Page 2 of 11
SU13.1-2 | Transplant Immunology and Immunosuppression — SDL Guide (Part 2)
Principles of Immunosuppressive Therapy
Because an allograft would otherwise be rejected, recipients require immunosuppression — drugs that dampen the immune response — and the central principle is to give enough to prevent rejection while limiting the inevitable harms of over-suppression. Immunosuppression is delivered in two phases. Induction is intense immunosuppression given at the time of transplantation to blunt the early, high-risk period; it uses antibody preparations such as basiliximab (a non-depleting anti-CD25 / IL-2-receptor monoclonal antibody) or depleting agents such as anti-thymocyte globulin. Maintenance immunosuppression is then continued for the life of the graft, typically combining drugs from different classes at lower doses to maximise effect while minimising any single drug's toxicity. The major maintenance classes are: calcineurin inhibitors — ciclosporin and tacrolimus — the backbone of most regimens, which block calcineurin and thereby IL-2-driven T-cell activation (nephrotoxicity is their key adverse effect); antiproliferatives — mycophenolate mofetil and azathioprine — which inhibit lymphocyte proliferation (causing bone-marrow suppression); corticosteroids, which are broadly anti-inflammatory and immunosuppressive (with the familiar long-term metabolic, bone and infective effects); and mTOR inhibitors — sirolimus (rapamycin) and everolimus — which block proliferation signalling. The indications for transplantation are end-stage organ failure (chronic kidney disease, decompensated cirrhosis, end-stage heart or lung disease, type 1 diabetes); the surgical principles are meticulous vascular and (for kidney) ureteric anastomosis with minimal cold-ischaemia time, and lifelong follow-up. The unavoidable price of immunosuppression is twofold and must be counselled: an increased risk of opportunistic infection (cytomegalovirus, Pneumocystis, BK virus, fungal infection) and an increased long-term risk of malignancy, especially skin cancers and post-transplant lymphoproliferative disorder.
Provided image
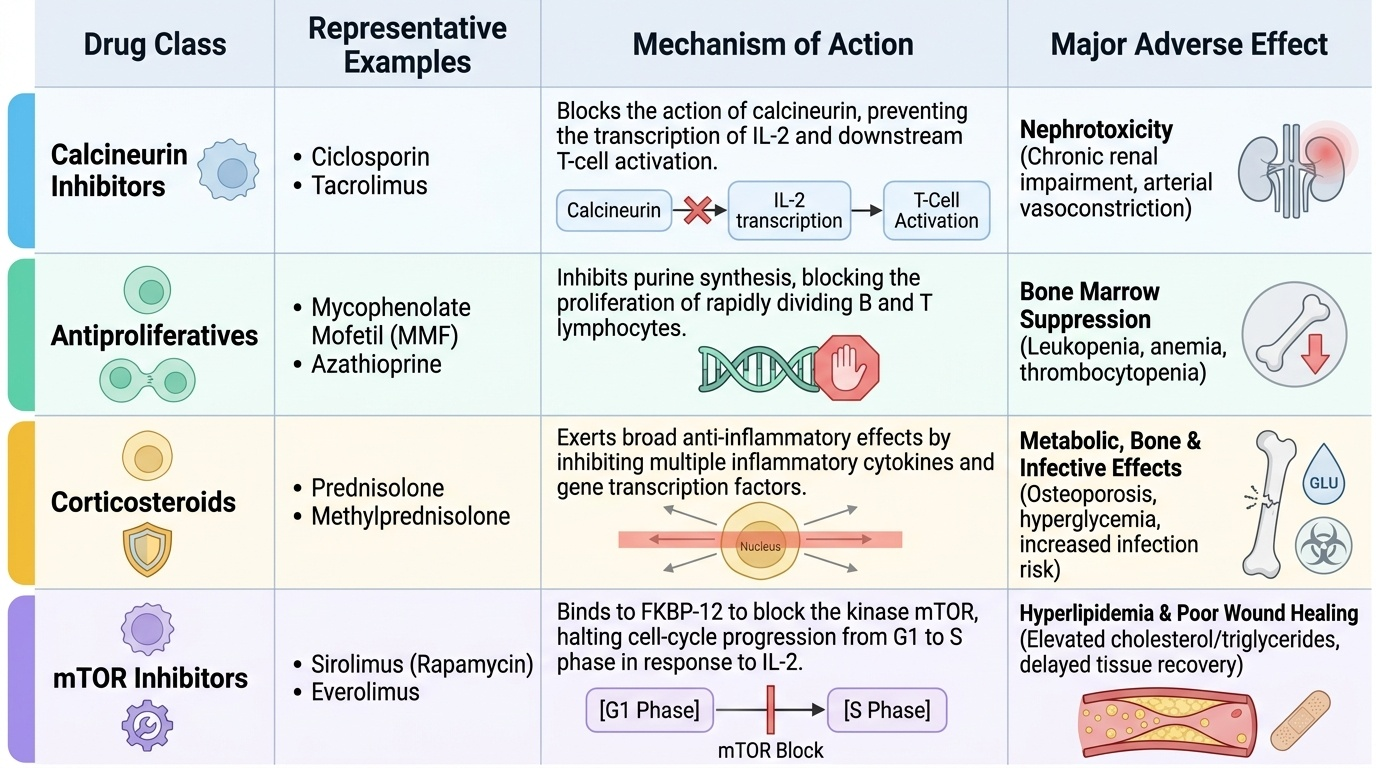
| Class | Example drugs | Mechanism | Major adverse effect |
|---|---|---|---|
| Calcineurin inhibitors | Ciclosporin, tacrolimus | Block calcineurin → reduce IL-2 / T-cell activation | Nephrotoxicity |
| Antiproliferatives | Mycophenolate mofetil, azathioprine | Inhibit lymphocyte (purine) proliferation | Bone-marrow suppression |
| Corticosteroids | Prednisolone | Broad anti-inflammatory / immunosuppressive | Metabolic, bone, infection |
| mTOR inhibitors | Sirolimus, everolimus | Block mTOR proliferation signalling | Impaired wound healing, dyslipidaemia |
Check Your Understanding
