Page 1 of 11
SU4.1-2 | Burns Assessment and Pathophysiology — SDL Guide
Learning Objectives
- Elicit, document and present a focused history and perform a structured physical examination in a patient with burns (SU4.1).
- Describe the local and systemic pathophysiology of burns, including burn shock (SU4.1).
- Describe the clinical features of burns and diagnose the type and extent (depth and %TBSA) of a burn (SU4.2).
- Plan appropriate initial treatment, including fluid resuscitation by the Parkland formula and criteria for referral to a burns unit (SU4.2).
INSTRUCTIONS
A burn is one of the few surgical emergencies in which a junior doctor's first-hour decisions visibly determine survival. The injury is deceptively simple to see and easy to underestimate: the visible wound is only the surface of a whole-body disease driven by massive fluid shifts, a hypermetabolic state and the constant threat of airway loss and infection. This module connects what you can observe at the bedside — the mechanism, the depth, the surface area — to the pathophysiology that explains why a large burn behaves like haemorrhage without bleeding, and then to the structured plan (airway, fluids, referral) that follows directly from an accurate assessment. Get the assessment right and the resuscitation almost writes itself.
References
- Bailey & Love's Short Practice of Surgery, Burns (textbook)
- SRB's Manual of Surgery, Burns (textbook)
- Sabiston Textbook of Surgery, Burns (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 a.m. and a 30-year-old man is wheeled in from a house fire. His face is sooty, his eyebrows are singed, and his voice has a rough, hoarse edge that was not there yesterday. His chest, both arms and the front of his abdomen are an angry mix of weeping red and pale, leathery skin. He is talking, frightened, asking for water — and to the untrained eye he looks stable. Yet within the hour the airway you can still see may swell shut, and the fluid silently leaking out of every burned capillary may tip him into shock. Nothing about his blood pressure right now tells you this. Everything about how you assess his airway, estimate how much of his body is burned, and start his fluids in the next sixty minutes does. This is why burns assessment is a skill worth doing precisely, every single time.
WHY THIS MATTERS
Burns are common in India, where open flames, kerosene stoves and scalds injure huge numbers of people, many of them children and young women. For a final-year student and intern, burns are also a guaranteed clinical encounter — in casualty, on the wards, and in examinations — and they reward a systematic mind. The reason assessment matters so much is that almost every downstream decision flows from two numbers and one judgement: the depth of the burn, the percentage of total body surface area burned, and whether the airway is threatened. From those you calculate fluids, decide on referral, anticipate complications, and counsel the family. Conversely, the commonest fatal errors in early burns care are not exotic: they are missing an inhalation injury, under-estimating the burned area, and under-resuscitating because fluids were started late or calculated from the wrong starting time. Mastering assessment is therefore the single highest-yield burns skill you will learn.
RECALL
Before building the clinical picture, recall some foundations. From anatomy and histology: the skin has a thin outer epidermis and a thicker dermis (a superficial papillary and a deeper reticular layer), and buried within the dermis are the dermal appendages — hair follicles, sebaceous and sweat glands — that are lined by epithelial cells. These appendages are the reservoir from which a partial-thickness burn re-grows its surface; once the burn destroys the full depth of dermis, that reservoir is gone and spontaneous healing fails. From physiology: recall the Starling forces governing fluid across capillaries — the balance of hydrostatic and oncotic pressure that normally keeps plasma in the vessels. A burn unleashes inflammatory mediators that make capillaries leaky, so plasma pours into the interstitium; holding on to this idea is the key to understanding burn shock and why we resuscitate with large volumes of fluid.
