Page 8 of 14
SU28.8 | Pyloric Stenosis, Peptic Ulcer Disease and Carcinoma Stomach — SDL Guide (Part 2)
Principles of Surgical and Medical Management
Management follows directly from the diagnosis, and the guiding principle differs for each. In infantile hypertrophic pyloric stenosis, the cardinal rule is that the operation is not an emergency — resuscitation is. The infant is first rehydrated and the hypochloraemic hypokalaemic metabolic alkalosis is corrected with intravenous fluids and potassium; only once electrolytes and acid-base status are normal is the definitive procedure performed: a Ramstedt pyloromyotomy, in which the hypertrophied pyloric muscle is split down to (but not through) the mucosa, relieving the obstruction with an excellent prognosis. In peptic ulcer disease, most patients are managed medically — H. pylori eradication (a course of a proton pump inhibitor with two antibiotics) and acid suppression with a proton pump inhibitor, together with stopping NSAIDs. Surgery is now largely reserved for complications: a perforated ulcer is treated by resuscitation and operative closure, classically an omental (Graham) patch repair (open or laparoscopic) plus peritoneal lavage; a bleeding ulcer is treated first by endoscopic haemostasis, with surgery for failure; and gastric outlet obstruction from scarring may need drainage or resection. In gastric carcinoma, the principle is stage, then treat with curative intent only when resectable: localised, operable disease is treated by gastrectomy (partial or total) with D2 lymphadenectomy, usually combined with perioperative chemotherapy, while advanced disease — signalled by the metastatic signs or by imaging — is treated palliatively (chemotherapy, relief of obstruction or bleeding, and nutritional support). The recurring theme is that one organ demands three quite different strategies.
Provided image
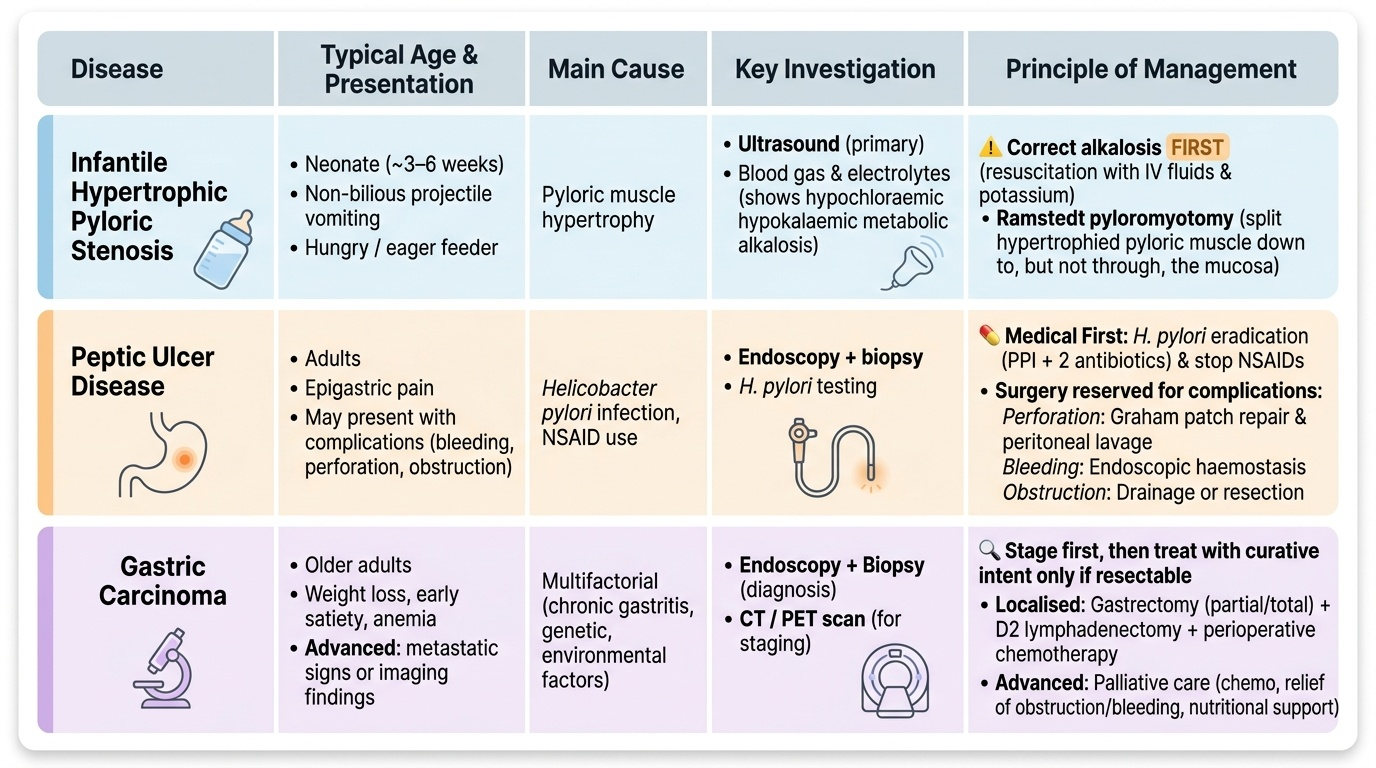
| Disease | Typical age & presentation | Main cause | Key investigation | Principle of management |
|---|---|---|---|---|
| Infantile hypertrophic pyloric stenosis | Neonate ~3–6 wk; non-bilious projectile vomiting, hungry | Pyloric muscle hypertrophy | Ultrasound (+ electrolytes/blood gas) | Correct alkalosis FIRST, then Ramstedt pyloromyotomy |
| Peptic ulcer disease | Adults; epigastric pain or a complication | H. pylori, NSAIDs | Endoscopy + biopsy + H. pylori test | Eradication + PPI; surgery (Graham patch) for perforation |
| Gastric carcinoma | >50 yr; weight loss, mass, anaemia | Adenocarcinoma (intestinal/diffuse) | Endoscopy + biopsy + CT staging | Gastrectomy + D2 ± chemo if resectable; else palliation |
CLINICAL PEARL
In the projectile-vomiting baby, the most dangerous mistake is to treat infantile hypertrophic pyloric stenosis as a surgical emergency and rush to theatre. It is a MEDICAL emergency first: the hypochloraemic hypokalaemic metabolic alkalosis must be corrected with intravenous fluids and potassium before any anaesthetic, because operating on an alkalotic, dehydrated infant risks apnoea and arrhythmia. The pyloromyotomy itself is elective once the biochemistry is normal. Remember the rule: resuscitate first, operate second.
