Page 7 of 20
SU27.4 | Gangrene and Amputation Principles — SDL Guide
Learning Objectives
- Describe the types of gangrene — dry, wet and special forms — and their surgical basis (SU27.4).
- Describe the principles of amputation, including its indications, the choice of level and the construction of a functional stump (SU27.4).
INSTRUCTIONS
Gangrene is tissue that has died and begun to decay, and it represents the visible end-point of the ischaemia and infection you have studied in arterial disease and the diabetic foot. The clinical tasks are to recognise which kind of gangrene you are dealing with — the slow, mummified, well-demarcated death of dry gangrene versus the spreading, septic, limb- and life-threatening process of wet gangrene — and to know when and how a limb or part must be amputated. This module connects the pathology of dry and wet gangrene and its special forms to the principles that govern amputation: treating the cause, deciding the indication, choosing the lowest level that will reliably heal, and building a stump that lets the patient walk again.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
An elderly man with longstanding peripheral arterial disease shows you his second and third toes: they are black, dry, shrivelled and painless, with a sharp line where the dead tissue meets healthy pink skin, and the changes have not advanced in weeks. Across the ward, a diabetic woman is acutely unwell — feverish, tachycardic and confused — with a swollen, dusky, blistered foot that smells foul, the discolouration creeping up towards her ankle by the hour. Both feet have gangrene, yet one is a stable problem you can plan around and the other is a surgical emergency that threatens her life unless the dead and infected tissue is removed today. Recognising which gangrene is in front of you, and knowing when a part must come off and at what level, is the core of this topic — and the difference between an unhurried operation and a race against sepsis.
WHY THIS MATTERS
Gangrene and amputation sit at the sharp end of vascular and diabetic surgery, and getting them right is a matter of saving lives and preserving function. Wet gangrene and gas gangrene are true emergencies in which delay allows sepsis to kill; dry gangrene, by contrast, can often be managed in a planned way once the underlying ischaemia has been addressed. The diabetic foot — a combination of neuropathy, ischaemia and infection — is one of the commonest reasons for limb loss in India and worldwide, and most amputations in diabetics are potentially preventable with earlier recognition and good foot care. When amputation is unavoidable, the level you choose determines whether the patient will walk again: a below-knee amputation that preserves the knee gives far better rehabilitation than an above-knee one. As a final-year student you must be able to classify gangrene, recognise the emergency forms, and state the principles that govern the timing, indication and level of amputation.
RECALL
Recall the foundations this builds on. From the occlusive arterial disease you have just studied: when arterial inflow falls far enough, tissue passes from rest pain to irreversible death — gangrene is the tissue-loss (Fontaine IV) end of that same spectrum, and acute limb ischaemia can produce gangrene within hours. From surgical infection and wound healing: necrotic, poorly perfused tissue is a perfect culture medium, so dead tissue plus bacteria gives spreading infection, and a stump will only heal if its blood supply is adequate. From microbiology, recall the clostridia — anaerobic spore-forming bacteria, of which Clostridium perfringens causes gas gangrene. Hold on to one unifying idea: gangrene is the convergence of two processes — ischaemia (loss of blood supply) and infection — and which of these dominates is exactly what separates dry from wet gangrene and dictates how urgently you must act.
