Page 7 of 17
SU24.1 | Pancreatitis — SDL Guide
Learning Objectives
- Describe the clinical features of acute pancreatitis and recognise its spectrum from a self-limiting illness to a life-threatening systemic catastrophe (SU24.1).
- Describe the aetiology and pathological basis of pancreatitis, including the autodigestion mechanism, the common causes, and the interstitial-versus-necrotising distinction (SU24.1).
- Describe the principles of investigation, severity assessment, prognosis and management of pancreatitis, including the supportive nature of early care and the role of antibiotics and surgery (SU24.1).
INSTRUCTIONS
Acute pancreatitis is one of surgery's great chameleons: the same diagnosis can mean a patient who is sore for a few days and home within the week, or a patient who slides into multi-organ failure on the intensive care unit. The gland digests itself, and how far that autodigestion spreads — confined oedema or extensive necrosis — largely decides the patient's fate. The clinical skills being built here are to make the diagnosis confidently from pain, enzymes and imaging; to grade severity early so the sick patient is recognised before they crash; and to manage by the principles that evidence actually supports — aggressive supportive care, no routine antibiotics in mild disease, treating the cause, and a restrained, step-up approach to the complications. Get the severity assessment right and the rest of the management follows.
References
- Bailey & Love's Short Practice of Surgery, The Pancreas (textbook)
- SRB's Manual of Surgery, Pancreas — Pancreatitis (textbook)
- Sabiston Textbook of Surgery, The Pancreas (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old man is brought to the emergency department doubled over with severe, boring epigastric pain that has bored straight through to his back over the last few hours, with relentless vomiting and a history of a heavy weekend's drinking. Two beds away, a 60-year-old woman with known gallstones has the same epigastric pain — but she is tachycardic, breathless, oliguric and confused, and her oxygen saturations are falling. Both have acute pancreatitis; the gland is digesting itself in each of them. Yet one will likely settle with fluids and analgesia over a few days while the other is on the edge of multi-organ failure and intensive care. The whole of pancreatitis management turns on telling these two patients apart early, treating the cause, and resisting the temptation to do too much too soon to a gland that mostly needs time and support to recover.
WHY THIS MATTERS
Pancreatitis matters because it is common, because its severity is deceptive, and because the wrong instincts can harm patients. Most attacks are mild and self-limiting, but the minority that turn severe carry a high mortality, and the early hours — when the patient may still look deceptively well — are exactly when aggressive fluid resuscitation and accurate severity scoring change outcomes. It also matters because pancreatitis is a topic where 'doing something' can