Page 1 of 11
SU13.1-2 | Transplant Immunology and Immunosuppression — SDL Guide
Learning Objectives
- Describe the immunological basis of organ transplantation, including the HLA/MHC system, donor-recipient matching and allorecognition (SU13.1).
- Distinguish hyperacute, acute and chronic graft rejection by their timing, dominant immune mechanism and histology (SU13.1).
- Discuss the principles of immunosuppressive therapy — induction versus maintenance, the major drug classes, their indications and the risks of infection and malignancy (SU13.2).
INSTRUCTIONS
Transplantation can cure organ failure that no other treatment can touch, yet the same immune system that defends the patient against infection is also what destroys a transplanted organ. Understanding why a graft is rejected, and how immunosuppressive drugs hold that rejection in check, is the foundation on which all of clinical transplantation rests. This module builds the basic immunology and pharmacology a surgeon needs to reason about matching, rejection and the lifelong balancing act of immunosuppression.
References
- Bailey & Love's Short Practice of Surgery, Transplantation chapter (textbook)
- SRB's Manual of Surgery, Organ Transplantation (textbook)
- Sabiston Textbook of Surgery, Transplantation and Immunology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 34-year-old woman has been on haemodialysis for three years. Her brother is a willing kidney donor, and on the day of the operation everything goes well — the new kidney pinks up, fills with blood and, within minutes, makes urine on the table. Three weeks later she is readmitted: her urine output has fallen, her creatinine is climbing, and the graft is tender. The kidney itself is healthy tissue; nothing has gone wrong mechanically. What is happening is immunological — her own immune system has recognised the transplanted organ as foreign and has begun, quietly and predictably, to attack it. Whether that kidney lasts twenty years or twenty days now depends almost entirely on how well we understand and control that immune response. Transplant immunology is the science of winning this battle.
WHY THIS MATTERS
Transplantation is the definitive treatment for end-stage failure of the kidney, liver, heart, lung and pancreas, and the single greatest obstacle to its success is not surgical technique but the recipient's immune system. Every decision in clinical transplantation flows from immunology: who can donate to whom (blood-group and tissue matching), how we screen for pre-existing antibodies that would destroy a graft within minutes (the crossmatch), why a patient must take immunosuppressive drugs for the lifetime of the graft, and why those same drugs leave them vulnerable to infection and cancer. A surgeon who understands the immunological basis can anticipate rejection, interpret a rising creatinine in the right framework, counsel a patient realistically, and recognise the price the patient pays for a working organ. This is foundational surgical science — examined directly and applied at the bedside of every transplant recipient.
RECALL
Before going further, recall three pieces of basic immunology you already know. First, the difference between innate and adaptive immunity, and that the adaptive response is led by T and B lymphocytes that recognise specific antigens. Second, the role of the major histocompatibility complex (MHC) in antigen presentation: MHC molecules display peptide fragments on the cell surface so that T cells can inspect them, and T cells become activated only when they receive both an antigen signal and a co-stimulatory signal. Third, the basic types of hypersensitivity — in particular type II, antibody-mediated cytotoxicity, in which preformed antibodies bind a target and trigger complement and cell-mediated destruction. Keep these in mind: graft rejection is essentially these familiar mechanisms turned against a transplanted organ.
Why Transplant Immunology Decides Whether a Graft Survives
Transplantation is the transfer of an organ or tissue from one site or individual to another to replace failed function, and its central problem is immunological rejection — the recipient's immune recognition and destruction of the graft as foreign. The likelihood and pattern of rejection depend on how genetically different the donor and recipient are, which is why the relationship between them is described by terms you must use precisely. An autograft is transferred within the same individual (a skin graft from thigh to face) and is never rejected. An isograft is between genetically identical individuals (identical twins) and is likewise immunologically accepted. An allograft — by far the commonest clinical situation — is between two genetically different members of the same species, and it is an allograft that the immune system attacks; the proteins that mark the graft as foreign are called alloantigens. A xenograft is between different species and faces the most violent rejection of all. Because the allograft is the clinical reality, the whole of transplant immunology is built around predicting, preventing and treating the rejection of allografts. This matters to the surgeon because rejection is largely predictable in its timing and mechanism, and — crucially — modifiable: careful donor-recipient matching reduces the immunological mismatch, and immunosuppressive drugs blunt the response, allowing a foreign organ to survive for years in a host that would otherwise destroy it within days.
