Page 1 of 26
SU29.1 | Hematuria Evaluation — SDL Guide
Learning Objectives
- Define haematuria and distinguish visible (macroscopic) from non-visible (microscopic) bleeding, and initial from terminal from total haematuria, and use these patterns to localise the source within the urinary tract (SU29.1).
- Describe the causes of haematuria organised by anatomical level and distinguish surgical (urological) from medical (glomerular) haematuria (SU29.1).
- Outline the ordered investigation of haematuria — urinalysis and microscopy, urine cytology, CT urogram and flexible cystoscopy — and state the principles of management, including the rule that painless visible haematuria mandates a full urological work-up (SU29.1).
INSTRUCTIONS
Blood in the urine frightens patients and, handled correctly, is one of the most rewarding presentations in surgery because it lets you catch urological cancers early. The single rule that organises the whole topic is simple and unforgiving: painless visible haematuria is urological malignancy until proven otherwise, and it earns a complete work-up — never a single reassuring test. This module teaches you to separate the patient who can be reassured from the one who needs urgent cystoscopy, to localise the bleeding by its timing and character, to tell surgical bleeding apart from glomerular (medical) bleeding, and to order the investigations in the right sequence.
References
- Bailey & Love's Short Practice of Surgery, The Urinary Bladder / Haematuria (textbook)
- SRB's Manual of Surgery, Haematuria and Urological Investigations (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients sit in your clinic on the same morning. The first is a 28-year-old woman who passed pink urine for two days during a painful urinary infection; her symptoms settled with antibiotics and the urine is clear again. The second is a 66-year-old retired factory worker and lifelong smoker who, without any pain at all, noticed bright red urine once last week and has felt completely well since. Both have 'blood in the urine', yet they sit at opposite ends of risk. The young woman almost certainly had a self-limiting infective cause; the older man has the textbook presentation of a bladder cancer hiding behind a single painless bleed. Your task — and the discipline this module builds — is to tell these two apart reliably, and to refuse to be reassured by the older man's wellness or by one normal test.
WHY THIS MATTERS
Haematuria is among the commonest reasons a patient is referred to a surgeon or urologist, and the stakes are asymmetric: most causes are benign, but the minority that are malignant are curable when caught early and lethal when dismissed. The cardinal trap is the painless visible bleed that stops on its own — the patient feels reassured, and an undisciplined clinician is reassured with them, while a transitional-cell carcinoma of the bladder grows quietly. For a final-year student this is also a high-yield clinical and viva topic: you are expected to define the types of haematuria, localise the source from the history, separate surgical from medical bleeding, and recite the investigation pathway in the correct order. Getting the framework right here protects real patients from a missed cancer and protects you in every long case and OSCE that involves the urinary tract.
RECALL
Recall some foundations before we build on them. From anatomy: urine is made in the kidneys, drains down the ureters into the bladder, and leaves through the urethra, which in men passes through the prostate — so blood can enter the stream at any of these levels, and where it enters shapes how it appears. From physiology: the glomerular filtration barrier normally holds back red cells, so when red cells do escape through a diseased glomerulus they are squeezed and distorted into dysmorphic forms and may clump with protein into red-cell casts — the fingerprint of bleeding from the kidney's own filter rather than from the drainage plumbing. From general surgical oncology, recall that epithelial cancers spread and stage in characteristic ways; the urinary tract is lined by urothelium (transitional epithelium) from the renal pelvis to the proximal urethra, which is why a single field-change carcinogen can seed tumours anywhere along that lining.
The Patient with Blood in the Urine
Haematuria simply means red blood cells in the urine, but the way it presents carries most of the diagnostic information, so define it precisely before you investigate. Visible (macroscopic, gross) haematuria is urine the patient can see is discoloured red or smoky; non-visible (microscopic) haematuria is detected only by dipstick and confirmed by microscopy, the patient's urine looking normal. The single most important clinical pattern is the distinction between painful and painless bleeding: painless visible haematuria is urological malignancy until proven otherwise and must trigger a complete work-up, whereas haematuria accompanied by pain more often reflects infection, calculi or trauma — though pain never excludes a tumour. The timing of blood within the stream localises the source: initial haematuria (blood at the start, clearing as the patient voids) points to the urethra or prostate; terminal haematuria (blood at the end of voiding) points to the bladder neck, trigone or posterior urethra; and total haematuria (blood throughout the stream, often with clots) implies bleeding from the bladder or the upper tract — kidney and ureter. The history must capture the colour and timing, any clots (which imply a surgical, non-glomerular source), associated pain or lower-urinary-tract symptoms, and the cancer risk factors that follow. Finally, exclude pseudohaematuria — red or dark urine without red cells — caused by beetroot, the antitubercular drug rifampicin, myoglobinuria after muscle injury and haemoglobinuria after intravascular haemolysis; the dipstick is positive in haemoglobinuria and myoglobinuria but microscopy shows no red cells, which is how you tell them apart from true haematuria.