be worse than supportive patience: routine antibiotics in mild disease, early CT at admission, and early open surgery for necrosis are all classic errors that good management avoids. For a final-year student, acute pancreatitis is a model of how to diagnose with a clear rule, grade with a validated score, and manage by the evidence — and a reminder that the surgeon's most important early actions here are resuscitation and assessment, not the knife.
RECALL
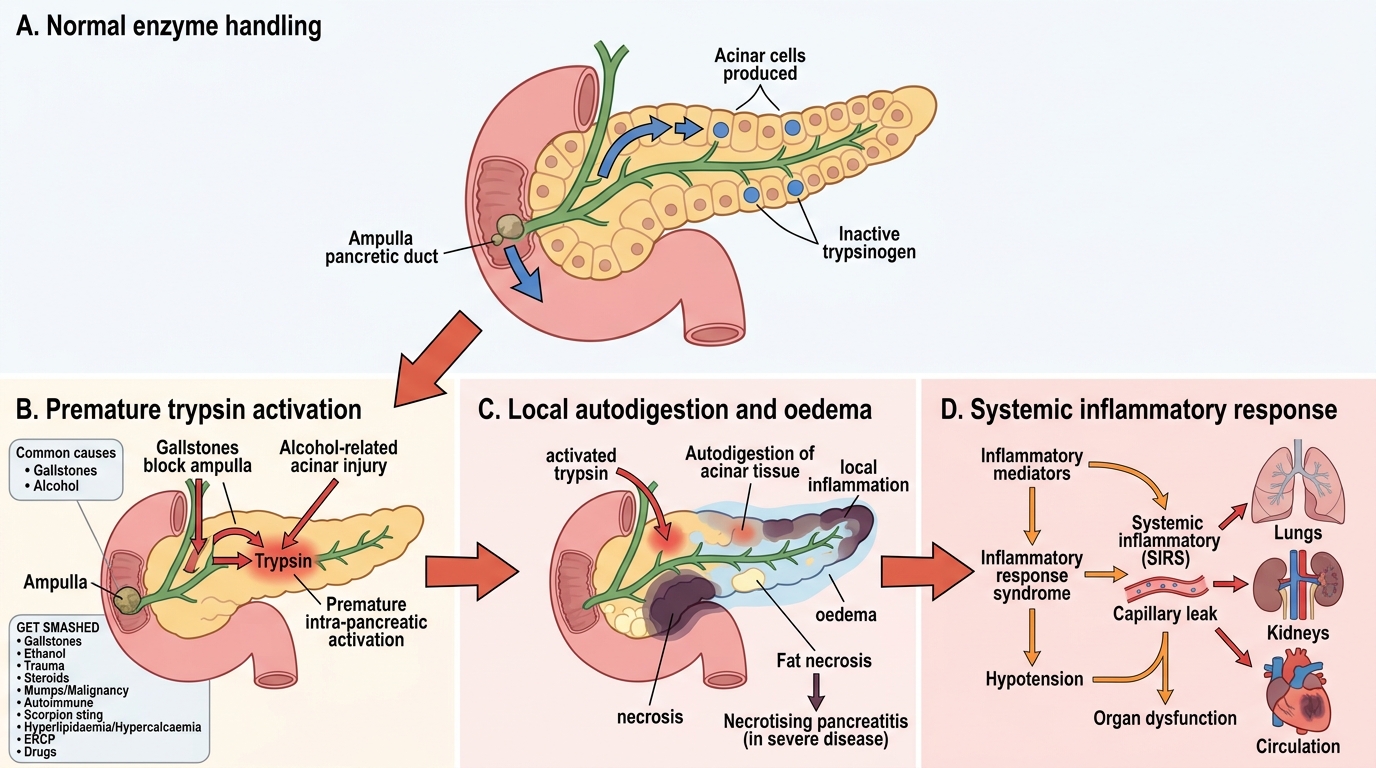
Recall the relevant pancreatic foundations before building on them. The pancreas is a retroperitoneal gland with both an exocrine function — acinar cells secreting digestive enzymes (including trypsinogen, lipase and amylase) into a ductal system draining to the duodenum — and an endocrine function from the islets of Langerhans. Crucially, the powerful digestive enzymes are normally secreted and stored as inactive precursors (zymogens) and are only activated in the duodenum, which protects the gland from digesting itself. Recall too that the common bile duct and the main pancreatic duct share a common channel at the ampulla of Vater, which is why a gallstone impacted there can obstruct pancreatic outflow and trigger pancreatitis. Hold on to one idea above all: pancreatitis is fundamentally a disease of premature, inappropriate activation of these enzymes inside the gland, leading to autodigestion — everything clinical flows from that single mechanism.
The Patient with Pancreatitis
Acute pancreatitis classically presents with severe, constant epigastric pain that radiates through to the back, often partially relieved by sitting forward, accompanied by nausea and vomiting that does not relieve the pain. The patient is typically distressed and may be tachycardic and dehydrated from vomiting and third-space fluid loss. The key clinical skill is to recognise that this single diagnosis spans a wide spectrum of severity. At the mild end, the patient is uncomfortable but systemically stable and settles over a few days. At the severe end, the autodigestive process drives a systemic inflammatory response that produces tachycardia, hypotension, tachypnoea and the features of organ dysfunction — respiratory compromise progressing towards acute respiratory distress syndrome (ARDS), acute kidney injury with oliguria, and circulatory shock. Examination may reveal epigastric tenderness and guarding, reduced bowel sounds from an associated ileus, and, in the small number with severe haemorrhagic necrotising disease, the classic but uncommon flank bruising (Grey Turner's sign) or periumbilical bruising (Cullen's sign). It is essential to distinguish this acute illness from chronic pancreatitis, a separate entity of long-standing, recurrent or persistent inflammation leading to irreversible fibrosis and to exocrine insufficiency (steatorrhoea) and endocrine insufficiency (diabetes), most commonly caused by alcohol and typically presenting with chronic pain, weight loss and malabsorption rather than an acute abdomen.
