Page 7 of 14
SU28.8 | Pyloric Stenosis, Peptic Ulcer Disease and Carcinoma Stomach — SDL Guide
Learning Objectives
- Describe the aetiology, clinical features, investigations and principles of management of infantile (congenital) hypertrophic pyloric stenosis (SU28.8).
- Describe the aetiology, clinical features, investigations and principles of management of peptic ulcer disease and its complications (SU28.8).
- Describe the aetiology, clinical features, investigations and principles of management of carcinoma of the stomach (SU28.8).
INSTRUCTIONS
This module brings together three diseases of the stomach that share a location but almost nothing else: a self-limiting muscular obstruction of the neonate that is cured by a small operation; the acid-and-Helicobacter disease of adults that is mostly treated with tablets but kills through its complications; and an adenocarcinoma that too often declares itself only when it is already incurable. Treating them as one 'stomach' topic is the commonest error — each has its own age group, cause, cardinal investigation and management principle. The unifying skill is to read the presentation, choose the one investigation that confirms the diagnosis, and apply the correct principle of management — resuscitate-then-operate for the vomiting baby, eradicate-and-suppress (and operate for complications) for the ulcer, and stage-then-treat for the cancer.
References
- Bailey & Love's Short Practice of Surgery, The Stomach and Duodenum (textbook)
- SRB's Manual of Surgery, Stomach and Duodenum (textbook)
- Sabiston Textbook of Surgery, Stomach (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients, three stories, one organ. A worried mother brings her three-week-old first-born son who vomits forcefully after every feed — the milk shoots out, it is never green, and he is ravenously hungry minutes later, yet he is losing weight and his nappies are drying up. In the next cubicle, a 45-year-old man clutches his upper abdomen, rigid and grey, after a day of sudden severe epigastric pain that began like a stab; an X-ray shows a thin black crescent of air under his diaphragm. In clinic, a 62-year-old woman describes months of vague fullness, fading appetite and steady weight loss, and your hand finds a hard mass in her epigastrium. The same word — 'stomach trouble' — covers a curable muscular obstruction, a surgical emergency from a perforated ulcer, and a cancer. The work of this module is to keep them firmly apart.
WHY THIS MATTERS
Peptic ulcer disease, its complications and gastric carcinoma are among the most important conditions in general surgery, and infantile hypertrophic pyloric stenosis is the classic neonatal surgical emergency that every doctor must recognise. Getting these three right matters because the right action for each is completely different, and the wrong assumption is dangerous: rushing the vomiting baby to theatre before correcting his alkalosis risks a perioperative death; treating an older patient's 'dyspepsia' with acid suppression without endoscopy can let a curable gastric cancer become incurable; and missing the free gas under the diaphragm in a perforated ulcer delays a life-saving operation. For the student, these conditions are high-yield in examinations and, more importantly, are diseases you will genuinely meet — the projectile-vomiting baby, the acute abdomen, and the older patient with alarm symptoms — where a clear, disease-specific plan is what keeps the patient safe.
RECALL
Recall some foundations before we build on them. From physiology: the parietal (oxyntic) cells of the stomach secrete hydrochloric acid through the H+/K+ ATPase 'proton pump', stimulated by gastrin (from antral G cells), histamine and the vagus; the mucosa is normally protected by a mucus–bicarbonate barrier and prostaglandins. Peptic ulceration results when this balance tips toward aggression — chiefly from Helicobacter pylori infection and from NSAIDs (which inhibit protective prostaglandins). From anatomy: the pylorus is the muscular outlet of the stomach into the duodenum; hypertrophy of its circular muscle in the neonate obstructs gastric emptying. Recall too the metastatic signs introduced in the stomach-examination module — Virchow's node (Troisier's sign), the Sister Mary Joseph nodule and the Krukenberg tumour — because gastric carcinoma spreads by lymphatics and transcoelomically to produce exactly these. Hold on to acid physiology (for PUD) and the pyloric muscle (for pyloric stenosis); the cancer will draw on the examination signs you already know.
