Page 7 of 26
SU29.2 | Congenital Genitourinary Anomalies — SDL Guide
Learning Objectives
- Describe the clinical features of the major congenital anomalies of the genitourinary system across their typical age at presentation (SU29.2).
- Explain the embryological basis and pathology of pelviureteric junction obstruction, posterior urethral valves, vesicoureteric reflux, hypospadias and undescended testis (SU29.2).
- Outline the investigation of a suspected congenital genitourinary anomaly — antenatal and postnatal ultrasound, micturating cystourethrogram, DMSA and MAG3 renography — and the principles of surgical management (SU29.2).
INSTRUCTIONS
Congenital anomalies of the genitourinary tract are among the commonest structural birth defects, and most are now suspected before birth on antenatal ultrasound. They matter because the kidney is unforgiving: an obstruction or reflux that goes unrecognised in infancy can quietly destroy renal function for life, while the same lesion treated early is usually compatible with normal kidneys. This module connects the embryology and pathology of the major anomalies to the way they present, the orderly imaging work-up that confirms them, and the surgical principles that relieve obstruction, preserve renal function, prevent infection and reconstruct. Two operative cautions run through it and must never be forgotten: posterior urethral valves are a disease of the male newborn, and the foreskin must be preserved — never circumcised — in a boy with hypospadias because it is needed for the repair.
References
- Bailey & Love's Short Practice of Surgery, The Urinary Bladder, Prostate, Kidney and Ureter / Paediatric Urology (textbook)
- SRB's Manual of Surgery, Urology — Congenital Anomalies of the Urogenital Tract (textbook)
- Sabiston Textbook of Surgery, Pediatric Surgery — Urologic Disorders (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In the neonatal unit two babies are referred to surgery on the same morning. The first is a boy, just a few days old, whose mother noticed that he dribbles rather than passes a proper stream, and whose lower abdomen carries a smooth, palpable swelling that the resident realises is a distended bladder; his antenatal scans had shown both kidneys to be dilated and the fluid around him to be scanty. The second baby is a girl whose antenatal scan flagged a single swollen kidney on one side, but who now feeds and voids without any obvious trouble. The same broad heading — 'congenital genitourinary anomaly' — yet one of these infants faces a urological emergency that threatens his kidneys and even his lungs, while the other can be watched along a careful, mostly non-operative path. Telling these stories apart, quickly and safely, is the whole purpose of this module.
WHY THIS MATTERS
Congenital genitourinary anomalies are common, frequently silent, and capable of causing irreversible harm if missed — which is exactly why a surgeon must recognise them. The kidney has no way of announcing slow damage: obstruction at the pelviureteric junction, valves blocking the male urethra, or urine refluxing up to the kidney with every infection can erode nephrons for months before anyone notices, and lost renal function does not come back. The flip side is genuinely hopeful: the very same lesions, picked up on an antenatal scan and treated in infancy, are usually compatible with normal kidneys and a normal life. For external genital anomalies the stakes are different but no less important — a correctly timed hypospadias repair or orchidopexy protects continence, fertility and body image, whereas a wrong early move (most notoriously circumcising a boy with hypospadias) can sabotage the definitive operation. For a final-year student these conditions are also high-yield: antenatal hydronephrosis, the male neonate who cannot void, the toddler with recurrent urinary infections, and the empty scrotum are classic clinical and viva scenarios.
RECALL
Recall a few foundations before building on them. From embryology and anatomy: the kidney drains through the renal pelvis into the ureter at the pelviureteric junction (PUJ), the ureter enters the bladder obliquely at the ureterovesical junction (an oblique tunnel that normally acts as a one-way flap valve preventing reflux), and the bladder empties through the urethra — which in the male passes through the prostatic (posterior) urethra. From physiology: glomerular filtration depends on unobstructed outflow and on a clean, low-pressure system; any back-pressure or stasis both damages nephrons directly and invites infection. Hold on to two ideas in particular. First, hydronephrosis — dilatation of the renal pelvis and calyces — is the common radiological signature shared by obstruction and high-grade reflux, so finding it tells you where to look, not yet what is wrong. Second, the developing foreskin (prepuce) and the urethral plate on the under-surface of the penis are the raw material a paediatric urologist later uses to reconstruct a hypospadiac urethra — which is why their preservation is built into early decision-making.