Clinical Presentation: History and Examination of the Burned Patient
A burned patient must be approached not as a wound to be dressed but as a trauma patient, because a major burn can kill through the airway and through fluid loss long before the skin becomes a problem. The history is therefore taken in parallel with a structured primary survey along the ABCDE sequence (Airway, Breathing, Circulation, Disability, Exposure). The single most important early task is to recognise an inhalation injury and an airway at risk, because oedema can convert a patent airway into an obstructed one within hours and intubation is far safer done early. Crucial history points are the mechanism (flame, scald, electrical, chemical), whether the injury occurred in an enclosed space (which hugely raises the risk of inhalation injury and carbon monoxide poisoning), the duration of contact, what first aid was given, the exact time of the burn (this anchors all fluid calculations), and the patient's tetanus status, comorbidities and any suspicion of non-accidental injury. On examination, look actively for the airway and inhalation red flags, then quantify the wound, because the assessment you document now drives every later decision.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
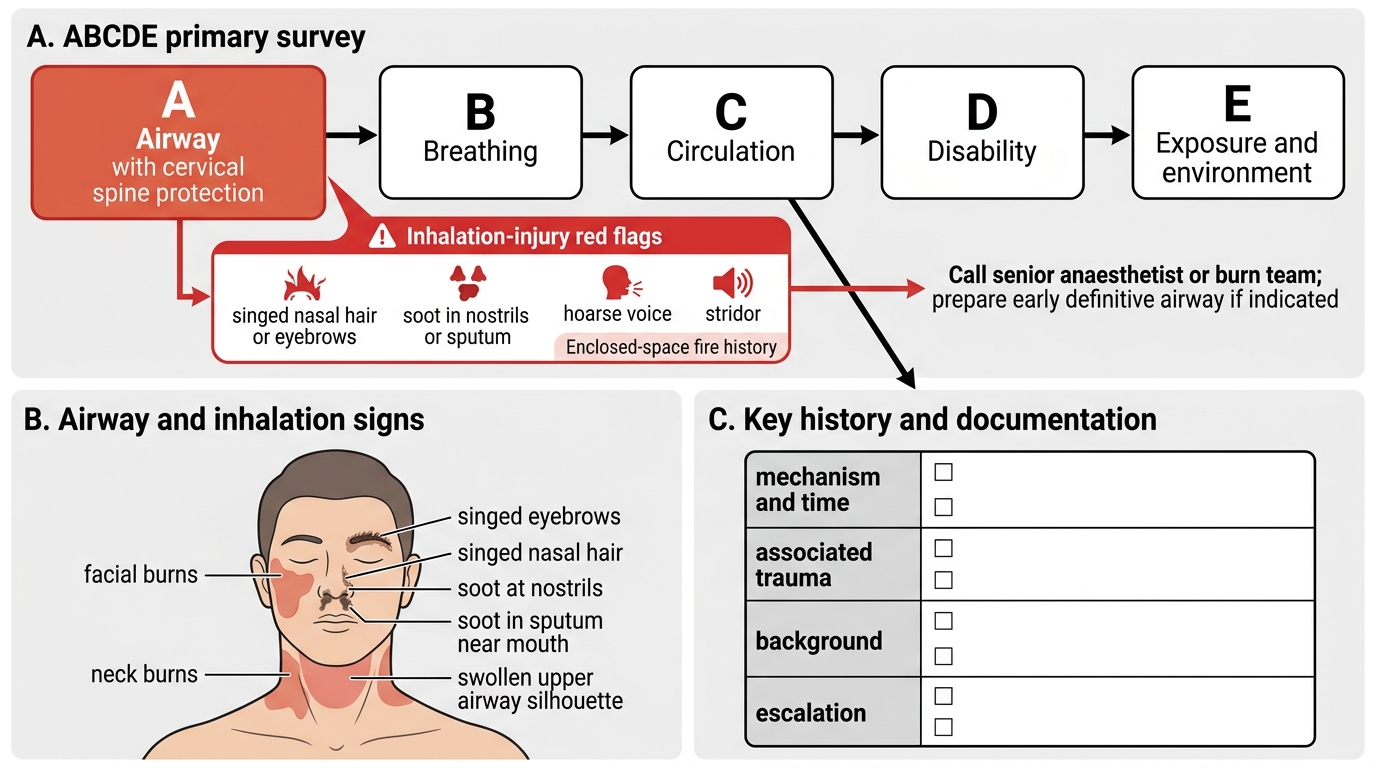
Initial Assessment of Major Burns: ABCDE and Airway Red Flags
Key features to elicit and document:
- Airway/inhalation red flags: burns to the face and neck, singed nasal hair and eyebrows, soot in the nostrils or sputum, a hoarse voice or stridor, and a history of fire in an enclosed space.
