Page 2 of 11
SU4.1-2 | Burns Assessment and Pathophysiology — SDL Guide (Part 2)
Planning Treatment: Fluid Resuscitation and Criteria for Referral
Once depth and %TBSA are known, the initial plan follows logically: secure the airway, replace the fluid the burn will lose, relieve any constriction, and decide who needs specialist care. Fluid resuscitation is the heart of early management and is calculated with the Parkland (Baxter) formula: 4 mL of Ringer's lactate per kilogram of body weight per percentage of TBSA burned, given over the first 24 hours. The timing is what students most often get wrong: half of this calculated volume is given in the first 8 hours measured from the time of the burn itself — not from the time of arrival in hospital — and the remaining half is given over the next 16 hours. If a patient reaches you four hours after the burn, that first half must therefore be delivered in the four hours that remain. The formula is only a starting estimate; resuscitation is then titrated to an end-point of urine output of 0.5-1 mL/kg/h in an adult (around 1 mL/kg/h in a child), measured via a urinary catheter. Alongside fluids, an inhalation injury or an airway at risk demands early intubation; a circumferential full-thickness burn of a limb can act as a tourniquet as oedema builds and may need escharotomy (incision through the dead eschar to restore perfusion), while a circumferential chest burn restricting ventilation needs the same. Analgesia, tetanus prophylaxis and wound care complete the early package. Finally, recognise which burns exceed local capability and require transfer to a burns unit.
Parkland Formula Worked Example
Widely used criteria for referral to a specialist burns unit include:
- Partial-thickness burns greater than about 10% TBSA (and any large full-thickness burn).
- Burns involving the face, hands, feet, perineum/genitalia or major joints.
- Electrical (including lightning) and significant chemical burns.
- Inhalation injury, or burns with associated major trauma.