The Patient with a Dead Toe or Foot
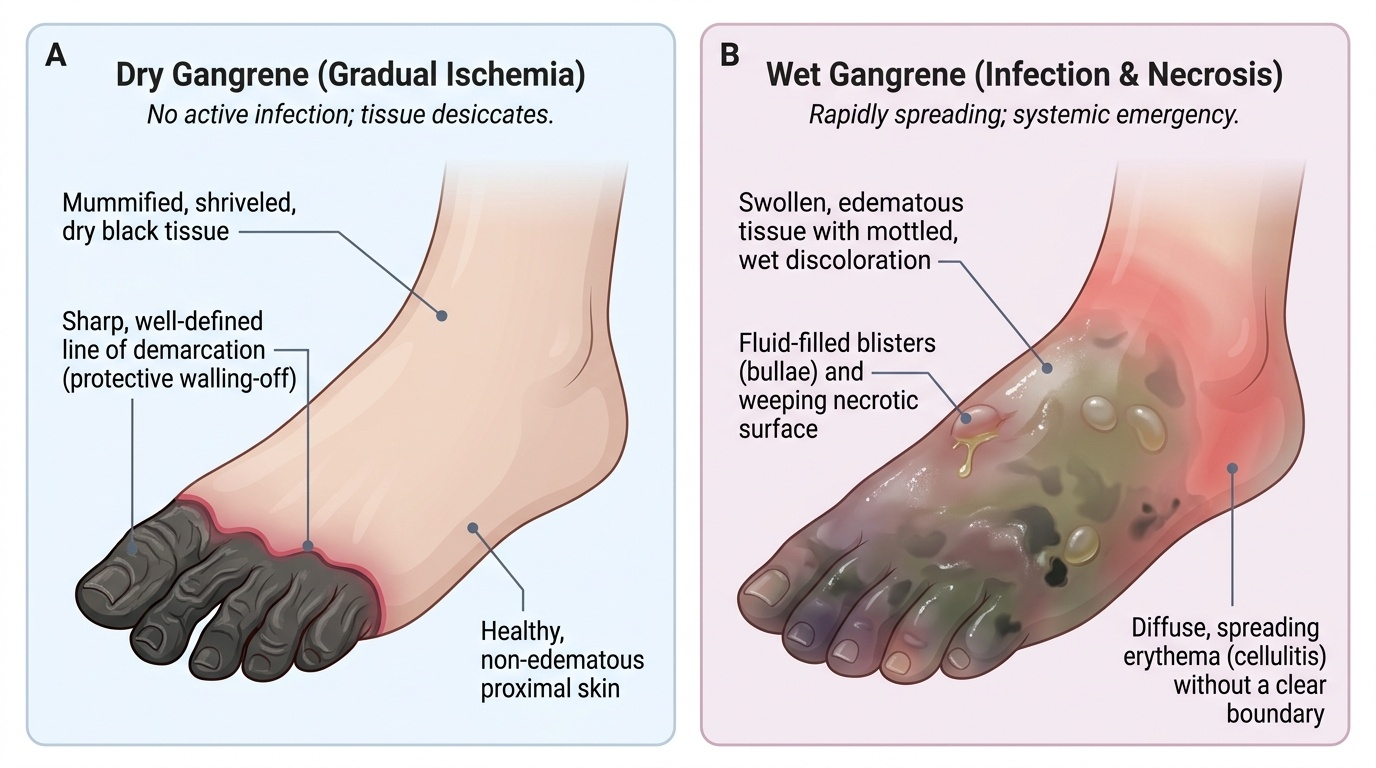
Gangrene presents as visibly dead tissue, and your first task at the bedside is to recognise which type it is, because the type dictates the urgency. Dry gangrene is the death of tissue from gradual arterial occlusion without superadded infection: the part — usually the toes or a distal foot — becomes cold, black, dry and shrivelled (mummified), is typically painless once the tissue is dead, and crucially shows a clear line of demarcation between the dead tissue and the viable, well-perfused skin above it; it tends to be stable rather than spreading. Wet gangrene is death of tissue with superadded infection (often with an element of venous as well as arterial obstruction): the part is swollen, discoloured, blistered, moist and foul-smelling, the changes spread proximally, there is surrounding cellulitis, and the patient is systemically unwell — febrile, tachycardic, even septic and confused. Wet gangrene is therefore an emergency. Two special situations must be recognised at once: gas gangrene, a clostridial myonecrosis with severe pain, crepitus (gas in the tissues), a thin discharge and profound toxaemia, demanding immediate surgery; and the diabetic foot, in which neuropathy (loss of protective sensation), ischaemia and infection combine, so that an apparently minor ulcer can progress rapidly to limb-threatening wet gangrene. Ask about diabetes, arterial disease, the speed of progression, pain, fever and the foot care the patient has had.