Aetiology and the Pathological Basis of Pancreatitis
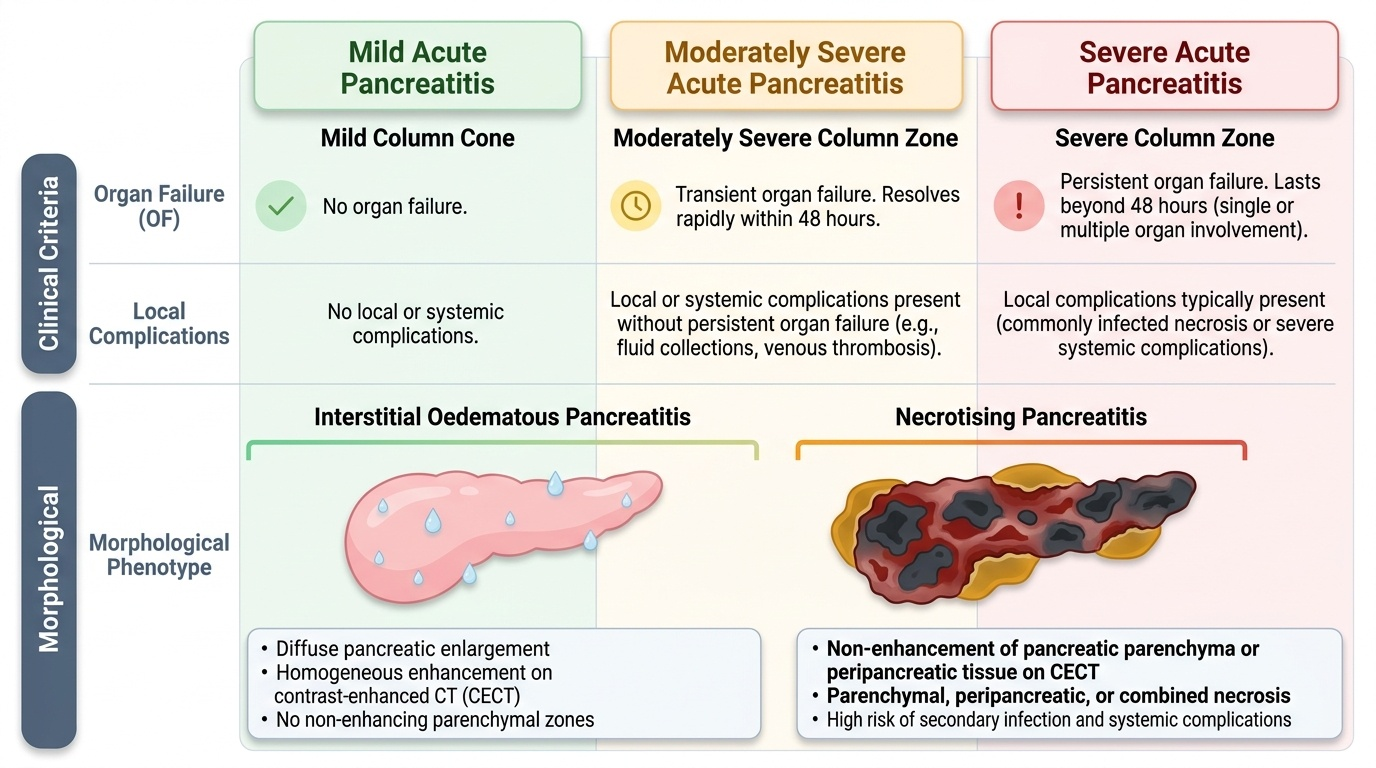
The central pathological event in pancreatitis is autodigestion: digestive enzymes that should be activated only in the duodenum are activated prematurely within the pancreas, and the gland begins to digest itself. Activated trypsin triggers a cascade activating other enzymes, lipase produces fat necrosis, and the inflammatory response causes oedema, vascular injury and, in severe cases, tissue death. The two commonest causes by far are gallstones (a stone obstructing the shared ampullary channel) and alcohol, and the full list of causes is captured by the well-known mnemonic GET SMASHED: Gallstones, Ethanol, Trauma, Steroids, Mumps (and other infections) / Malignancy, Autoimmune, Scorpion sting, Hyperlipidaemia / Hypercalcaemia / Hypothermia, ERCP, and Drugs. Pathologically, acute pancreatitis is divided by the revised Atlanta classification into two morphological types: interstitial oedematous pancreatitis, in which the gland is inflamed and oedematous but viable, which is the milder and far commoner form; and necrotising pancreatitis, in which there is death of pancreatic and/or peripancreatic tissue, which carries a much higher risk of complications and death, especially if the necrosis becomes infected. Chronic pancreatitis is a distinct, progressive process in which repeated injury (most often from alcohol) produces irreversible fibrosis, ductal changes and calcification with loss of both exocrine and endocrine function. Understanding that the disease ranges from confined oedema to widespread infected necrosis is what makes severity assessment meaningful.