- Circumferential burns, burns at the extremes of age, and burns in patients with significant comorbidity.
CLINICAL PEARL
Always calculate the first half of the Parkland fluid from the time of the burn, not the time of arrival. A patient who reaches casualty three hours after a flame burn has already 'used up' three of the eight hours, so the first half must be delivered in the five hours that remain — running it over the full eight from arrival silently under-resuscitates the patient. And never let a normal blood pressure reassure you in a major burn: hypotension is a late sign, so titrate to urine output (0.5-1 mL/kg/h in adults), not to the cuff.
Self-Assessment: Consolidating Burns Assessment
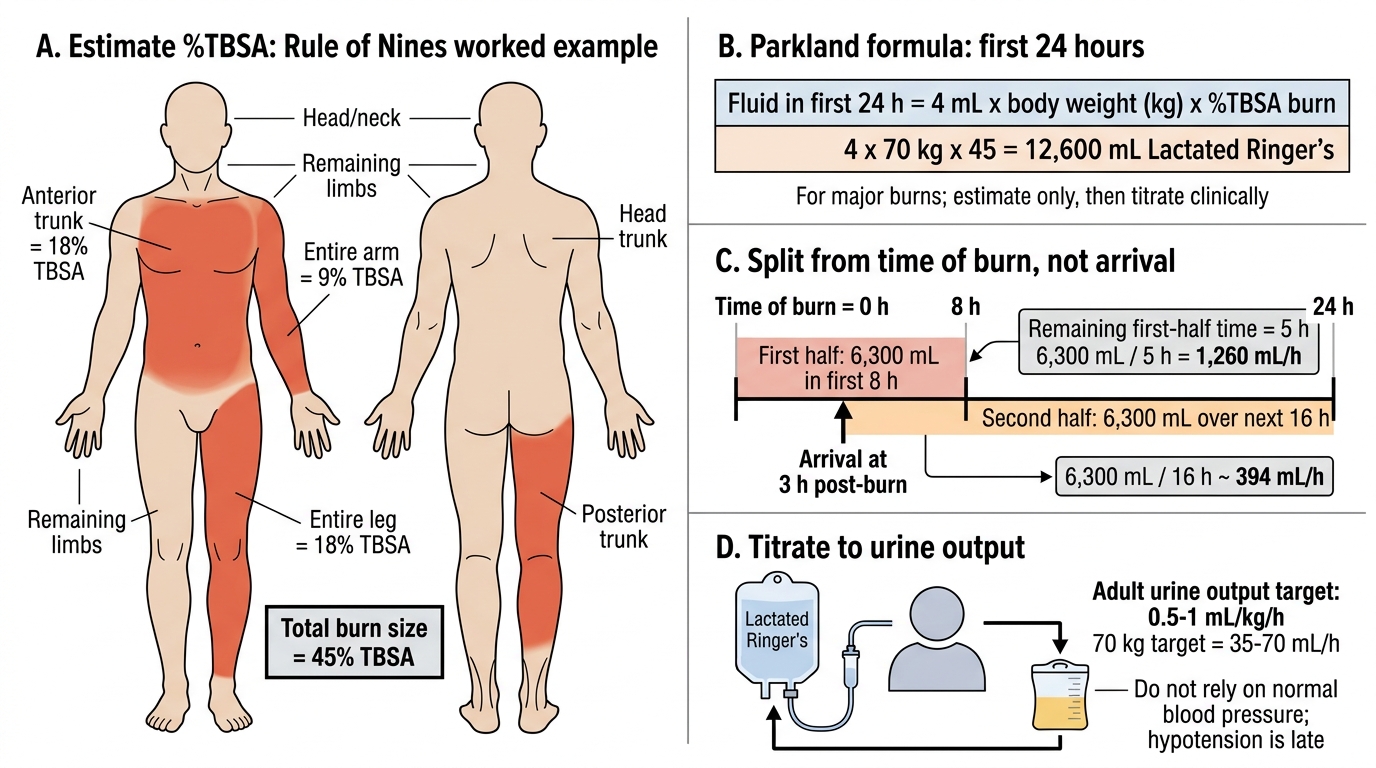
Test your integrated understanding with a worked scenario before moving on. A 70 kg man sustains flame burns to the whole of his anterior trunk, the whole of one entire arm and the front and back of one entire leg. Work through the assessment in order. First estimate the %TBSA using Wallace's rule of nines: anterior trunk 18%, one whole upper limb 9%, and one whole lower limb 18% — a total of about 45% TBSA. Next apply the Parkland formula: 4 mL x 70 kg x 45 = 12,600 mL of Ringer's lactate over 24 hours, of which half (6,300 mL) is given in the first 8 hours from the time of the burn and the remaining 6,300 mL over the next 16 hours. Then state your end-point of resuscitation: titrate the rate to maintain a urine output of 0.5-1 mL/kg/h, roughly 35-70 mL/h in this patient, via a catheter. Finally, list the parallel priorities you must not forget: assess and protect the airway (look for inhalation injury), give analgesia and tetanus prophylaxis, examine for circumferential burns that might need escharotomy, and recognise that a 45% burn clearly meets the criteria for referral to a specialist burns unit. Rehearsing this exact sequence — area, formula, end-point, airway, referral — turns a chaotic resuscitation into a checklist you can run under pressure.