Check Your Understanding
Bring the threads together by reasoning back through the three patients in the hook. The three-week-old first-born boy with non-bilious projectile vomiting who stays hungry has infantile hypertrophic pyloric stenosis: confirm with ultrasound (and palpate the olive), check the hypochloraemic hypokalaemic metabolic alkalosis, correct it first, then perform a Ramstedt pyloromyotomy. The 45-year-old with sudden severe pain, a rigid abdomen and free gas under the diaphragm has a perforated peptic ulcer: resuscitate and repair, classically with a Graham omental patch, and treat the underlying H. pylori. The 62-year-old with months of weight loss and an epigastric mass has gastric carcinoma: endoscopy and biopsy for the diagnosis, CT to stage, and curative gastrectomy with D2 lymphadenectomy only if resectable — otherwise palliation. Use these to self-test the competency. First, can you give the aetiology, cardinal clinical features, key investigation and management principle for each of the three conditions, keeping them distinct? Second, can you state the characteristic biochemical disturbance of pyloric stenosis and why resuscitation precedes surgery? Third, can you describe the complications of peptic ulcer disease and how each is managed, and outline the types and spread of gastric adenocarcinoma? The questions that follow check exactly these links.
SELF-CHECK
A 45-year-old presents with sudden severe epigastric pain, a board-like rigid abdomen and free gas under the diaphragm on an erect chest X-ray. What is the diagnosis and the classic operative repair?
A. Acute pancreatitis; conservative management
B. Perforated peptic ulcer; omental (Graham) patch repair
C. Gastric outlet obstruction; gastrojejunostomy
D. Bleeding peptic ulcer; partial gastrectomy
Reveal Answer
Answer: B. Perforated peptic ulcer; omental (Graham) patch repair
Sudden severe pain with a rigid abdomen and pneumoperitoneum (free gas under the diaphragm) indicates a perforated peptic ulcer. After resuscitation, the classic repair is an omental (Graham) patch closure (open or laparoscopic) with peritoneal lavage, plus treatment of the underlying H. pylori.
SELF-CHECK
Which feature is characteristic of the DIFFUSE type of gastric adenocarcinoma?
A. Gland-forming intestinal-type histology
B. Signet-ring cells infiltrating the wall, producing linitis plastica
C. Arising only from Barrett's metaplasia
D. Spread exclusively by the bloodstream
Reveal Answer
Answer: B. Signet-ring cells infiltrating the wall, producing linitis plastica
The diffuse type of gastric adenocarcinoma is composed of poorly cohesive signet-ring cells that infiltrate the wall; when extensive it produces the rigid, contracted 'leather-bottle' stomach (linitis plastica). The intestinal type is gland-forming and linked to chronic atrophic gastritis with intestinal metaplasia.