HLA/MHC Class I and Class II Antigen Presentation
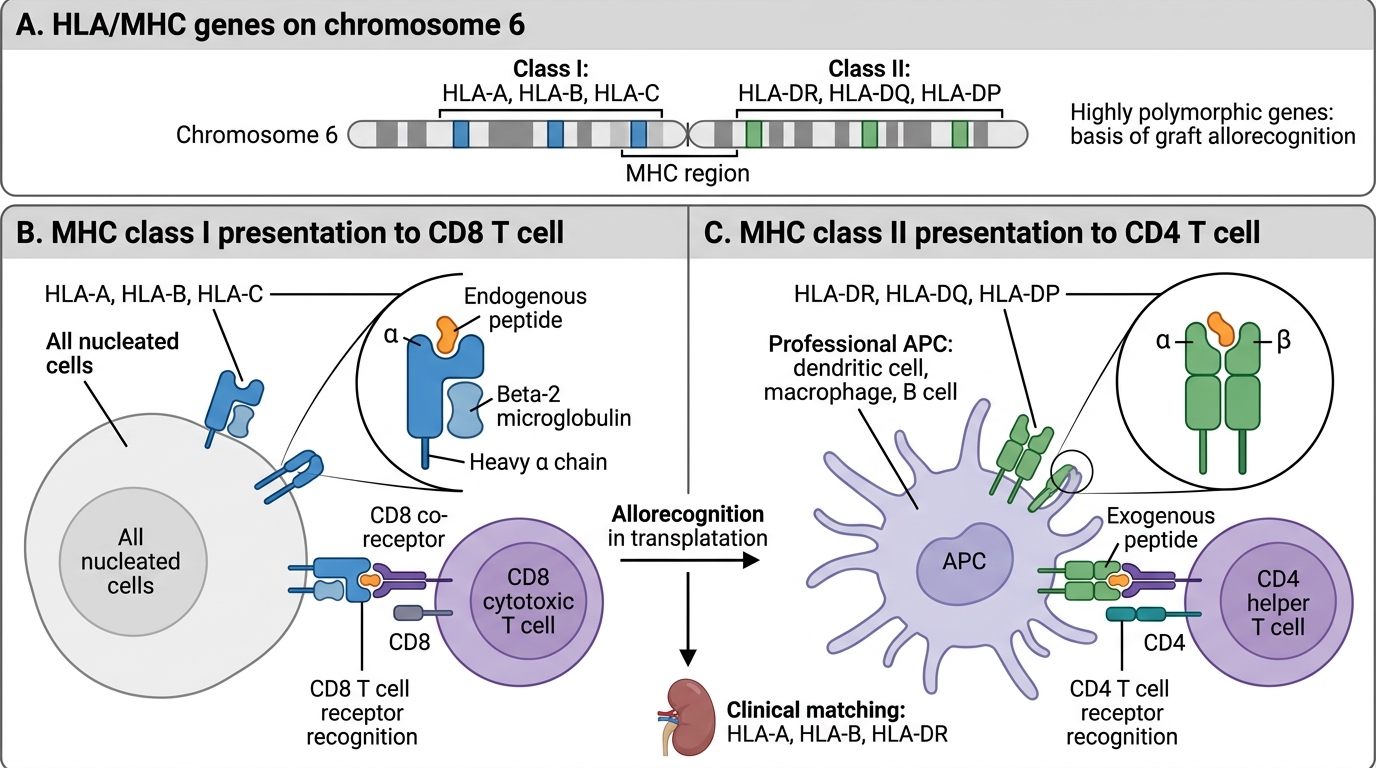
The HLA/MHC System and the Basis of Allorecognition
The molecules that the recipient's immune system reads as 'foreign' on a graft are chiefly the human leucocyte antigens (HLA) — the human version of the major histocompatibility complex (MHC), encoded by a cluster of highly polymorphic genes on chromosome 6. Because these genes are so variable in the population, two unrelated people almost never share the same set, which is exactly why an allograft is recognised as foreign. HLA molecules come in two classes that you must distinguish. HLA class I molecules — HLA-A, HLA-B and HLA-C — are expressed on the surface of essentially all nucleated cells and present peptide antigen to CD8 (cytotoxic) T cells. HLA class II molecules — HLA-DR, HLA-DQ and HLA-DP — are expressed mainly on professional antigen-presenting cells such as dendritic cells, macrophages and B cells, and present antigen to CD4 (helper) T cells. For clinical kidney transplantation the loci that matter most are HLA-A, HLA-B and HLA-DR, and the better these are matched between donor and recipient, the longer the graft tends to survive. Two further immunological screens are essential. ABO blood-group compatibility is required because the A and B antigens behave as transplantation antigens on the graft endothelium and preformed anti-A/anti-B antibodies would destroy an incompatible organ immediately. The crossmatch mixes recipient serum with donor lymphocytes to detect preformed anti-donor HLA antibodies; a positive crossmatch is a contraindication to transplantation because it predicts hyperacute rejection.