Three Different Patients, Three Different Diseases
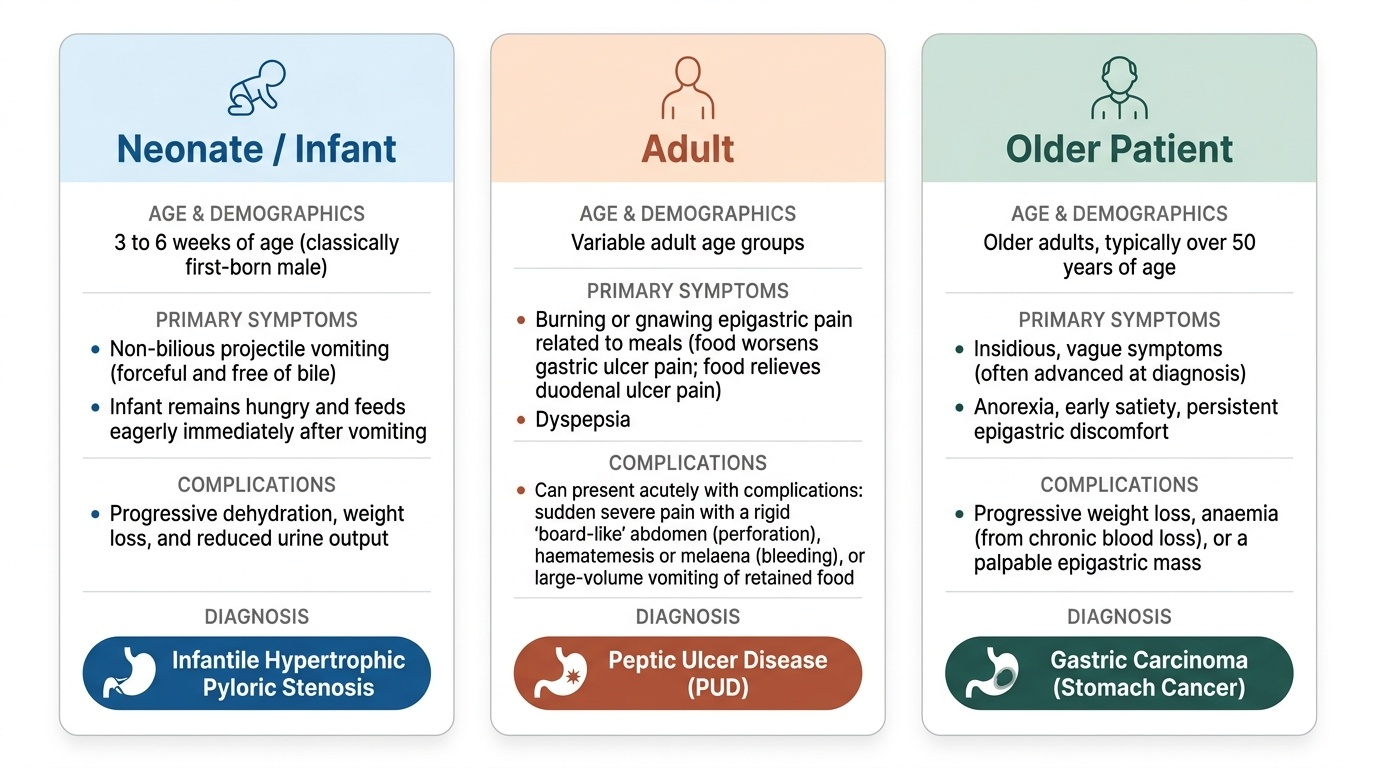
The three conditions of this competency present in three quite different ways, and recognising the pattern is the first step. Infantile hypertrophic pyloric stenosis presents in a baby, classically a first-born male at three to six weeks of age, with non-bilious projectile vomiting — the vomit is forceful and free of bile (because the obstruction is proximal to the bile duct's entry), and the infant remains hungry and feeds eagerly after vomiting. Progressive vomiting leads to dehydration, weight loss and reduced urine output. Peptic ulcer disease (PUD) presents in adults with epigastric pain — classically burning or gnawing, related to meals (duodenal ulcer pain is often relieved by food, while gastric ulcer pain may be worsened by it) — and dyspepsia; but it commonly first declares itself through a complication: sudden severe pain and a rigid 'board-like' abdomen from perforation, haematemesis or melaena from bleeding, or large-volume vomiting of retained food from gastric outlet obstruction caused by a scarred pyloric ulcer. Carcinoma of the stomach presents in older patients (usually over fifty) with insidious, vague symptoms — anorexia, early satiety, weight loss, persistent epigastric discomfort, and sometimes anaemia from chronic blood loss or a palpable epigastric mass; because the symptoms are non-specific, it is too often advanced at diagnosis. Reading these three patterns — the vomiting hungry baby, the adult with ulcer pain or an acute abdomen, and the older patient with weight loss — sets each patient on the correct diagnostic path.
