Page 8 of 17
SU24.1 | Pancreatitis — SDL Guide (Part 2)
Principles of Management and Prognosis
The management of acute pancreatitis is, above all, supportive, because there is no drug that switches off the autodigestive process and the gland mostly needs time, resuscitation and organ support to recover. The early priorities are aggressive intravenous fluid resuscitation (the single most important early intervention, correcting the large third-space and vomiting losses and maintaining perfusion, titrated to urine output and physiology), effective analgesia, supplemental oxygen and monitoring, with severe cases managed in a high-dependency or intensive care setting. Nutrition matters: enteral feeding is preferred and is started early once tolerated rather than prolonged starvation. A key evidence-based principle is that antibiotics are NOT given routinely in mild acute pancreatitis and are reserved for proven or strongly suspected infection (particularly infected pancreatic necrosis) — prophylactic antibiotics for sterile disease are not beneficial. The underlying cause is treated: for gallstone pancreatitis, this means cholecystectomy (usually during the same admission once the attack settles in mild disease) and urgent ERCP if there is associated cholangitis or persistent biliary obstruction; for alcohol, abstinence and supportive care. Complications must be anticipated and are divided into local — acute fluid collections, pseudocyst (a collection of pancreatic fluid walled off by a non-epithelialised wall, usually maturing over about four weeks), walled-off necrosis, and infected necrosis — and systemic — SIRS, ARDS, acute kidney injury and shock. Infected pancreatic necrosis is the principal indication for intervention, and the modern approach is a restrained, escalating 'step-up' strategy (image-guided percutaneous or endoscopic drainage first, progressing to minimally invasive necrosectomy only if needed) rather than early open surgery, which carries high mortality. Prognosis depends chiefly on the development and persistence of organ failure and on infection of necrosis: mild interstitial disease usually recovers fully, whereas severe necrotising disease with persistent organ failure carries a substantial mortality.
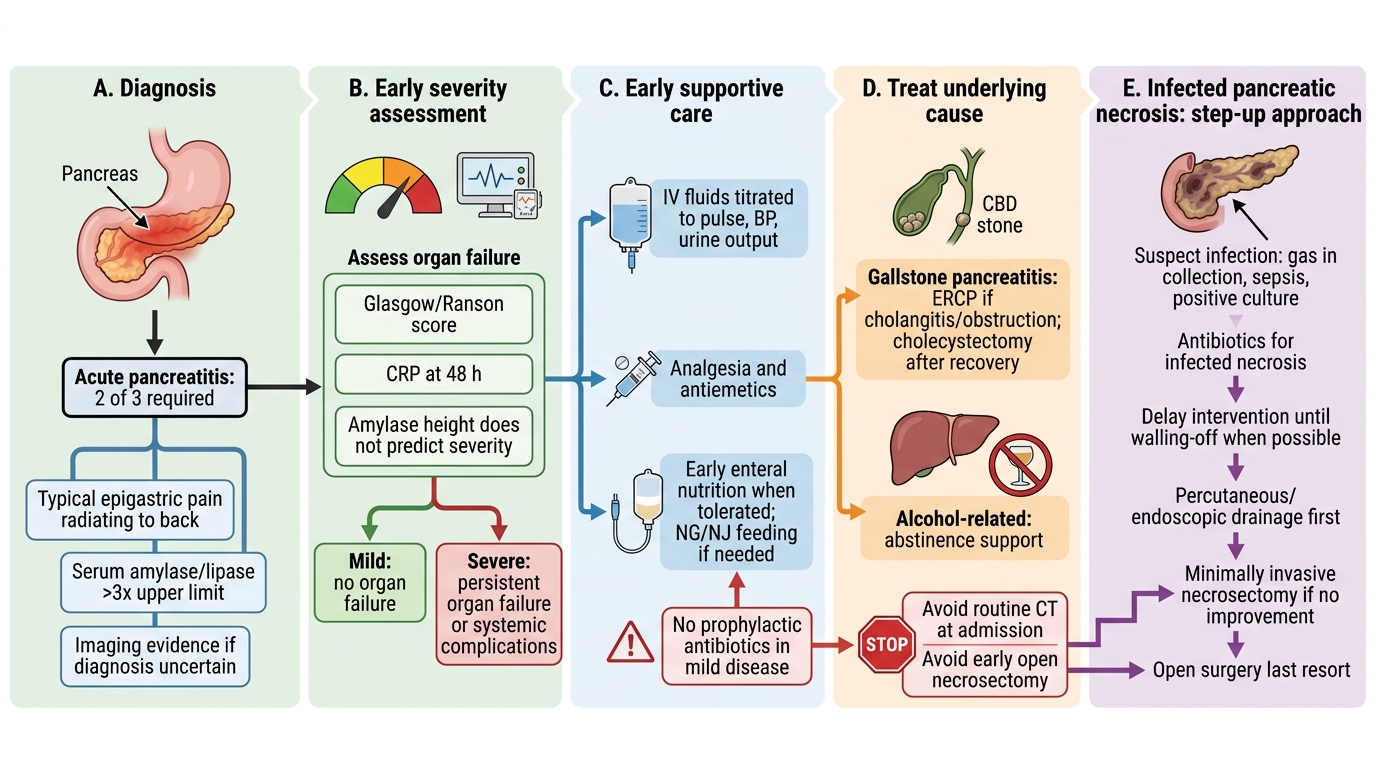
Acute Pancreatitis Management Flow
CLINICAL PEARL
Two reflexes save patients in acute pancreatitis. First, resuscitate aggressively and grade severity early — aggressive intravenous fluids titrated to physiology are the most important early intervention, and a validated score (Glasgow/Ranson, CRP at 48 h) identifies the sick patient before they crash. Second, resist over-treating: do NOT give prophylactic antibiotics in mild disease, do NOT rush to CT at admission (necrosis takes ~72–96 h to declare), and do NOT take necrosis to early open surgery — use a step-up drainage-first approach, reserving antibiotics and intervention for infected necrosis. The height of the amylase does not predict severity.