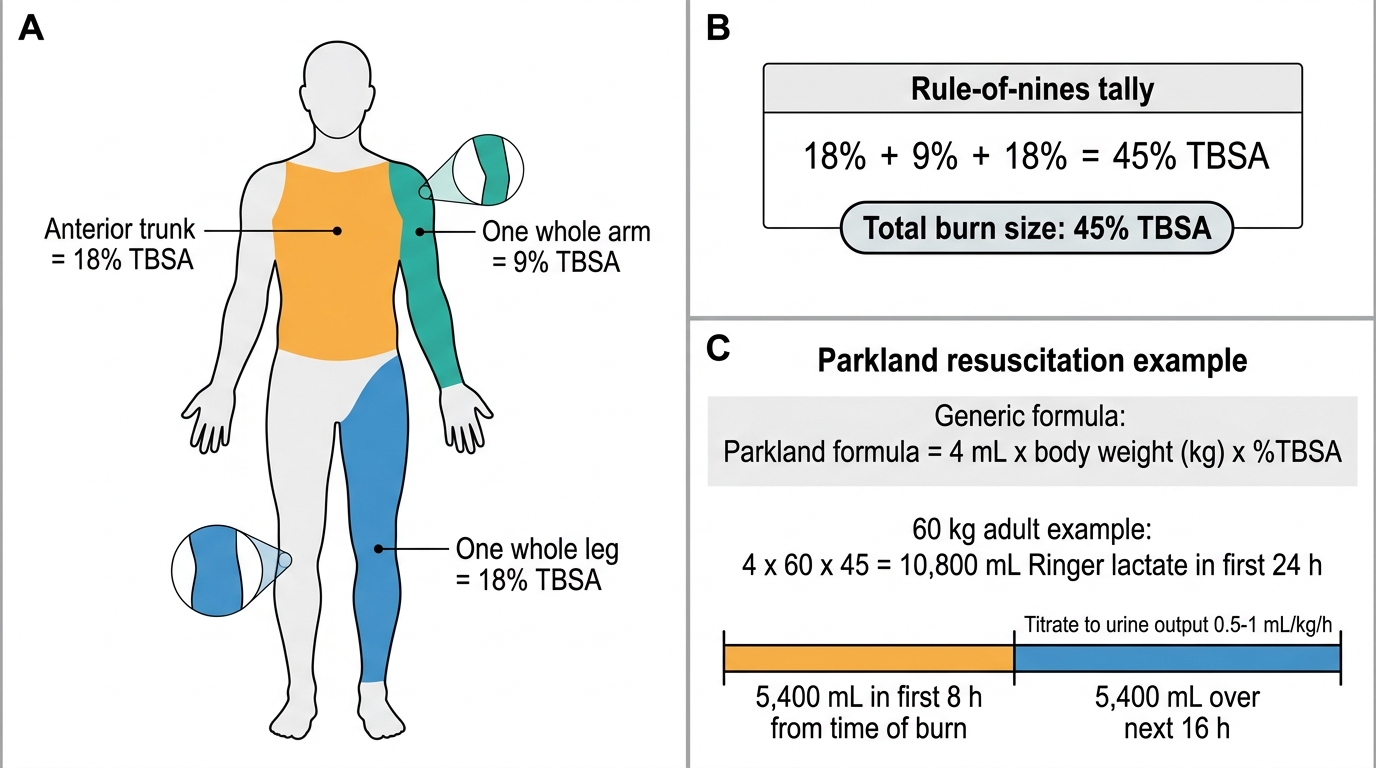
Rule of Nines and Parkland Calculation for 45% TBSA Burn
SELF-CHECK
A 60 kg adult has burns estimated at 30% TBSA from a flame injury. Using the Parkland formula, what is the total volume of Ringer's lactate for the first 24 hours, and how is it timed?
A. 3,600 mL total, all given evenly over 24 hours
B. 7,200 mL total, with half (3,600 mL) in the first 8 hours from the time of the burn and the rest over the next 16 hours
C. 7,200 mL total, with half in the first 8 hours from the time of hospital arrival
D. 14,400 mL total, with half in the first 8 hours from the time of the burn
Reveal Answer
Answer: B. 7,200 mL total, with half (3,600 mL) in the first 8 hours from the time of the burn and the rest over the next 16 hours
Parkland = 4 mL x kg x %TBSA = 4 x 60 x 30 = 7,200 mL of Ringer's lactate in the first 24 hours. Half (3,600 mL) is given in the first 8 hours measured from the TIME OF THE BURN, and the remaining half over the next 16 hours. Timing from arrival rather than from the burn under-resuscitates the patient; the rate is then titrated to a urine output of 0.5-1 mL/kg/h.