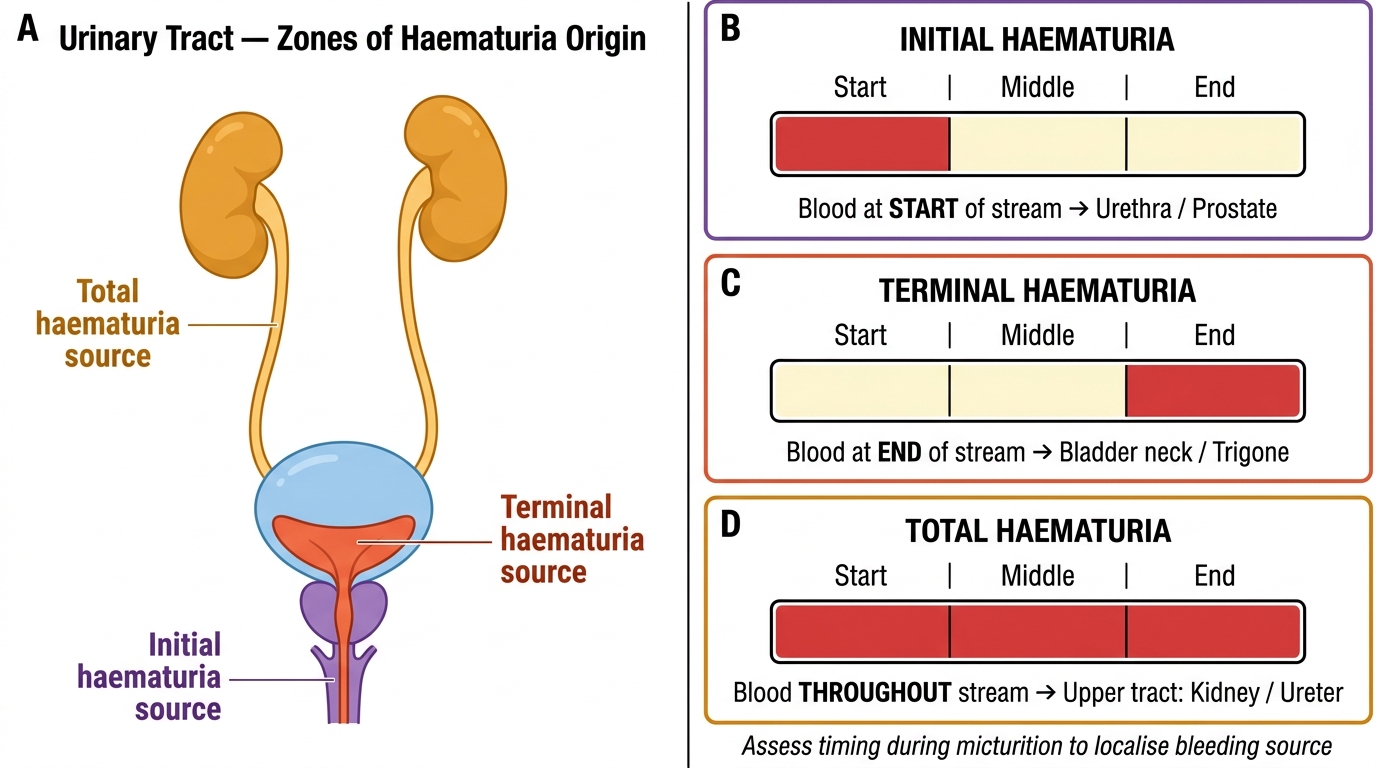
Haematuria Localisation: Urinary Tract Zones and Stream Timing
- Visible vs non-visible: seen by the patient vs detected only on dipstick/microscopy.
