Page 8 of 26
SU29.2 | Congenital Genitourinary Anomalies — SDL Guide (Part 2)
Principles of Surgical Management
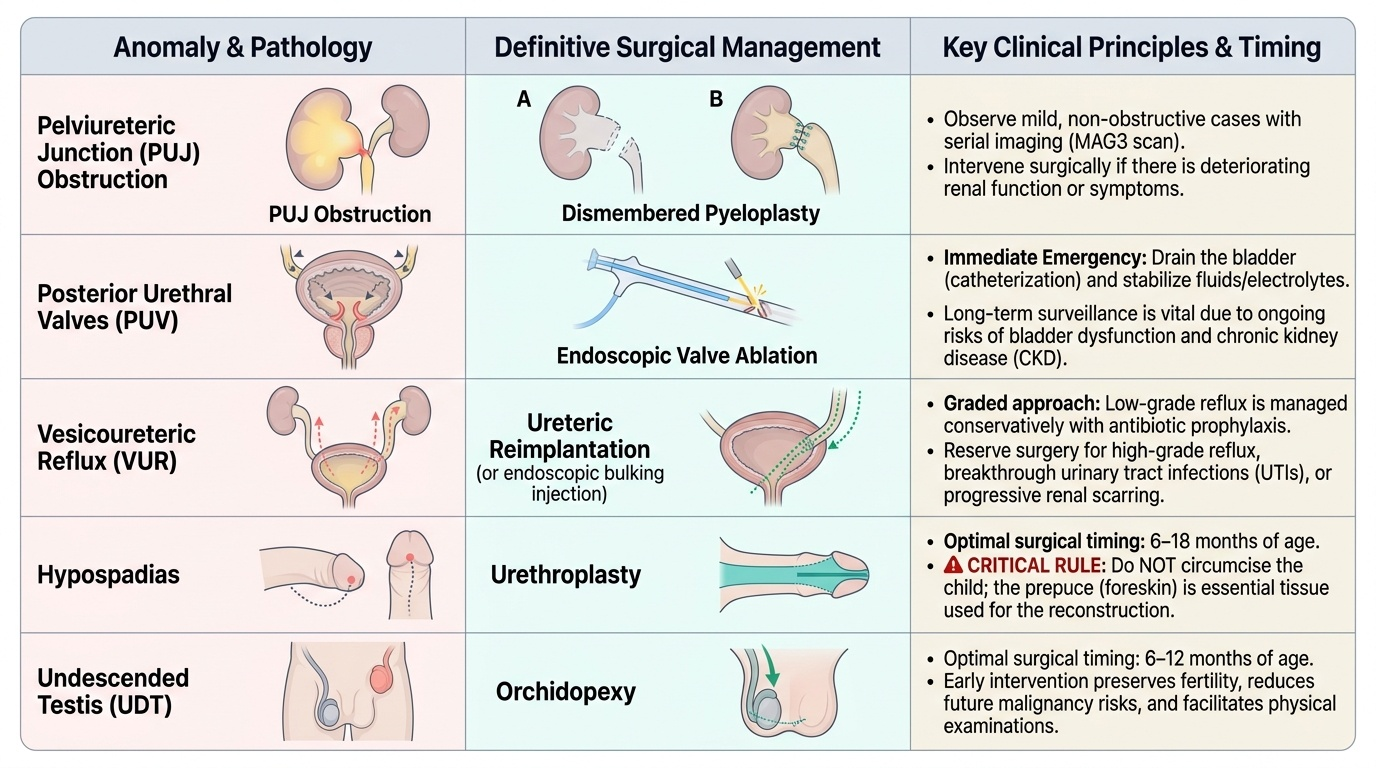
Management of every congenital genitourinary anomaly serves four shared principles — relieve obstruction, preserve renal function, treat and prevent infection, and reconstruct — and the specific operation follows from where the lesion sits and what the work-up has shown. For PUJ obstruction, mild antenatally detected hydronephrosis that is not obstructive on MAG3 and has preserved function can be observed with serial imaging, while a genuinely obstructed kidney with deteriorating function or symptoms is treated by pyeloplasty, classically the dismembered Anderson-Hynes repair that excises the narrow segment and re-anastomoses a funnelled pelvis to the ureter. For posterior urethral valves, the priorities are immediate: drain the bladder (catheter) and stabilise the often deranged fluid, electrolyte and renal status, then perform endoscopic valve ablation, followed by long-term protection and surveillance of bladder and renal function, since these children remain at risk of bladder dysfunction and chronic kidney disease. For vesicoureteric reflux, the principle is graded and largely conservative: low-grade reflux is managed by surveillance and, in selected children, antibiotic prophylaxis, with the expectation that many resolve spontaneously as the child grows; surgical ureteric reimplantation (or endoscopic injection) is reserved for high-grade reflux, breakthrough infections despite prophylaxis, or progressive scarring. For hypospadias, the definitive treatment is urethroplasty to bring the meatus to the tip, correct the chordee and reconstruct the urethra, usually performed at around 6–18 months of age — and the cardinal rule is that the child must NOT be circumcised, because the foreskin is the tissue used in the repair. For the undescended testis, orchidopexy brings the testis into the scrotum and fixes it there, performed by about 6–12 months of age to reduce the later risks of impaired fertility and malignancy and to allow examination of the gonad. Exstrophy-epispadias requires staged reconstructive closure in specialist centres. Across all of these, early recognition and the preservation of renal and reproductive function are what define success.