Provided image
- Neonate, non-bilious projectile vomiting, hungry → infantile hypertrophic pyloric stenosis.
- Adult, ulcer-type epigastric pain or acute abdomen → peptic ulcer disease (± complication).
- Older patient, weight loss, early satiety, epigastric mass → gastric carcinoma.
Aetiology and Pathological Basis
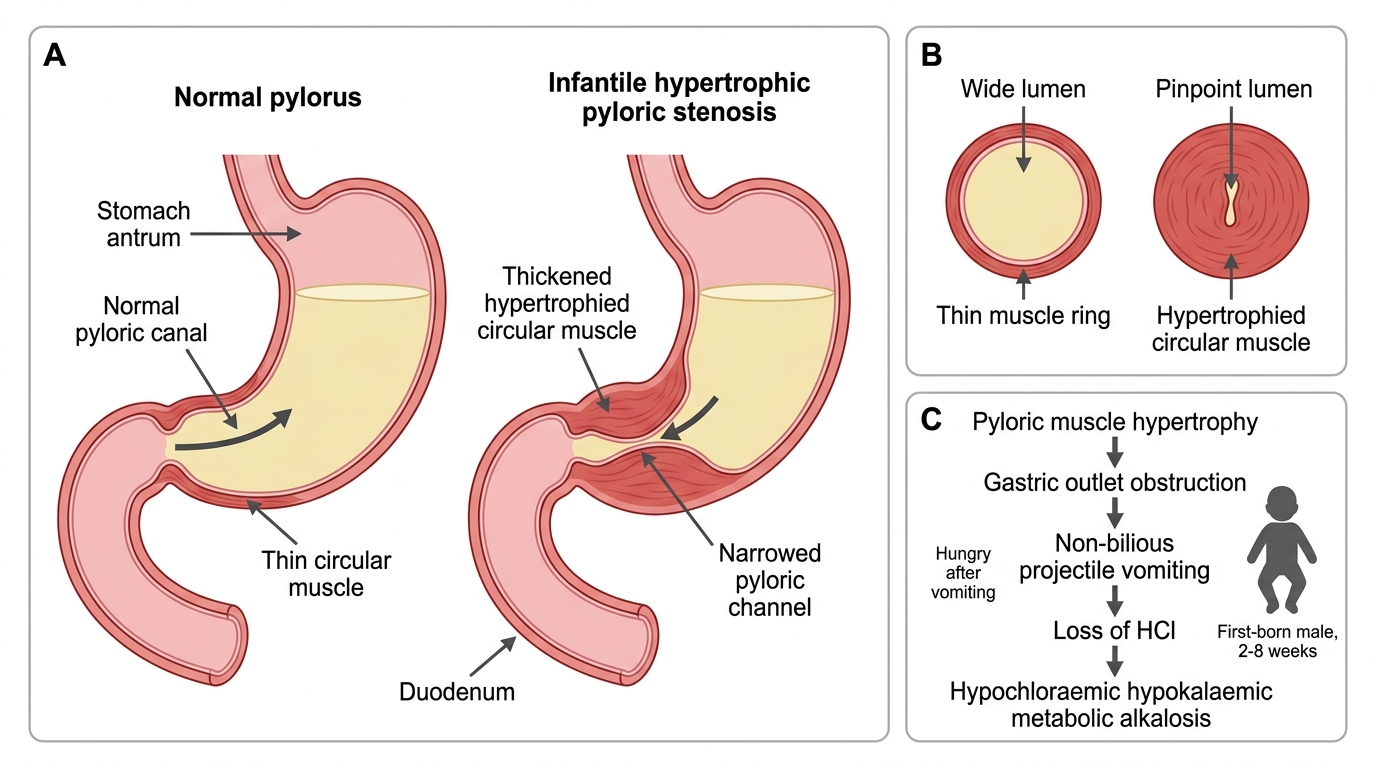
Each disease has a distinct pathological basis. In infantile hypertrophic pyloric stenosis, there is hypertrophy and hyperplasia of the circular smooth muscle of the pylorus, narrowing and elongating the pyloric channel so that the stomach cannot empty; the cause is multifactorial (genetic predisposition and other factors), and the obstruction produces persistent vomiting of acid-rich gastric contents. The resulting biochemical hallmark is a hypochloraemic, hypokalaemic metabolic alkalosis with paradoxical aciduria — the loss of hydrochloric acid in the vomit depletes chloride and hydrogen ions, and ongoing potassium loss compounds it; correcting this disturbance is central to safe management. Peptic ulcer disease is caused chiefly by Helicobacter pylori infection (which damages the mucosa and disturbs acid regulation) and by NSAIDs (which inhibit the prostaglandins that protect the mucosa); less commonly, marked acid hypersecretion (as in the gastrin-secreting tumours of Zollinger–Ellison syndrome) is responsible. Ulcers are gastric or duodenal, and their danger lies in eroding through the wall (perforation) or into a vessel (bleeding). Gastric carcinoma is almost always an adenocarcinoma, broadly of an intestinal type (gland-forming, linked to H. pylori-driven chronic atrophic gastritis and intestinal metaplasia, environmental and dietary factors) and a diffuse type (poorly cohesive signet-ring cells infiltrating the wall, which when extensive produces the rigid, contracted linitis plastica or 'leather-bottle' stomach). It spreads by direct invasion, by lymphatics (to Virchow's node), by blood (to the liver), and transcoelomically (to the umbilicus as a Sister Mary Joseph nodule and to the ovaries as a Krukenberg tumour).
Infantile Hypertrophic Pyloric Stenosis
- Pyloric stenosis: hypertrophy of pyloric circular muscle → outlet obstruction → hypochloraemic hypokalaemic metabolic alkalosis.
- PUD: H. pylori + NSAIDs (± Zollinger–Ellison); complications = perforation, bleeding, obstruction.
- Gastric carcinoma: adenocarcinoma — intestinal type vs diffuse (signet-ring, linitis plastica); spreads lymphatic/blood/transcoelomic.
SELF-CHECK
A 4-week-old first-born boy has non-bilious projectile vomiting and remains hungry. Which biochemical disturbance is most characteristic?
A. Hyperchloraemic metabolic acidosis
B. Hypochloraemic hypokalaemic metabolic alkalosis
C. High anion-gap metabolic acidosis
D. Respiratory alkalosis
Reveal Answer
Answer: B. Hypochloraemic hypokalaemic metabolic alkalosis
Infantile hypertrophic pyloric stenosis causes loss of hydrochloric acid in the vomitus, producing a hypochloraemic, hypokalaemic metabolic alkalosis (with paradoxical aciduria). Correcting this electrolyte and acid-base disturbance must precede surgery — the operation is not an emergency, resuscitation is the priority.