- Mechanism and time: flame, scald, contact, electrical or chemical; and the precise clock time the burn occurred.
- Associated injuries: falls, blasts or jumps from height may add fractures or visceral injury — a burn does not exclude other trauma.
- Background: age, weight (needed for fluid calculation), comorbidities, tetanus immunisation, and the social circumstances of the injury.
Pathophysiology of Burns: Local Wound and Systemic Burn Shock
Understanding why a large burn is dangerous requires separating the local wound response from the systemic response. Locally, the classic description is Jackson's burn-wound model of three concentric zones. At the centre is the zone of coagulation, where the tissue is irreversibly dead from protein denaturation. Surrounding it is the critical zone of stasis, where tissue is injured but potentially salvageable: perfusion here is sluggish, and if the patient is under-resuscitated, allowed to become hypotensive, or develops infection, this zone progresses to necrosis and the burn effectively deepens. The outermost zone of hyperaemia has increased blood flow and usually recovers. Good early care — adequate fluids and wound care — is largely aimed at saving the zone of stasis. Systemically, a burn covering a large surface area releases inflammatory mediators that increase capillary permeability throughout the body, so plasma leaks into the interstitium causing massive oedema and a fall in circulating volume; this distributive-and-hypovolaemic picture is burn shock. Beyond the first day the patient enters a