Page 8 of 20
SU27.4 | Gangrene and Amputation Principles — SDL Guide (Part 2)
Principles of Amputation
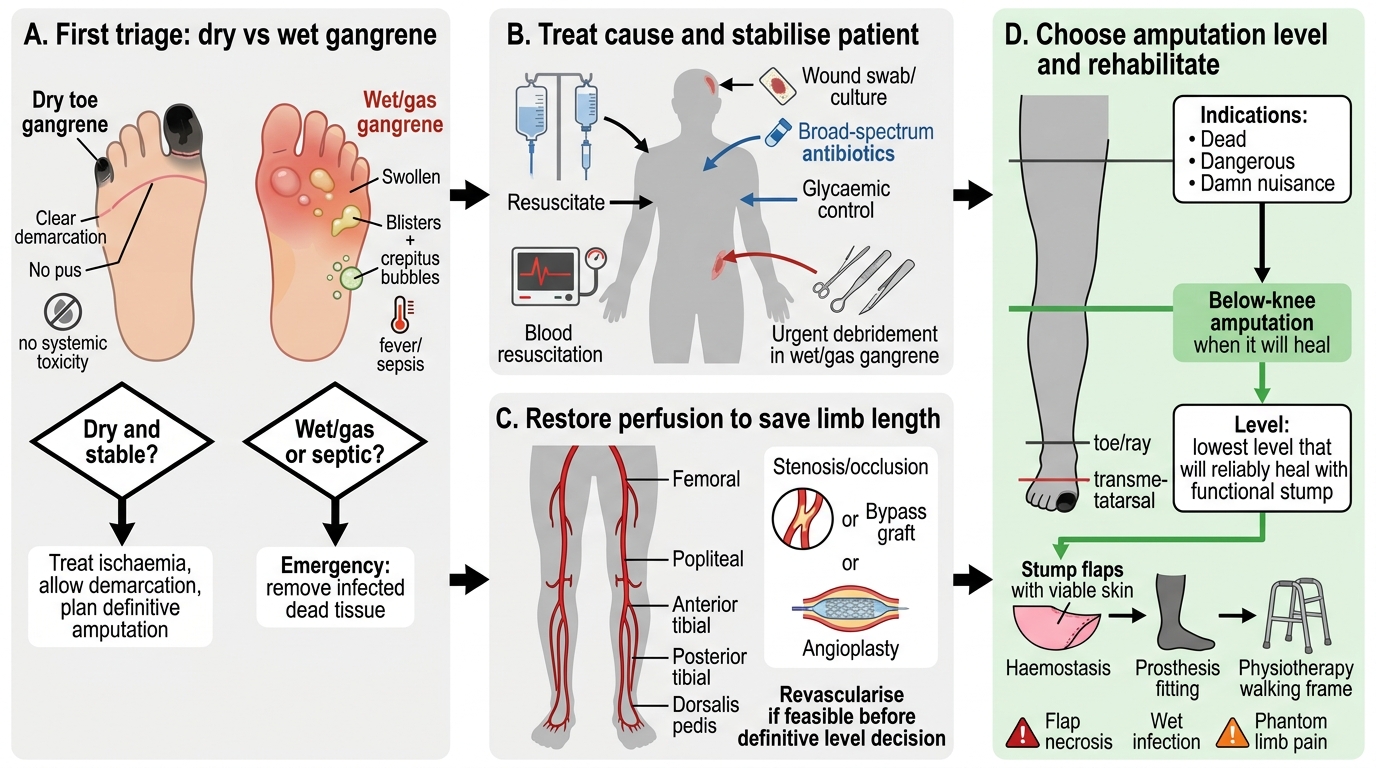
Before any amputation, the principle is to treat the cause and optimise the patient: control infection (urgent debridement and antibiotics in wet or gas gangrene), correct hyperglycaemia and resuscitate the septic patient, and revascularise wherever possible so that more of the limb can be saved and a lower amputation will heal. The classic indications for amputation are the three D's: Dead (the part is non-viable — irreversible ischaemia or established gangrene), Dangerous (the part threatens life — spreading wet or gas gangrene with sepsis, or malignancy), and Damn nuisance / useless (an intractably painful or non-functional limb that is worse than no limb). The cardinal rule of level selection is to amputate at the lowest level that will reliably heal while leaving a useful, functional stump: common levels ascend from toe and ray amputation, through transmetatarsal, to below-knee and above-knee amputation. Preserving the knee matters greatly — a below-knee amputation gives far better prosthetic mobility and rehabilitation than an above-knee one — so the surgeon balances the certainty of healing (which favours a higher level with better blood supply) against function (which favours the lowest viable level). The stump must be constructed for function: adequate length, healthy well-perfused muscle and skin flaps with the suture line away from pressure areas, secure haemostasis, and gentle handling to allow a prosthesis later. Complications to anticipate and consent for include stump infection or breakdown, flap necrosis (often meaning the level was too low), reactionary haemorrhage, phantom limb pain, and the longer-term challenge of rehabilitation. The goal throughout is not merely to remove dead tissue but to return the patient to walking.