Check Your Understanding
Return to the two patients in the hook and reason through them with the framework. The 48-year-old man with alcohol-related epigastric pain radiating to the back and a raised lipase satisfies the two-of-three diagnostic rule; if his Glasgow score is low, his CRP stays below 150, and he has no organ failure, he has mild interstitial pancreatitis and needs fluids, analgesia, early enteral nutrition and abstinence — but no routine antibiotics and no early CT. The 60-year-old woman with gallstones who is tachycardic, breathless, oliguric and confused has the markers of severe disease with persistent organ failure: she needs intensive resuscitation in a critical-care setting, careful severity scoring, a CECT at the right time to assess necrosis, and treatment of her gallstone cause (cholecystectomy after recovery, urgent ERCP if cholangitis), with vigilance for infected necrosis managed by a step-up approach. Use these to self-test the competency this module covers. First, can you state the two-of-three diagnostic rule and explain why lipase is preferred and why enzyme height does not equal severity? Second, can you grade severity using a validated score and the revised Atlanta categories, and time the CECT correctly? Third, can you outline supportive management, the limited role of antibiotics, treatment of the cause, the local and systemic complications, and the step-up approach to infected necrosis? The questions that follow check exactly these links.
SELF-CHECK
Which statement about the management of acute pancreatitis is correct?
A. Prophylactic antibiotics should be given routinely to all patients with acute pancreatitis
B. Early management is mainly supportive (aggressive fluids, analgesia, nutrition); antibiotics are reserved for infected necrosis, not routine in mild disease
C. Necrotising pancreatitis should be treated with early open necrosectomy in all cases
D. A contrast-enhanced CT should always be performed at the moment of admission to grade severity
Reveal Answer
Answer: B. Early management is mainly supportive (aggressive fluids, analgesia, nutrition); antibiotics are reserved for infected necrosis, not routine in mild disease
Early management is supportive: aggressive fluid resuscitation, analgesia, oxygen and early enteral nutrition. Antibiotics are NOT routine in mild acute pancreatitis and are reserved for proven/suspected infection such as infected necrosis. Infected necrosis is managed by a step-up (drainage-first) approach rather than early open surgery, and CECT is most useful a few days into the illness, not at admission.