The Child Presenting with a Genitourinary Anomaly
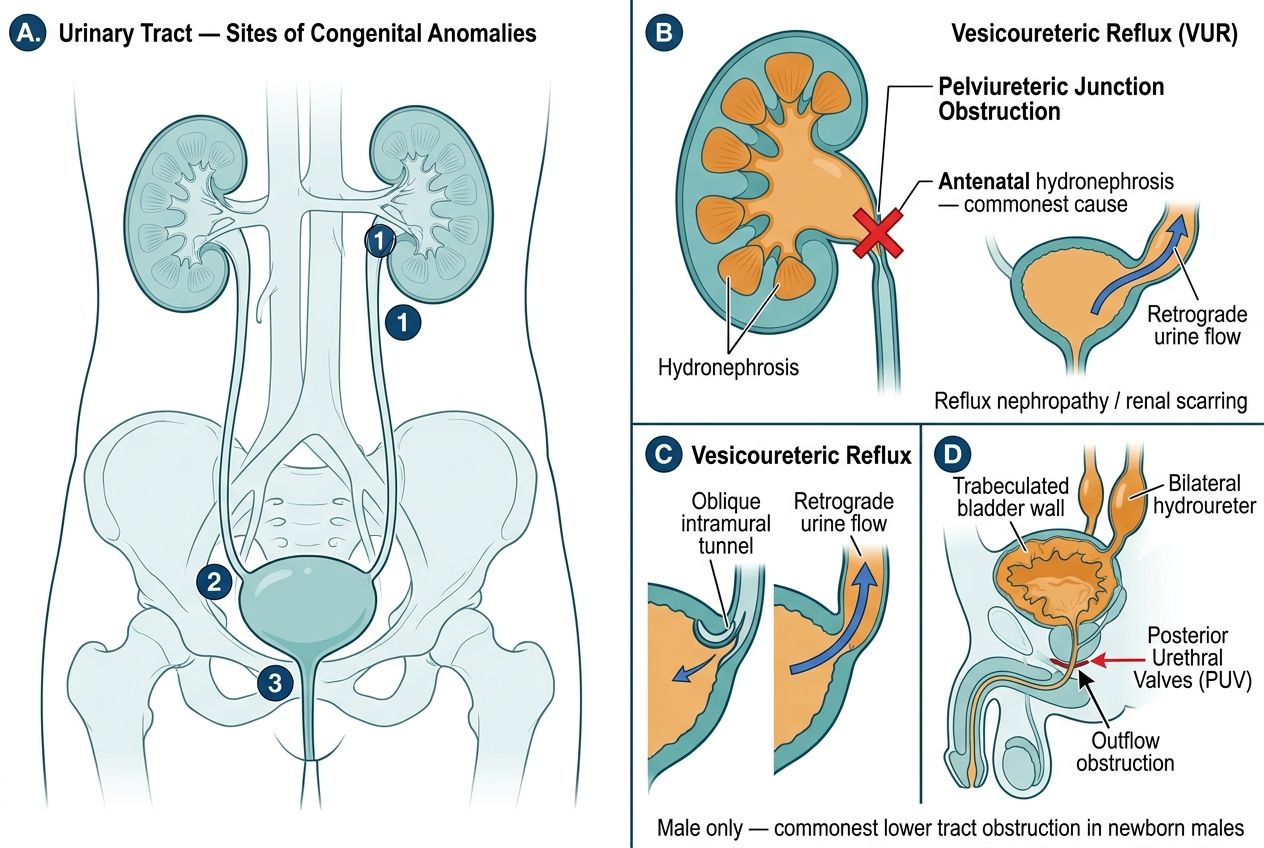
Congenital genitourinary anomalies announce themselves in a small number of recognisable ways, and matching the presentation to the likely lesion is the first clinical skill. Increasingly the earliest clue is antenatal hydronephrosis — a dilated renal pelvis seen on the routine antenatal ultrasound — which is the commonest reason these children reach a surgeon at all; the commonest cause of isolated antenatal hydronephrosis is pelviureteric junction (PUJ) obstruction. After birth, the single most urgent presentation is the male neonate who cannot void normally: a poor or dribbling urinary stream, a distended palpable bladder, and bilateral antenatal hydronephrosis (often with reduced liquor, oligohydramnios) point to posterior urethral valves (PUV), the commonest cause of lower urinary tract obstruction in male newborns and a urological emergency. A little later, the toddler with recurrent urinary tract infections, particularly febrile infections, should raise the question of vesicoureteric reflux (VUR). Beyond the urinary tract, two external genital presentations are unmistakable on the newborn check: hypospadias, recognised by an abnormally sited (ventral) urethral opening with a hooded, incomplete foreskin and a downward bend of the penis, and the empty scrotum of an undescended testis. The rarer but dramatic exstrophy-epispadias complex presents at birth with the bladder open on the lower abdominal wall. The older child with intermittent loin pain provoked by a large fluid load — Dietl's crisis — is the classic late presentation of PUJ obstruction. Reading these patterns correctly directs both the urgency and the imaging that follows.