prolonged hypermetabolic, catabolic state with immunosuppression that raises the risk of sepsis, and stress-related gastroduodenal ulceration known as Curling's ulcer may occur. These mechanisms explain why we resuscitate aggressively, feed early, and guard relentlessly against infection.
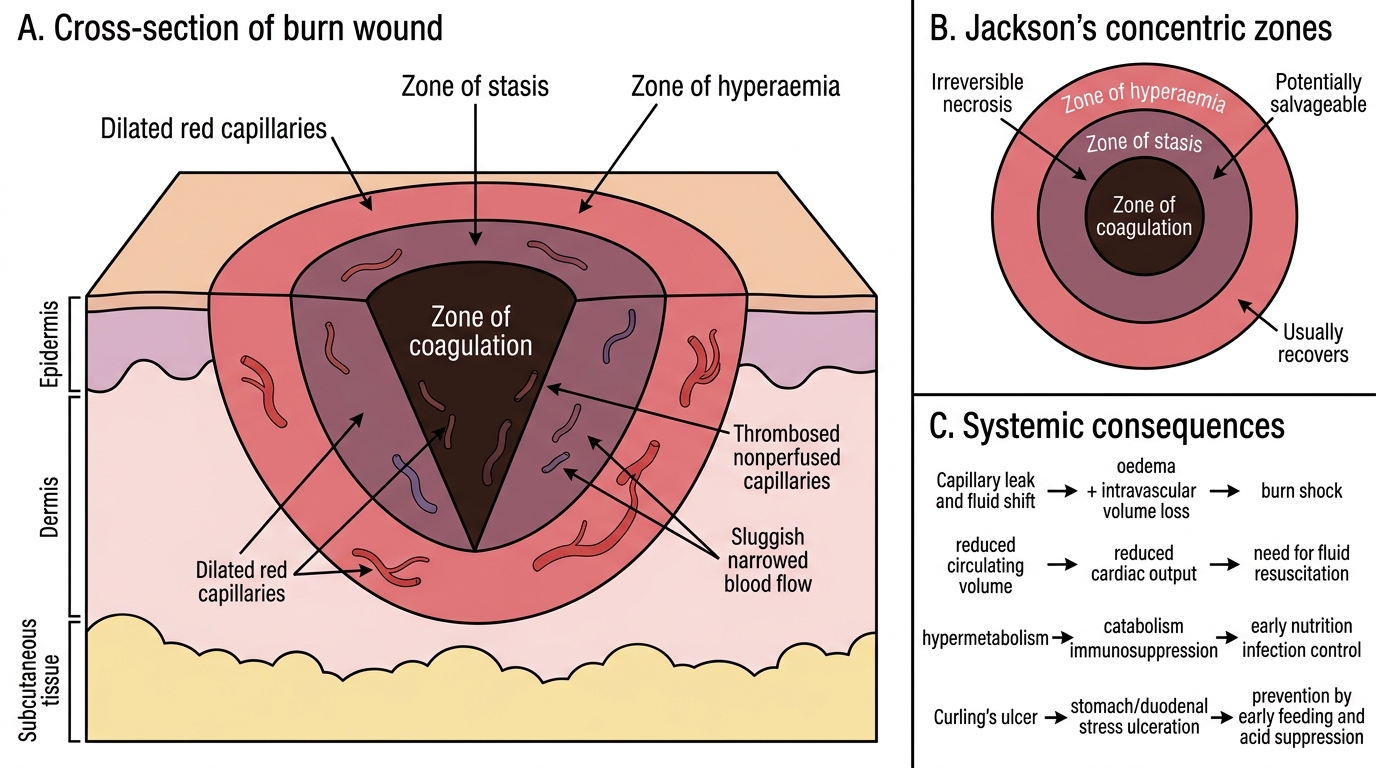
Jackson's Three Zones of a Burn Wound
The systemic consequences in sequence:
- Capillary leak and fluid shift: increased permeability moves plasma into tissues, producing oedema and intravascular volume loss — the basis of burn shock.
- Cardiovascular: reduced circulating volume lowers cardiac output early; this is the rationale for the resuscitation formula.
- Hypermetabolism: a sustained catabolic, immunosuppressed state follows, driving the need for early nutrition and infection control.
- Curling's ulcer: acute stress ulceration of the stomach/duodenum, prevented by early feeding and acid suppression.
SELF-CHECK
In Jackson's model of the burn wound, which zone is potentially salvageable and may progress to necrosis if the patient is under-resuscitated or becomes infected?
A. Zone of coagulation
B. Zone of stasis
C. Zone of hyperaemia
D. Zone of demarcation
Reveal Answer
Answer: B. Zone of stasis
The central zone of coagulation is irreversibly dead and the outer zone of hyperaemia usually recovers. It is the intermediate zone of stasis — injured but viable tissue with precarious perfusion — that can be saved by good resuscitation or lost (deepening the burn) if the patient is allowed to become hypotensive or septic.