Provided image
| Anomaly | Definitive management | Key principle / caution |
|---|---|---|
| PUJ obstruction | Anderson-Hynes (dismembered) pyeloplasty | Confirm true obstruction on MAG3 first; observe non-obstructed mild HN |
| Posterior urethral valves | Endoscopic valve ablation (after catheter drainage + stabilisation) | Male only; protect bladder/renal function long-term |
| Vesicoureteric reflux | Prophylaxis/surveillance; reimplantation if high-grade/breakthrough | Many low-grade cases resolve spontaneously |
| Hypospadias | Urethroplasty (~6–18 months) | NEVER circumcise — foreskin needed for repair |
| Undescended testis | Orchidopexy (~6–12 months) | Reduces infertility and malignancy risk |
CLINICAL PEARL
Never circumcise a boy with hypospadias. The hooded, incomplete prepuce that draws attention to the condition is also the surgeon's primary reconstructive resource — its skin may be needed as a flap or graft to rebuild the urethra and resurface the penis during urethroplasty. A reflex newborn circumcision in such a child can remove the very material the repair may depend on and makes the definitive operation harder or impossible. The same instinct to slow down and think applies to the antenatally dilated kidney: dilatation is not the same as obstruction. Before committing a child to pyeloplasty, confirm with a MAG3 diuretic renogram that the system genuinely fails to drain — many mildly dilated kidneys are non-obstructed and need only watchful serial ultrasound, not an operation.
Check Your Understanding
Bring the threads together by reasoning back through the two neonates in the hook. The baby boy with a poor stream, a palpable bladder, and antenatal bilateral hydronephrosis with oligohydramnios has the textbook picture of posterior urethral valves — a lower-tract obstruction unique to males, demanding urgent bladder drainage and stabilisation, a diagnostic micturating cystourethrogram, and endoscopic valve ablation, with lifelong attention to bladder and renal function. The baby girl with isolated unilateral antenatal hydronephrosis who is otherwise well most likely has PUJ obstruction, which is investigated with postnatal ultrasound and a MAG3 diuretic renogram to decide whether the kidney is truly obstructed (pyeloplasty) or merely dilated (observation). Use these to self-test the competency this module covers. First, can you list the major congenital GU anomalies and the way each typically presents, including which one is confined to boys? Second, can you explain, anatomically, where each lesion sits and how it damages the kidney or genital tract? Third, can you name the right investigation for each question — ultrasound for structure, MCUG for valves and reflux grade, DMSA for scarring, MAG3 for obstruction — and the principle that guides each operation, including the two cardinal cautions (do not circumcise in hypospadias; confirm obstruction before pyeloplasty)? The questions check exactly these links.