| Feature | HLA class I | HLA class II |
|---|---|---|
| Examples | HLA-A, HLA-B, HLA-C | HLA-DR, HLA-DQ, HLA-DP |
| Expressed on | All nucleated cells | Antigen-presenting cells (dendritic, macrophage, B cell) |
| Presents antigen to | CD8 cytotoxic T cells | CD4 helper T cells |
| Main clinical-matching loci | HLA-A, HLA-B | HLA-DR |
SELF-CHECK
Before a kidney transplant, mixing the recipient's serum with the donor's lymphocytes shows that the recipient has preformed antibodies against the donor's cells (a positive crossmatch). What does this predict, and what is the appropriate action?
A. It predicts chronic rejection over years; proceed and monitor
B. It predicts hyperacute rejection within minutes to hours; transplantation is contraindicated
C. It predicts acute cellular rejection at 2 weeks; increase steroids
D. It is a normal finding; proceed without concern
Reveal Answer
Answer: B. It predicts hyperacute rejection within minutes to hours; transplantation is contraindicated
A positive crossmatch means the recipient already has preformed anti-donor HLA antibodies. On revascularisation these bind the graft endothelium and trigger complement-mediated hyperacute rejection within minutes to hours, thrombosing the graft. A positive crossmatch is therefore a contraindication to transplantation with that donor.
How the Immune System Rejects a Graft: Mechanisms and Patterns of Rejection
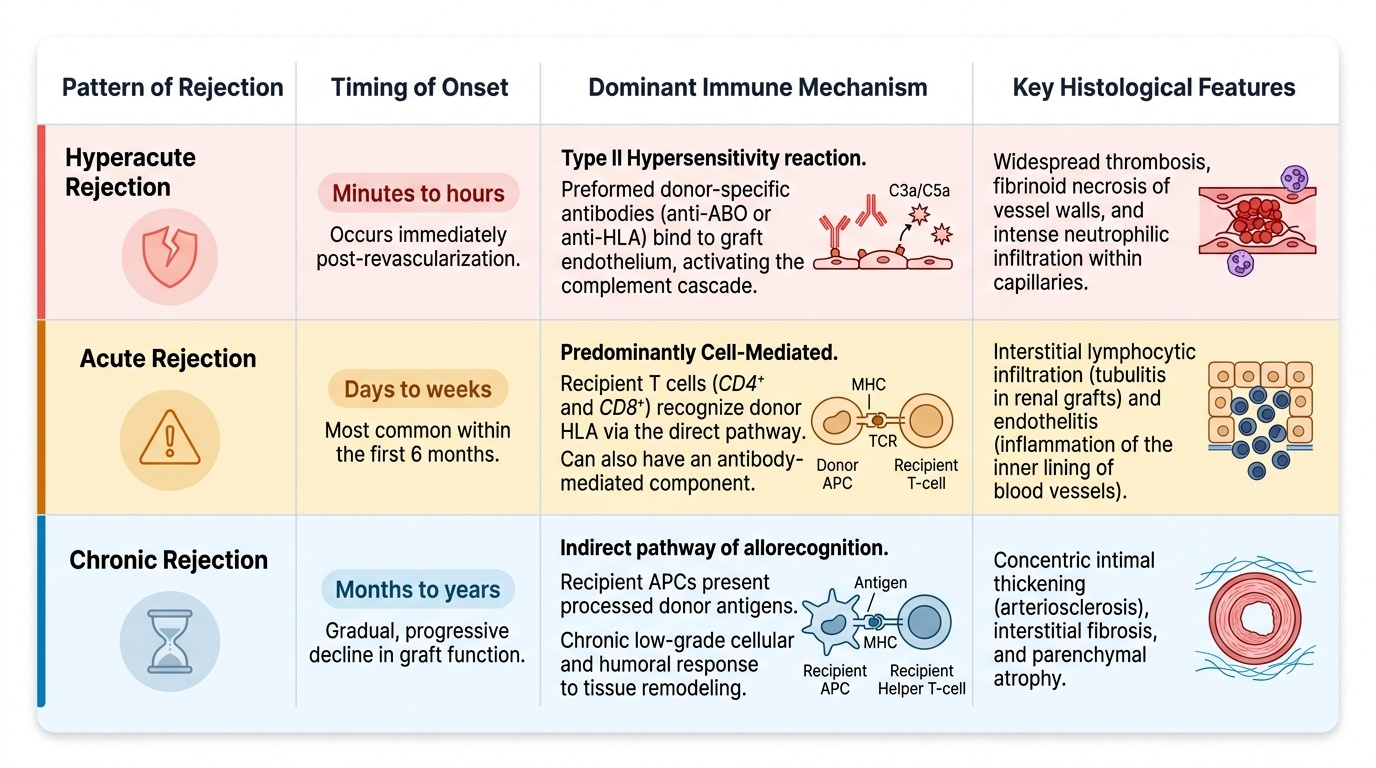
Rejection begins with allorecognition — the recipient's T cells recognising donor HLA as foreign. This happens by two complementary routes: the direct pathway, in which recipient T cells recognise intact donor HLA molecules displayed on donor antigen-presenting cells carried within the graft (the dominant driver of early acute rejection), and the indirect pathway, in which recipient antigen-presenting cells process shed donor antigen and present it on the recipient's own HLA (important in late and chronic rejection). Activated CD4 helper T cells then coordinate the attack: CD8 cytotoxic T