- Painless visible haematuria = urological malignancy until proven otherwise (full work-up).
- Initial → urethra/prostate; terminal → bladder neck/trigone; total → bladder or upper tract.
- Pseudohaematuria (no RBCs on microscopy): beetroot, rifampicin, myoglobinuria, haemoglobinuria.
Causes by Tract Level and the Surgical-versus-Medical Divide
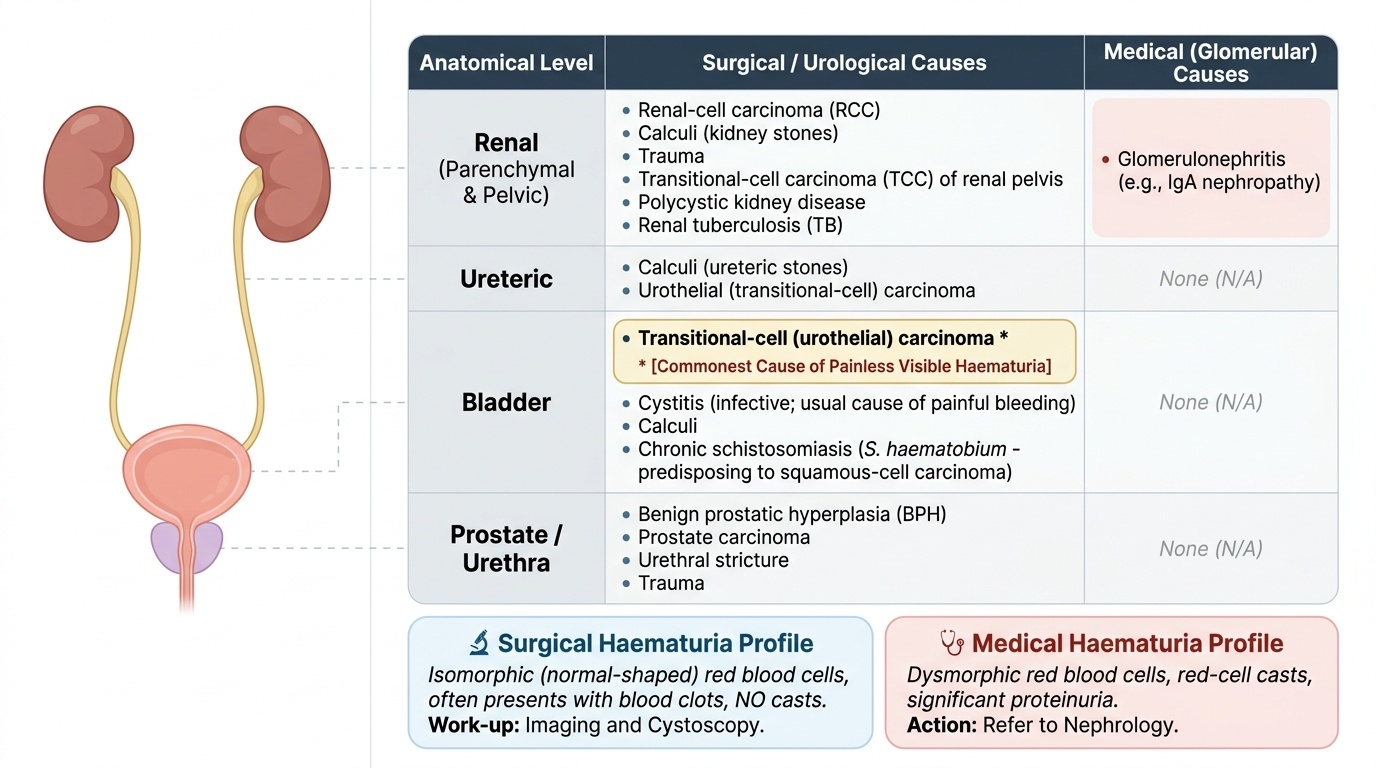
Once true haematuria is confirmed, organise the causes anatomically from kidney to urethra, because a level-by-level list is both exhaustive and clinically usable. At the renal (parenchymal/pelvic) level, surgical causes include renal-cell carcinoma, calculi, trauma, transitional-cell carcinoma of the renal pelvis, polycystic kidney disease and renal tuberculosis, while glomerular (medical) disease such as IgA nephropathy and other glomerulonephritides also bleeds here. At the ureteric level, the leading causes are calculi and urothelial (transitional-cell) carcinoma. At the bladder level, the dominant surgical cause — and the commonest cause of painless visible haematuria — is transitional-cell (urothelial) carcinoma; other bladder causes are cystitis (infective, the usual cause of painful bleeding), calculi, and chronic schistosomiasis (Schistosoma haematobium), which through chronic inflammation predisposes to squamous-cell carcinoma of the bladder. At the prostate/urethral level, causes include benign prostatic hyperplasia, prostate carcinoma, urethral stricture and trauma. Cutting across this anatomical list is the crucial clinical divide between surgical (urological) and medical (glomerular) haematuria: surgical bleeding gives isomorphic (normal-shaped) red cells, often with clots and no casts, and is worked up by imaging and cystoscopy, whereas medical bleeding gives dysmorphic red cells, red-cell casts and significant proteinuria, which should be referred to nephrology rather than subjected to a surgical work-up. Finally, know the risk factors for urothelial cancer that raise your suspicion in any haematuria: cigarette smoking (the strongest modifiable factor), occupational exposure to aromatic amines (aniline dyes, rubber and the printing industry), prior cyclophosphamide therapy, and chronic bladder irritation including schistosomiasis.