Assessing Depth and Extent: Diagnosing Type and TBSA
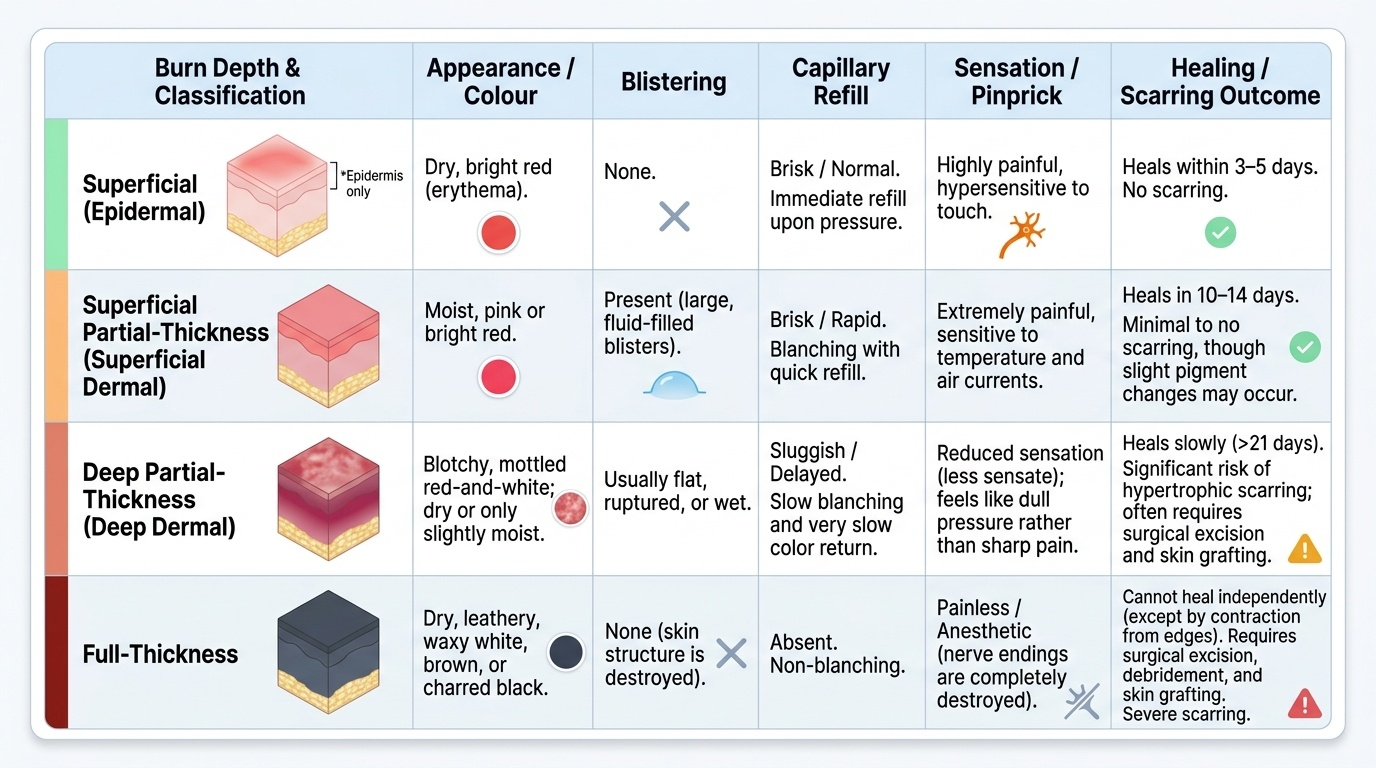
Two measurements convert a frightening wound into a manageable plan: how deep the burn is and how much of the body it covers. Depth is judged clinically from appearance, blistering, capillary refill, sensation and the likely healing outcome, and is conventionally graded as superficial (epidermal) — dry, red, painful, no blisters, like simple sunburn, healing in days without scarring; superficial partial-thickness (superficial dermal) — moist, pink, blistered, very painful with brisk capillary refill, healing in about two weeks; deep partial-thickness (deep dermal) — blotchy red-and-white, less sensate, sluggish capillary refill, healing slowly with scarring and often needing grafting; and full-thickness — dry, leathery, white or charred, painless because the nerve endings are destroyed, and unable to heal except by contraction and grafting. Depth matters because it predicts healing and the need for surgery. Extent is expressed as percentage total body surface area (%TBSA), counting partial-thickness and deeper burns but NOT simple epidermal erythema. Three tools are used: Wallace's rule of nines for a rapid adult estimate; the patient's palm including the fingers, taken as roughly 1% TBSA, for small or scattered burns; and the age-corrected Lund-Browder chart, which is the most accurate and is essential in children, whose head is proportionally larger and limbs proportionally smaller than an adult's, so the adult rule of nines would mis-estimate their burns.