cells kill graft cells directly, and B cells mature into plasma cells that produce anti-donor antibodies. The clinical result is classified by timing and mechanism into three patterns. Hyperacute rejection occurs within minutes to hours of revascularisation and is caused by preformed antibodies (anti-ABO or anti-HLA) — a type II antibody-mediated reaction that activates complement, thromboses graft vessels and is essentially untreatable, which is why ABO matching and the crossmatch exist to prevent it. Acute rejection occurs over days to weeks (most often in the first six months) and is predominantly cell-mediated (T-cell) rejection, though antibody-mediated acute rejection also occurs; it presents as graft dysfunction (a rising creatinine and tender graft in a kidney), is confirmed on biopsy, and — importantly — is usually reversible with intensified immunosuppression. Chronic rejection develops over months to years, is driven by both immune (largely the indirect pathway and chronic antibody injury) and non-immune factors, shows progressive fibrosis and graft vasculopathy on histology, and responds poorly to treatment — it is the main cause of late graft loss. Distinct from all three is graft-versus-host disease, in which immunocompetent donor lymphocytes (notably in bone-marrow or intestinal transplantation) attack the immunosuppressed recipient's tissues — the reverse direction of attack.
Provided image
- Hyperacute: minutes-hours; preformed anti-ABO/anti-HLA antibodies (type II); vascular thrombosis; prevented by ABO matching and crossmatch, not treatable.
- Acute: days-weeks (usually first 6 months); predominantly T-cell (cellular), also antibody-mediated; reversible with intensified immunosuppression.
- Chronic: months-years; immune (indirect pathway, chronic antibody) plus non-immune injury; fibrosis and graft vasculopathy; main cause of late graft loss, treatment-resistant.
- Graft-versus-host disease: donor lymphocytes attack the recipient — the opposite direction (bone-marrow/intestinal transplants).