia, and the unnecessary dehydration from over-fasting harms far more patients than aspiration does.
SELF-CHECK
A previously well 30-year-old presents for an elective hernia repair. He has no systemic disease. Which ASA physical status grade is most appropriate, and what does the grade describe?
A. ASA I — it describes a normal healthy patient with no systemic disease
B. ASA I — it describes the low technical difficulty of the operation
C. ASA III — it describes a patient with severe systemic disease
D. ASA II — it grades the predicted ease of intubation
Reveal Answer
Answer: A. ASA I — it describes a normal healthy patient with no systemic disease
A healthy patient with no systemic disease is ASA I. The ASA scale grades the patient's systemic disease burden, NOT the difficulty of the operation and NOT the airway — airway/intubation difficulty is predicted by the separate Mallampati classification.
Check Your Understanding
Before moving on, consolidate this material by reasoning a real patient through the whole pathway rather than recalling isolated facts. Picture a 55-year-old man with controlled diabetes listed for an elective inguinal hernia repair, and walk him through the three phases. In the preoperative phase you assess him, assign an ASA grade that reflects his systemic disease, optimise his blood sugar, take informed consent, instruct him on 2-4-6-8 fasting so he may drink clear fluids until two hours before surgery, and complete a venous-thromboembolism risk assessment to plan prophylaxis. In the intraoperative phase the team performs the WHO checklist — Sign-In before induction, Time-Out before incision to confirm patient, procedure and side, and Sign-Out before he leaves theatre — while maintaining asepsis, normothermia and monitoring. In the postoperative phase you provide multimodal analgesia, manage his fluids in light of the salt-and-water-retaining stress response, continue VTE prophylaxis, encourage early mobilisation and watch for complications. Now test yourself on three things: can you name the three phases and the key tasks of each; can you state precisely what the ASA classification grades and how it differs from the Mallampati score; and can you justify, for this patient, why each safety step exists? The questions below check exactly these links.