Provided image
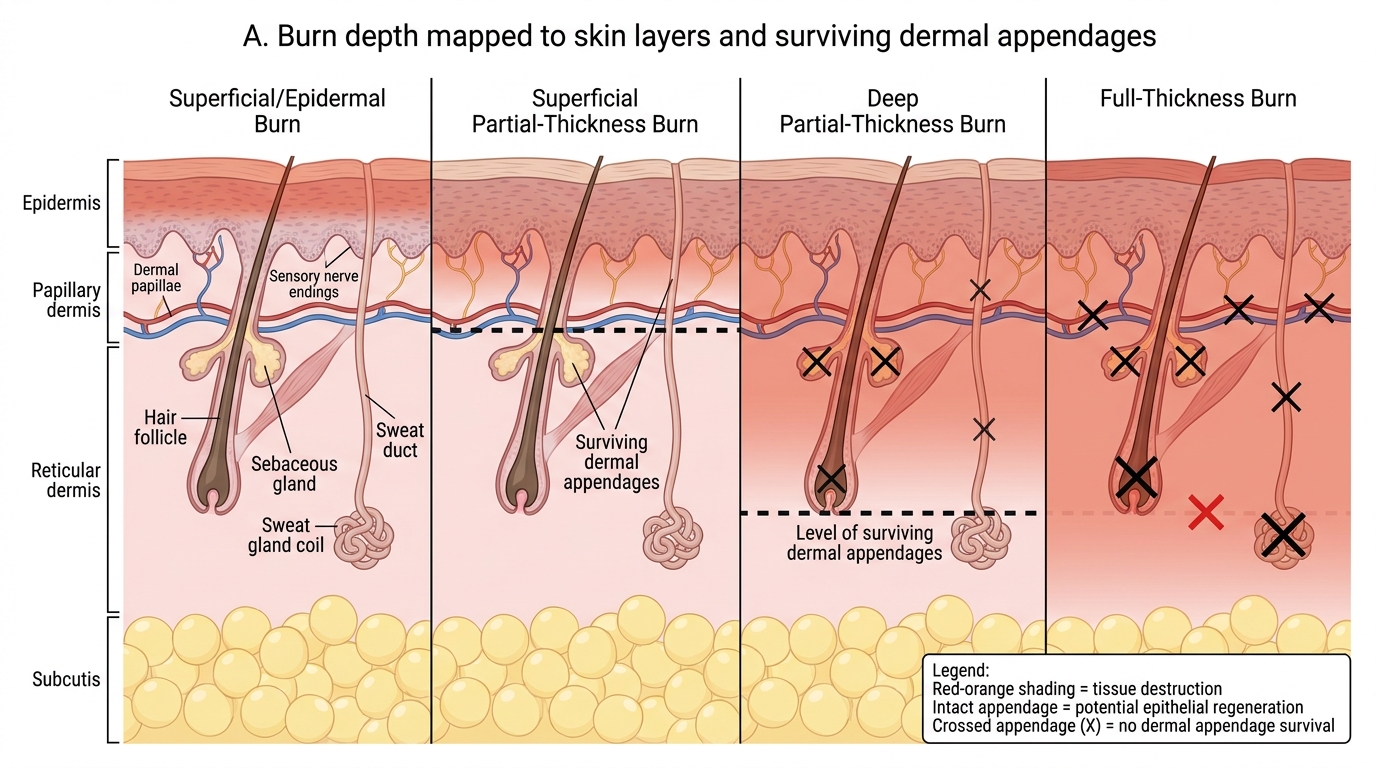
Burn Depths and Surviving Dermal Appendages
In the adult, Wallace's rule of nines assigns body regions in multiples of nine:
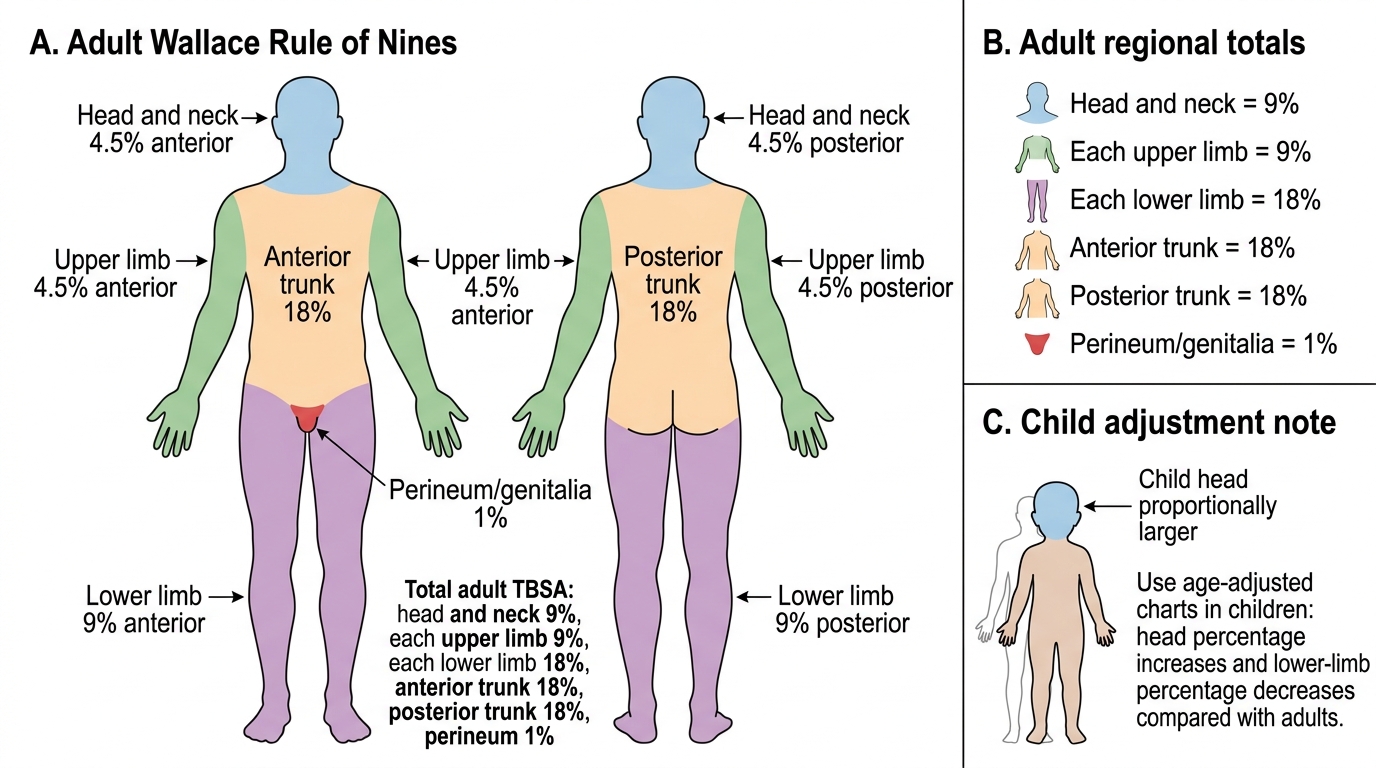
Wallace Rule of Nines for Adult Burns
- Head and neck: 9%
- Each upper limb: 9%
- Each lower limb: 18%
- Anterior trunk: 18%
- Posterior trunk: 18%
- Perineum/genitalia: 1%
The clinical features distinguishing the burn depths are best compared side by side:
| Depth | Appearance | Blisters | Capillary refill | Sensation | Healing |
|---|---|---|---|---|---|
| Superficial (epidermal) | Dry, red | None | Brisk | Painful | Days, no scar; NOT counted in %TBSA |
| Superficial partial-thickness | Moist, pink | Present | Brisk | Very painful | ~2 weeks, minimal scar |
| Deep partial-thickness | Blotchy red/white | May be present | Sluggish | Reduced | Slow, scarring; may need graft |
| Full-thickness | Dry, white/leathery/charred | None | Absent | Painless | Will not heal spontaneously; needs graft |