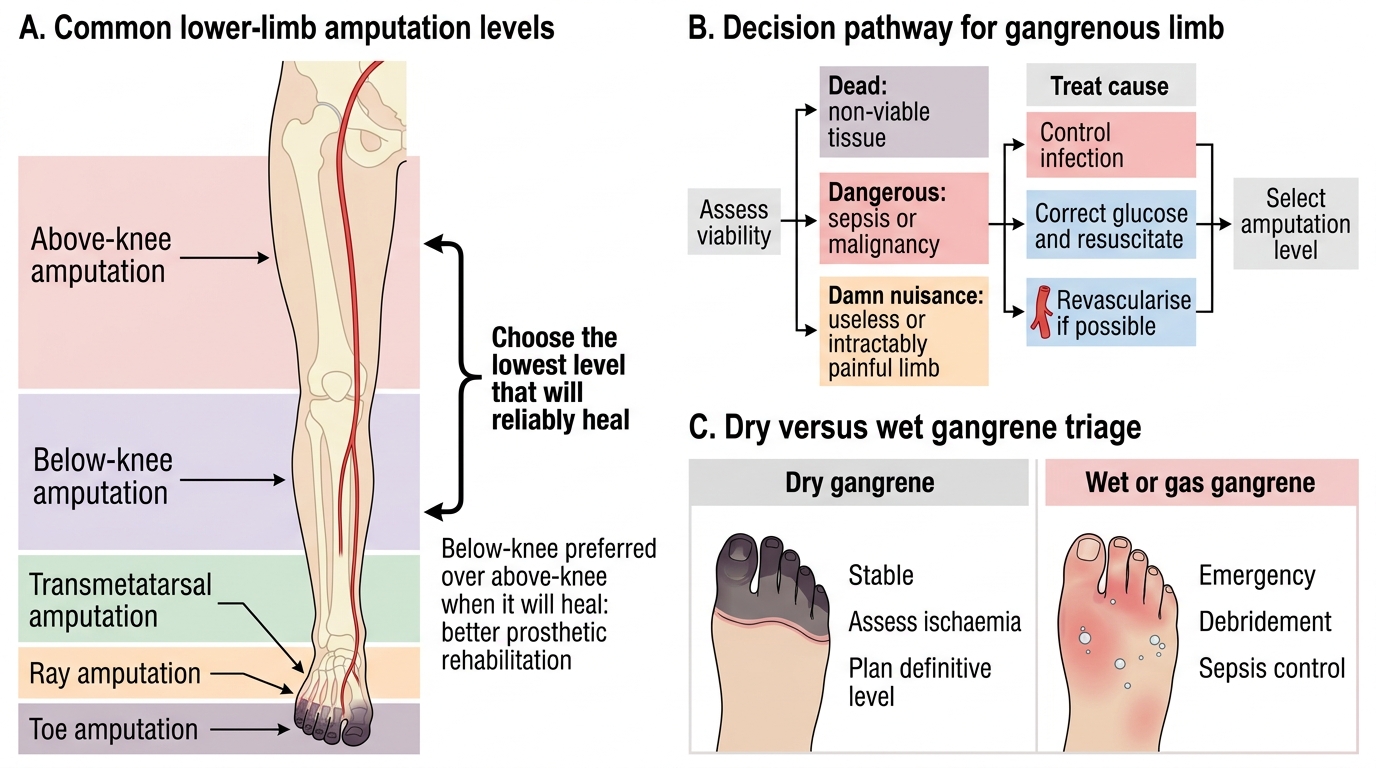
Common Lower-Limb Amputation Levels and Gangrene Decision Pathway
Decision Pathway for a Gangrenous Limb
- First, treat the cause: control infection (urgent debridement in wet/gas gangrene), correct glucose, resuscitate, revascularise to save limb length.