Provided image
| Level | Principal surgical/urological causes | Medical (glomerular) causes |
|---|---|---|
| Renal | RCC, calculi, trauma, TCC of renal pelvis, polycystic kidney, TB | Glomerulonephritis (e.g. IgA nephropathy) |
| Ureteric | Calculi, urothelial (transitional-cell) carcinoma | — |
| Bladder | TCC (commonest painless cause), cystitis, calculi, schistosomiasis → SCC | — |
| Prostate/urethra | BPH, prostate carcinoma, stricture, trauma | — |
SELF-CHECK
A 64-year-old smoker reports a single episode of painless, bright-red urine and is otherwise completely well. Which is the single commonest cause of painless visible haematuria that you must exclude?
A. Acute cystitis
B. Transitional-cell (urothelial) carcinoma of the bladder
C. Benign prostatic hyperplasia
D. IgA nephropathy
Reveal Answer
Answer: B. Transitional-cell (urothelial) carcinoma of the bladder
Transitional-cell (urothelial) carcinoma of the bladder is the commonest cause of painless visible haematuria, and a smoking history sharply increases that risk. Painless visible haematuria is urological malignancy until proven otherwise and mandates a full work-up. Cystitis typically causes PAINFUL bleeding; BPH may cause haematuria but is a diagnosis of exclusion only after malignancy is ruled out; IgA nephropathy is a glomerular (medical) cause flagged by dysmorphic red cells and red-cell casts, not isolated painless visible bleeding.
Examination and the Haematuria Work-up
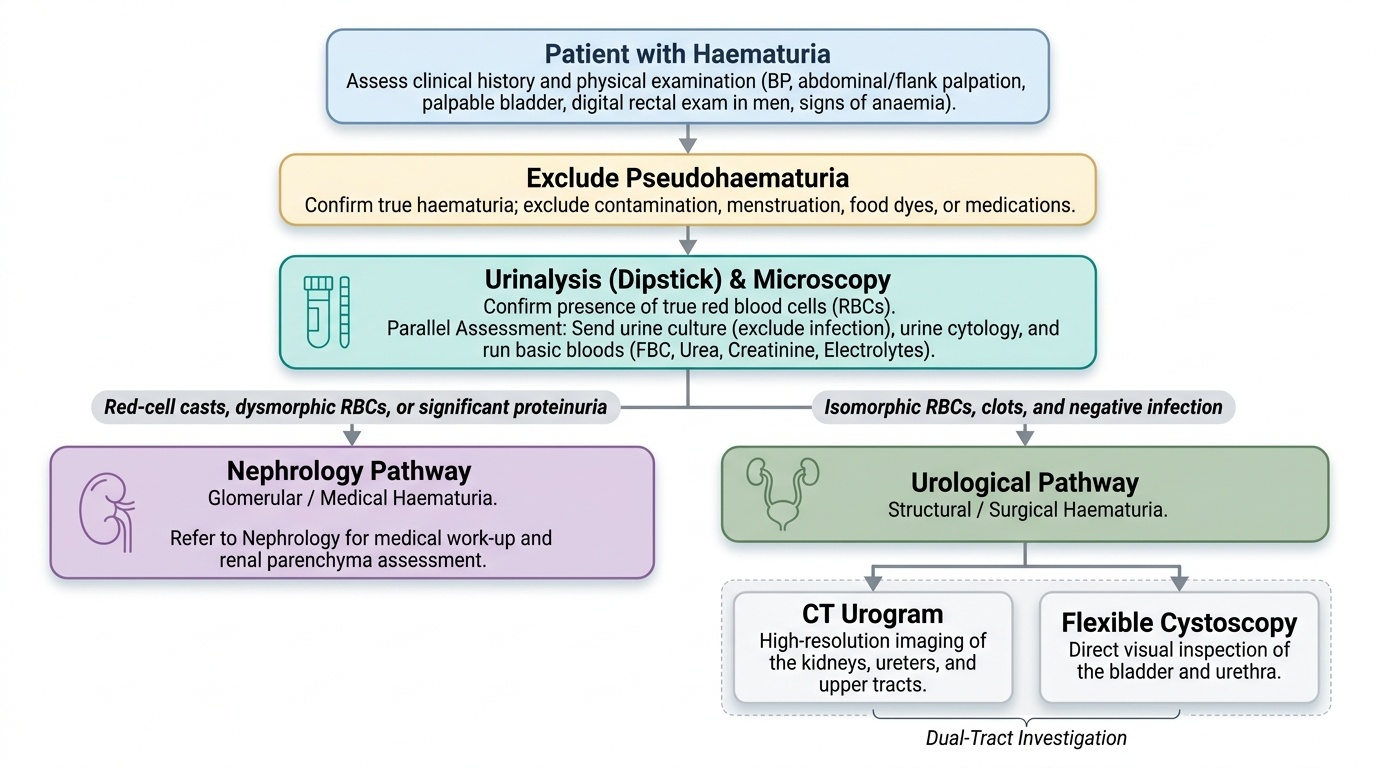
Examination in haematuria is focused but disciplined, and it is followed by a fixed investigation sequence so that no patient is reassured prematurely. On examination, check the blood pressure (hypertension and oedema hint at glomerular disease), palpate the abdomen and flanks for a renal mass or tenderness, examine for a palpable bladder (clot retention), and in men