Types of Gangrene and their Surgical Basis
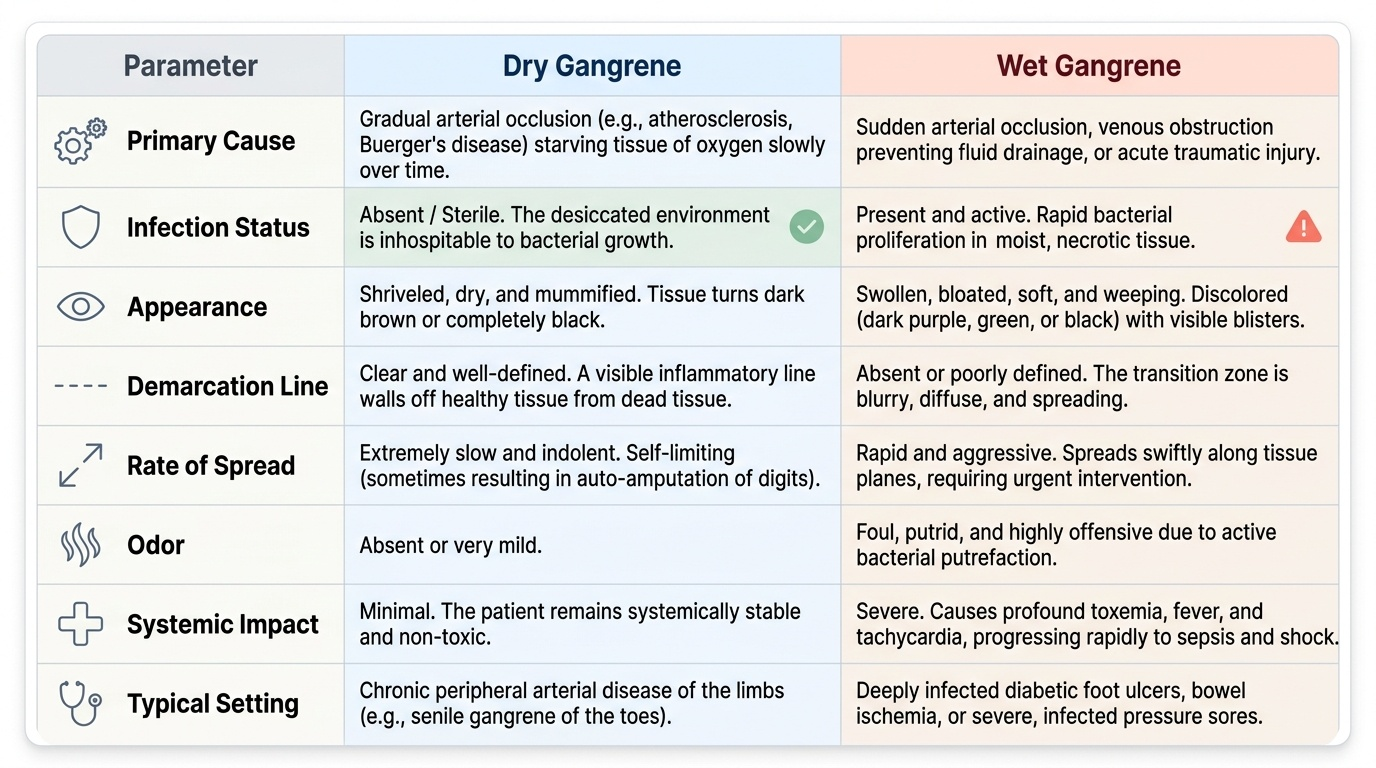
Gangrene means macroscopic death of tissue with subsequent putrefaction, and its surgical classification turns on the presence or absence of infection because that determines both the appearance and the urgency. In dry gangrene, gradual arterial occlusion (as in atherosclerotic peripheral arterial disease or Buerger's disease) starves the tissue slowly; without infection the dead part desiccates and mummifies, a protective line of demarcation forms as the body walls off the dead tissue, and the process is indolent — sometimes a dry gangrenous toe will even auto-amputate. In wet gangrene, the dead tissue becomes infected (and there is often coexisting venous obstruction preventing drainage), so bacteria proliferate in the moist necrotic tissue and spread along tissue planes; the part swells, blisters, weeps and smells, no clear line of demarcation forms, and the patient becomes toxic — untreated, this leads to overwhelming sepsis and death. The two important special forms are gas gangrene, clostridial (chiefly Clostridium perfringens) myonecrosis producing gas, toxaemia and rapid muscle death — a surgical emergency requiring aggressive debridement, high-dose antibiotics and resuscitation; and the diabetic foot, where the combination of peripheral neuropathy, peripheral arterial disease and impaired immunity allows ulcers to become deeply infected and gangrenous, frequently of the wet type. Recognising the type defines the surgical response: dry gangrene allows planned treatment of the underlying ischaemia, whereas wet and gas gangrene demand urgent removal of dead and infected tissue.