Provided image
- Antenatal hydronephrosis (commonest first clue) → most often PUJ obstruction; also VUR, PUV, duplex systems.
- Male neonate, poor stream + palpable bladder + bilateral hydronephrosis ± oligohydramnios → posterior urethral valves (emergency).
- Toddler with recurrent (febrile) UTIs → vesicoureteric reflux.
- Ventral urethral meatus + chordee + hooded prepuce → hypospadias; empty scrotum → undescended testis.
Embryological Basis and Pathology of the Major Anomalies
Each anomaly is best understood as a fault at a particular level of the developing urinary or genital tract, and the level dictates both the imaging signature and the operation. At the renal pelvis, an intrinsic narrowing or an abnormal muscular segment at the pelviureteric junction impedes drainage, so urine backs up and the pelvis and calyces dilate — PUJ obstruction, the commonest cause of antenatal hydronephrosis. At the ureterovesical junction, a short or abnormally straight intramural ureteric tunnel fails as a flap valve, so urine refluxes retrograde toward the kidney during voiding — vesicoureteric reflux (VUR); the danger is not the reflux itself but the delivery of infected, high-pressure urine to the kidney, producing pyelonephritic scarring (reflux nephropathy) and, in time, hypertension and chronic kidney disease. In the posterior (prostatic) urethra of the male, persistent membranous folds — posterior urethral valves — obstruct outflow; because the obstruction is present throughout fetal life, the whole system above suffers: a thick-walled trabeculated bladder, bilateral hydronephrosis, and impaired urine production that reduces amniotic fluid (oligohydramnios) and, in severe cases, causes pulmonary hypoplasia. Among the external genitalia, hypospadias results from incomplete fusion of the urethral folds, giving a triad of a ventral ectopic urethral meatus, ventral chordee (downward curvature), and a dorsally hooded prepuce; the undescended testis (cryptorchidism) is an arrest of normal testicular descent, leaving the gonad in the abdomen or inguinal canal where higher temperature impairs spermatogenesis and where the risk of malignancy and torsion is increased. The exstrophy-epispadias complex is a midline closure failure of the lower abdominal and bladder wall. Two structural variants complete the picture: the horseshoe kidney (lower poles fused across the midline, tethered under the inferior mesenteric artery and prone to stasis, stones and PUJ obstruction) and the duplex collecting system (a kidney drained by two ureters, in which the upper-pole ureter tends to obstruct and the lower-pole ureter tends to reflux).
Congenital Urinary Tract Anomalies: Anatomical Sites and Pathological Changes
- PUJ obstruction (renal pelvis): impaired drainage → hydronephrosis; commonest cause of antenatal hydronephrosis.
- VUR (ureterovesical junction): failed flap valve → retrograde infected urine → reflux nephropathy/scarring.
- PUV (posterior urethra, male only): outflow obstruction → trabeculated bladder, bilateral hydronephrosis, oligohydramnios, pulmonary hypoplasia.
- Hypospadias: ventral meatus + chordee + hooded prepuce. Undescended testis: arrested descent → infertility and malignancy risk.
SELF-CHECK
A newborn boy has a poor urinary stream, a palpable bladder, and antenatal scans showing bilateral hydronephrosis with oligohydramnios. Which anomaly is the most likely cause?
A. Pelviureteric junction obstruction
B. Posterior urethral valves
C. Vesicoureteric reflux
D. Hypospadias
Reveal Answer
Answer: B. Posterior urethral valves
This is the classic picture of posterior urethral valves — the commonest cause of lower urinary tract obstruction in male newborns. The lower-tract obstruction produces a thick-walled bladder, bilateral hydronephrosis and reduced fetal urine output (oligohydramnios, which threatens pulmonary hypoplasia). PUJ obstruction typically gives unilateral hydronephrosis without bladder outflow obstruction; VUR usually presents later with recurrent UTIs; hypospadias is an external genital anomaly and does not cause hydronephrosis.