perform a digital rectal examination to assess the prostate; look for signs of anaemia from chronic blood loss. The investigation pathway then proceeds in order. First, urinalysis (dipstick) plus microscopy confirms that true red cells are present and looks for casts and dysmorphic red cells: the presence of red-cell casts, dysmorphic red cells or significant proteinuria redirects the patient to nephrology as medical/glomerular haematuria, whereas isomorphic red cells and clots keep the patient on the surgical pathway. Send urine for culture to exclude infection and urine cytology, which can detect high-grade urothelial malignancy (it is insensitive for low-grade tumours, so a negative cytology never excludes cancer). Take bloods including full blood count, urea/creatinine and electrolytes to assess renal function and anaemia. For imaging of the upper urinary tract, CT urogram is the investigation of choice because it demonstrates renal masses, stones and upper-tract urothelial tumours in one study; ultrasound is a useful, radiation-free first-line adjunct (good for renal masses, hydronephrosis and bladder lesions) but is less sensitive for small upper-tract tumours and stones. The bladder and lower tract are assessed by flexible cystoscopy, which is the gold-standard investigation and is mandatory in any adult with painless visible haematuria because it directly visualises bladder tumours that imaging can miss. The work-up is therefore not a single test but a coordinated set — upper tract by CT urogram, lower tract by cystoscopy — completed regardless of whether an early test happens to be normal.
Provided image
- Urinalysis + microscopy: confirm RBCs; red-cell casts/dysmorphic RBCs/proteinuria → nephrology.
- Urine cytology: detects high-grade urothelial cancer; a negative result does NOT exclude cancer.
- Bloods: FBC, urea/creatinine/electrolytes (renal function, anaemia).
- CT urogram = imaging of choice for the upper tract; ultrasound is a radiation-free adjunct.
- Flexible cystoscopy = gold standard for the bladder/lower tract.