Investigation of the Three Disorders
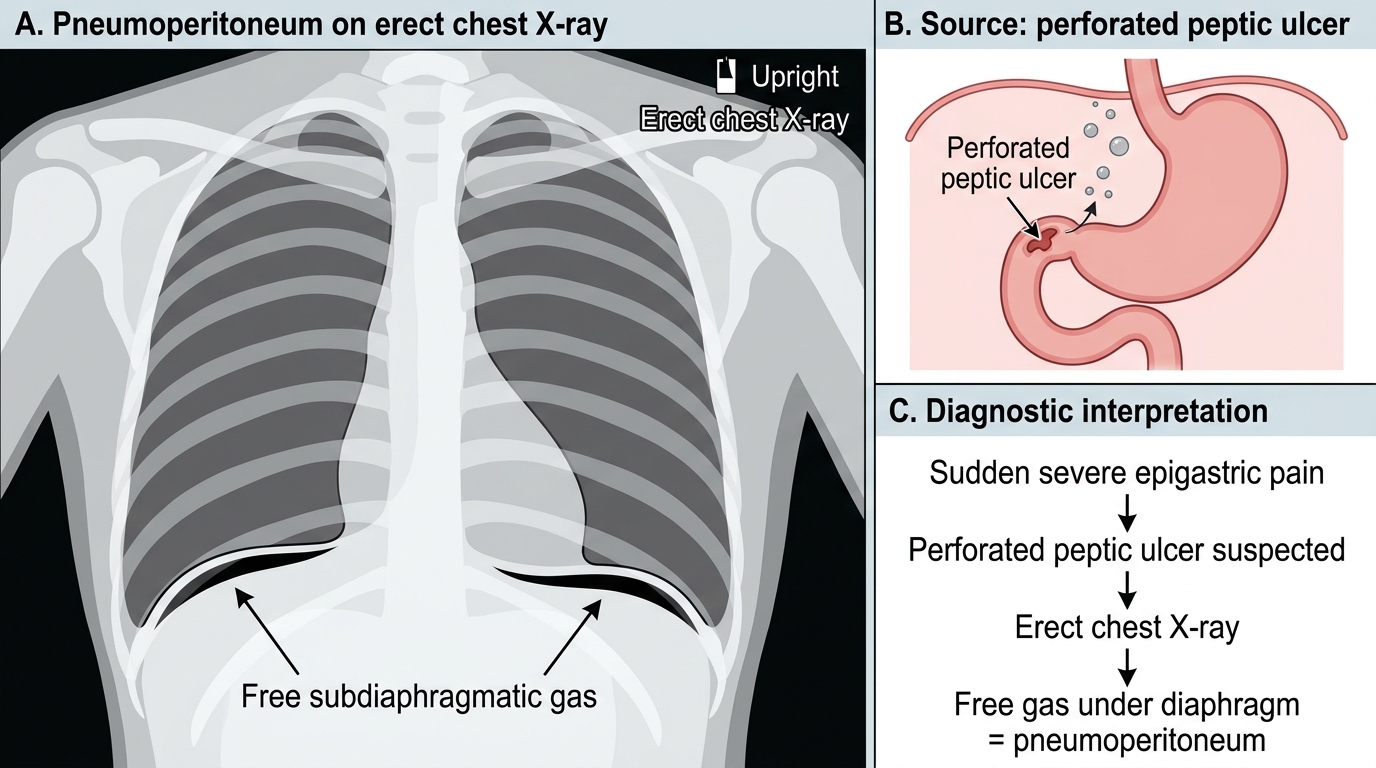
Each disease has one or two key investigations that confirm the diagnosis. For infantile hypertrophic pyloric stenosis, a careful test feed may reveal visible gastric peristalsis and a palpable, firm, olive-shaped pyloric 'tumour' (the palpable olive) in the right upper quadrant; the confirmatory test is abdominal ultrasound, which measures the thickened, elongated pyloric muscle. Equally important is to check serum electrolytes and a blood gas to identify and quantify the hypochloraemic hypokalaemic metabolic alkalosis that must be corrected before surgery. For peptic ulcer disease, upper gastrointestinal endoscopy is the key investigation — it visualises the ulcer, allows biopsy (mandatory for a gastric ulcer to exclude malignancy), and permits therapeutic haemostasis of a bleeding ulcer; testing for H. pylori (urea breath test, stool antigen, rapid urease test or histology on biopsy) guides eradication. In suspected perforation, an erect chest X-ray showing free gas under the diaphragm (pneumoperitoneum) confirms it, with CT for equivocal cases. For gastric carcinoma, endoscopy with biopsy establishes the tissue diagnosis, and CT of the chest, abdomen and pelvis (often with endoscopic ultrasound and, where available, diagnostic laparoscopy for peritoneal disease) stages the tumour to determine resectability.
Pneumoperitoneum in Perforated Peptic Ulcer
- Pyloric stenosis: test feed (palpable olive, visible peristalsis) + ultrasound (confirms); electrolytes/blood gas (alkalosis to correct).
- PUD: endoscopy + biopsy (gastric ulcers must be biopsied) + H. pylori testing; perforation → erect CXR (free gas).
- Gastric carcinoma: endoscopy + biopsy (diagnosis) + CT (± EUS, laparoscopy) (staging).