Clinical Examination and Investigation
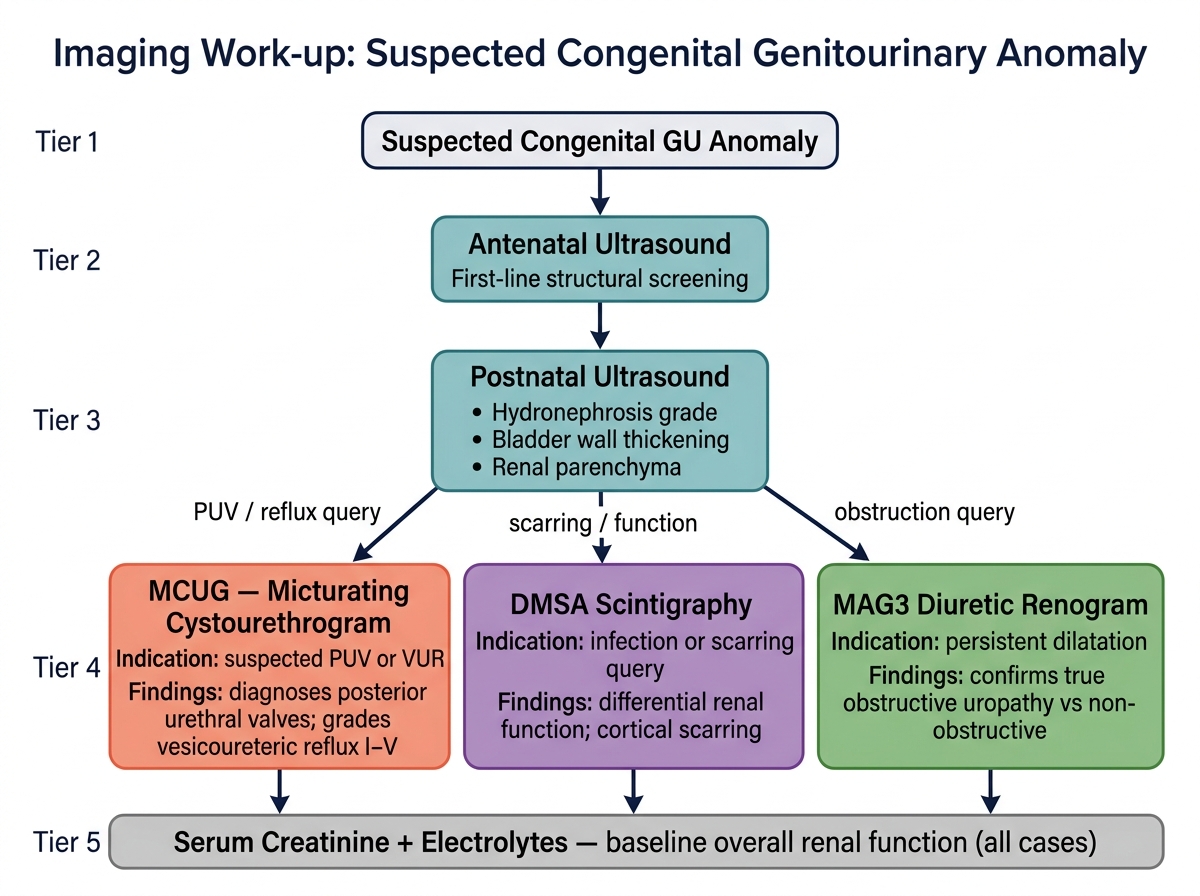
Examination and imaging are deployed in a logical order that follows from the suspected level of the lesion. The clinical examination begins with general observation and abdominal palpation for a flank mass (a hydronephrotic kidney) or a distended bladder, and proceeds to a careful inspection of the external genitalia: in a boy, note the position of the urethral meatus, the presence of chordee, and whether the prepuce is hooded (hypospadias), and palpate both sides of the scrotum and the inguinal canal to determine whether each testis is descended, retractile, or impalpable (undescended testis). In the male neonate, observe the urinary stream and feel for a palpable bladder. The imaging work-up is then built around a small set of complementary tests, each answering a specific question. Ultrasound — antenatally and then postnatally — is the screening and first-line structural test, demonstrating hydronephrosis, bladder wall thickening and the kidneys' size and parenchyma. The micturating cystourethrogram (MCUG) is the key functional test of the lower tract: it is diagnostic for posterior urethral valves (showing a dilated posterior urethra and the obstructing valve) and it is used to grade vesicoureteric reflux from I to V. A DMSA scan (a static cortical scan) shows differential renal function and, crucially, cortical scarring from reflux nephropathy. A MAG3 diuretic renogram is the test that distinguishes a genuinely obstructed system from one that is merely dilated, by tracking whether the tracer washes out after a diuretic — essential before committing a child to pyeloplasty. Underpinning all of these, serum creatinine and electrolytes quantify overall renal function and guide urgency, particularly in bilateral disease or PUV.
Imaging Algorithm for Suspected Congenital Genitourinary Anomaly
- Ultrasound (antenatal + postnatal): first-line structural test — hydronephrosis, bladder wall, parenchyma.
- MCUG: diagnostic for PUV; grades VUR (I–V).
- DMSA: differential function and cortical scarring.
- MAG3 diuretic renogram: confirms whether dilatation is truly obstructive. Serum creatinine/electrolytes: overall renal function.