- Indications (the three D's): Dead (non-viable), Dangerous (life-threatening sepsis/malignancy), Damn nuisance (useless or intractably painful limb).
- Level: the lowest level that will reliably heal with a functional stump; below-knee preferred over above-knee for rehabilitation.
- Stump and aftercare: viable flaps, good length, haemostasis; watch for flap necrosis, infection, phantom limb pain; rehabilitate to a prosthesis.
CLINICAL PEARL
The single most important triage decision in gangrene is dry versus wet. DRY gangrene of a toe in a patient with peripheral arterial disease is usually stable: address the underlying ischaemia (consider revascularisation), let a clear line of demarcation form, and plan a definitive amputation at a level that will heal — it is rarely an emergency. WET (or gas) gangrene is the opposite: the spreading infection and systemic toxicity mean dead and infected tissue must be removed urgently (debridement or amputation), with resuscitation, antibiotics and glycaemic control, because delay allows fatal sepsis. Never wait for a line of demarcation in a septic, spreading wet foot — that delay can cost the patient their life, not just their leg.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The elderly man with black, dry, painless, well-demarcated gangrene of two toes and no systemic upset has dry gangrene on a background of peripheral arterial disease: he is not an emergency, so the plan is to assess and where possible revascularise the limb, allow the demarcation to mature, control risk factors, and then perform a planned amputation (toe or ray) at a level that will heal. The septic diabetic woman with a swollen, foul, spreading, blistered foot has wet gangrene: she needs urgent resuscitation, broad-spectrum antibiotics, glycaemic control and emergency debridement or amputation to remove the infected dead tissue and control sepsis — you cannot wait for demarcation. Use these to self-test the competency this module covers. First, can you describe and distinguish the types of gangrene — dry, wet, gas and the diabetic foot — and their surgical basis? Second, can you assess a gangrenous limb for type, viability, blood supply and fitness, and name the relevant investigations? Third, can you state the principles of amputation — treating the cause first, the three D indications, choosing the lowest level that will reliably heal, and why below-knee is preferred to above-knee? The questions below check exactly these links.
SELF-CHECK
When an amputation is unavoidable for lower-limb gangrene, what is the guiding principle for choosing the level, and why is below-knee generally preferred to above-knee?
A. Always amputate as high as possible to guarantee healing; the level does not affect rehabilitation
B. Amputate at the lowest level that will reliably heal with a functional stump; below-knee preserves the knee and gives far better prosthetic mobility
C. Choose the level by the patient's age alone
D. Amputate at the line of demarcation regardless of blood supply or infection
Reveal Answer
Answer: B. Amputate at the lowest level that will reliably heal with a functional stump; below-knee preserves the knee and gives far better prosthetic mobility
The cardinal principle is to amputate at the LOWEST level that will reliably heal while leaving a useful, functional stump — balancing certainty of healing (favouring a higher level with better blood supply) against function (favouring a lower level). Below-knee amputation is generally preferred to above-knee because preserving the knee joint markedly improves prosthetic walking and rehabilitation.