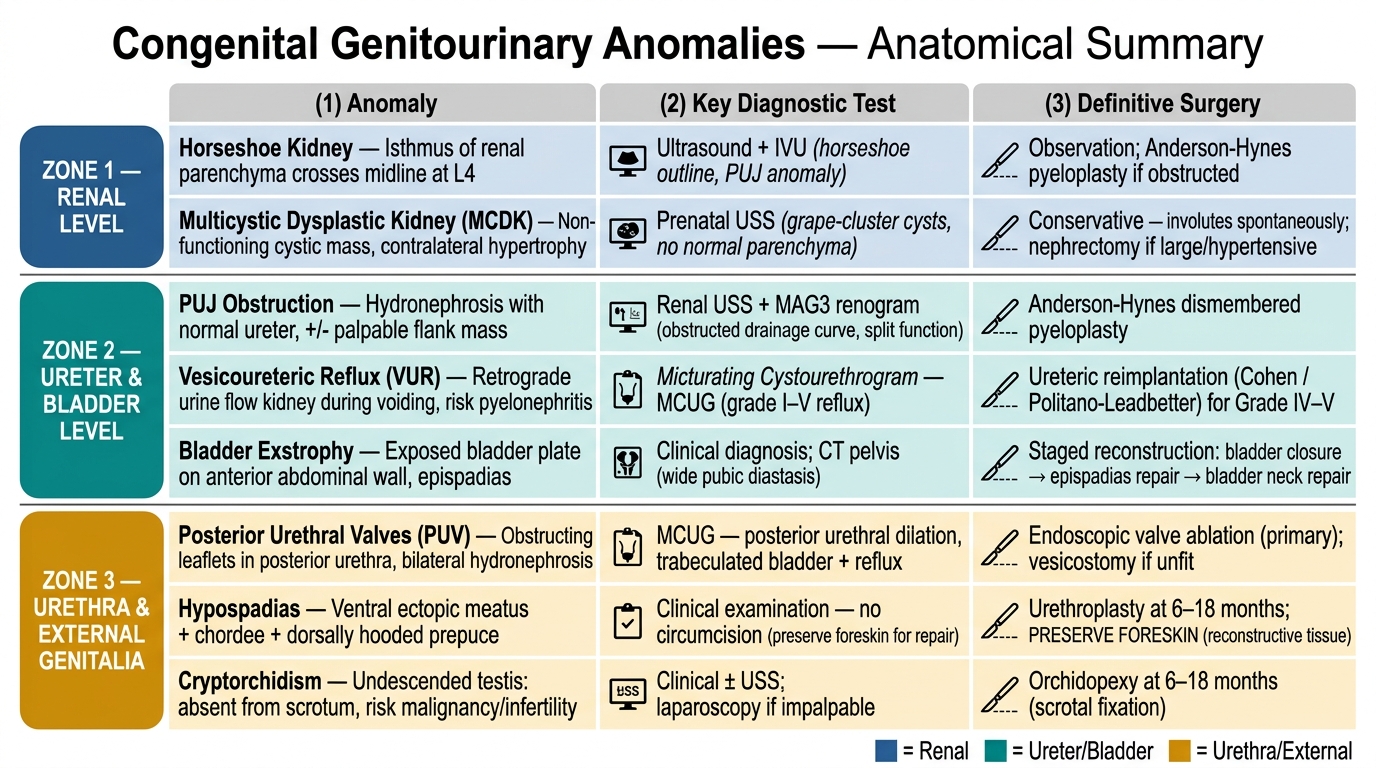
Congenital Genitourinary Anomalies: Anatomical Level, Key Diagnosis, and Definitive Surgery
SELF-CHECK
A boy is born with the urethral opening on the under-surface of the penis, a downward curvature, and an incompletely formed hooded foreskin. What is the single most important instruction regarding his early care?
A. Perform a routine neonatal circumcision before discharge
B. Do NOT circumcise — the foreskin is needed for the future urethroplasty
C. Begin long-term antibiotic prophylaxis immediately
D. Arrange urgent endoscopic valve ablation
Reveal Answer
Answer: B. Do NOT circumcise — the foreskin is needed for the future urethroplasty
This is hypospadias (ventral ectopic meatus + ventral chordee + dorsally hooded prepuce). The foreskin must be preserved because it is the tissue used to reconstruct the urethra and resurface the penis at urethroplasty (typically ~6–18 months); circumcising the child removes the reconstructive material. Antibiotic prophylaxis is a principle in vesicoureteric reflux, and endoscopic valve ablation is the treatment for posterior urethral valves — neither applies here.