Before moving on, consolidate the model by reasoning through it rather than recalling isolated facts. Picture the kidney recipient from the start of this module and trace the immunology end to end. First, matching: she received a graft only after ABO compatibility was confirmed and a negative crossmatch excluded preformed anti-donor antibodies, with HLA-A, HLA-B and HLA-DR matched as far as possible to lower the immunological load. Second, rejection patterns: because the crossmatch was negative she did not suffer hyperacute rejection on the table; her three-week presentation with a rising creatinine and tender graft is the classic picture of acute, predominantly cell-mediated rejection — confirmed on biopsy and, importantly, reversible with intensified immunosuppression. Third, immunosuppression: she will remain on lifelong maintenance therapy, typically a calcineurin inhibitor plus an antiproliferative plus a steroid, balanced to prevent rejection without tipping her into infection or malignancy. Test yourself on three links: can you name each HLA class and the T-cell subset it engages; can you place a given rejection scenario into the correct pattern by its timing and mechanism; and can you match each immunosuppressive class to its mechanism and its principal adverse effect? The short question below checks exactly these connections.
CLINICAL PEARL
A negative pre-transplant crossmatch does NOT mean rejection will never happen — it only excludes the preformed antibodies that cause hyperacute rejection. Acute cellular rejection, driven by the recipient's T cells, can still appear over the following days to weeks and typically declares itself as graft dysfunction (a rising creatinine and a tender graft in a kidney transplant). The key clinical point is that acute rejection, unlike hyperacute, is usually reversible if recognised early and treated with intensified immunosuppression — so a rising creatinine in a transplant recipient demands prompt investigation, not watchful waiting.
SELF-CHECK
A kidney transplant recipient on maintenance therapy is found to have nephrotoxicity attributed to one of her immunosuppressive drugs. Which class is the most likely culprit, and by what mechanism does it work?
A. Antiproliferative (mycophenolate) — inhibits lymphocyte proliferation
B. Calcineurin inhibitor (tacrolimus or ciclosporin) — blocks calcineurin and IL-2-driven T-cell activation
C. Corticosteroid (prednisolone) — broad anti-inflammatory action
D. mTOR inhibitor (sirolimus) — blocks proliferation signalling
Reveal Answer
Answer: B. Calcineurin inhibitor (tacrolimus or ciclosporin) — blocks calcineurin and IL-2-driven T-cell activation
Calcineurin inhibitors — ciclosporin and tacrolimus — are the backbone of maintenance immunosuppression; they block calcineurin and thereby IL-2-driven T-cell activation, but their characteristic and dose-limiting adverse effect is nephrotoxicity. Antiproliferatives cause marrow suppression, steroids cause metabolic/bone/infective effects, and mTOR inhibitors impair wound healing and cause dyslipidaemia.