Provided image
Provided image
- Dry gangrene: gradual ischaemia, no infection; black, mummified, painless; clear line of demarcation; indolent.
- Wet gangrene: necrosis + infection (± venous obstruction); swollen, foul, spreading; systemically toxic; emergency.
- Gas gangrene: clostridial myonecrosis (C. perfringens); crepitus, toxaemia; surgical emergency.
- Diabetic foot: neuropathy + ischaemia + infection; minor ulcer → rapid limb-threatening (often wet) gangrene.
SELF-CHECK
Which set of features best describes DRY gangrene rather than wet gangrene?
A. Swollen, foul-smelling, spreading, with the patient systemically septic
B. Black, shrivelled and mummified, with a clear line of demarcation and no superadded infection
C. Crepitus, gas in the tissues and rapid muscle death
D. A painless ulcer with surrounding cellulitis tracking up the leg
Reveal Answer
Answer: B. Black, shrivelled and mummified, with a clear line of demarcation and no superadded infection
Dry gangrene results from gradual arterial occlusion WITHOUT superadded infection: the tissue desiccates and mummifies (black, shrivelled), a clear line of demarcation forms between dead and viable tissue, and it tends to be indolent rather than spreading. Swelling, foul smell, spread and systemic toxicity describe wet gangrene; crepitus and rapid muscle death describe gas gangrene.
Assessment and Investigation
Assessment has three aims: define the extent and type of gangrene, determine the viability and blood supply of the remaining tissue, and judge the patient's fitness for the operation that follows. Examine the dead area for its margins and for a line of demarcation, look for spreading infection (cellulitis, lymphangitis, crepitus suggesting gas), and assess the whole limb's perfusion — temperature, capillary refill and the peripheral pulses — because the level at which an amputation will heal depends on where there is enough blood supply. In a diabetic foot, specifically test protective sensation (the 10 g monofilament) to document neuropathy, probe the ulcer for depth and bony involvement, and assess the arterial supply (pulses, ABPI — remembering it can be falsely high in calcified diabetic vessels — and toe pressures). Investigations are then targeted: blood glucose and HbA1c and aggressive glycaemic control, full blood count, inflammatory markers, renal function and blood and wound cultures to guide antibiotics, and imaging — arterial duplex/CT/MR angiography to map vessels for possible revascularisation, and plain radiographs (and sometimes MRI) of the foot to detect osteomyelitis and tissue gas. The synthesis of these findings answers the operative questions: is this dry gangrene that can be planned, or wet/gas gangrene needing emergency debridement; can the limb be revascularised; and at what level will an amputation reliably heal?
- Examine: extent and line of demarcation, signs of spreading infection/crepitus, limb perfusion and pulses.
- Diabetic foot: 10 g monofilament for neuropathy, probe-to-bone, ABPI (may be falsely high) and toe pressures.
- Bloods/cultures: glucose and HbA1c, FBC, CRP, renal function, blood and wound cultures.
- Imaging: duplex/CT/MR angiography for revascularisation; foot X-ray/MRI for osteomyelitis and gas.