Acute Pancreatitis: Trypsin Activation to Organ Dysfunction
- Commonest causes: gallstones and alcohol.
- GET SMASHED: Gallstones, Ethanol, Trauma, Steroids, Mumps/Malignancy, Autoimmune, Scorpion sting, Hyperlipidaemia/Hypercalcaemia/Hypothermia, ERCP, Drugs.
- Morphology (revised Atlanta): interstitial oedematous (mild, common) vs necrotising (severe, infection risk).
- Chronic pancreatitis: irreversible fibrosis → exocrine + endocrine insufficiency; usually alcohol.
SELF-CHECK
What is the central pathophysiological mechanism of acute pancreatitis, and what are its two commonest causes?
A. Bacterial infection of the gland; causes are E. coli and Klebsiella
B. Premature intra-pancreatic activation of digestive enzymes causing autodigestion; causes are gallstones and alcohol
C. Autoimmune destruction of islet cells; causes are type 1 diabetes and viral infection
D. Ischaemic infarction of the pancreas; causes are atherosclerosis and embolism
Reveal Answer
Answer: B. Premature intra-pancreatic activation of digestive enzymes causing autodigestion; causes are gallstones and alcohol
Acute pancreatitis results from premature, inappropriate activation of digestive enzymes (notably trypsin) within the pancreas, leading to autodigestion and inflammation. The two commonest causes are gallstones and alcohol (the 'G' and 'E' of GET SMASHED).
Examination, Investigation and Severity Assessment
The diagnosis of acute pancreatitis rests on a clear rule: it requires at least two of three features — characteristic epigastric pain radiating to the back, a serum amylase or lipase elevated to more than three times the upper limit of normal, and characteristic findings on cross-sectional imaging. Of the enzymes, lipase is more sensitive and specific than amylase and remains elevated for longer, so it is the better test where available; importantly, the height of the enzyme rise does NOT predict severity, so a 'very high amylase' is not the same as a 'very severe attack'. Because severity is what drives management and is not obvious at the bedside, every patient is graded with a validated severity score rather than by impression alone: the Glasgow (Imrie) score and Ranson's criteria combine clinical and laboratory variables to stratify risk, and a CRP greater than about 150 mg/L at 48 hours is a useful marker of severe disease. Severity is then formally categorised by the revised (modified) Atlanta classification into mild (no organ failure and no local or systemic complications), moderately severe (transient organ failure resolving within 48 hours, or local complications), and severe (persistent organ failure beyond 48 hours). A contrast-enhanced CT (CECT) is the best test to demonstrate and quantify pancreatic necrosis, but it is most informative when performed a few days into the illness (around 72–96 hours) rather than at admission, because necrosis takes time to declare itself; routine early CT at presentation adds little and can mislead. Baseline bloods (full blood count, urea and electrolytes, glucose, calcium, liver function and lactate dehydrogenase) feed the scoring systems and guide resuscitation, and an ultrasound is used early to look for gallstones as the cause.
Provided image
| Severity (revised Atlanta) | Organ failure | Complications |
|---|---|---|
| Mild | None | None |
| Moderately severe | Transient (<48 h) | Local complications or transient systemic features |
| Severe | Persistent (>48 h) | Often with local complications; high mortality |