Page 2 of 26
SU29.1 | Hematuria Evaluation — SDL Guide (Part 2)
Principles of Management
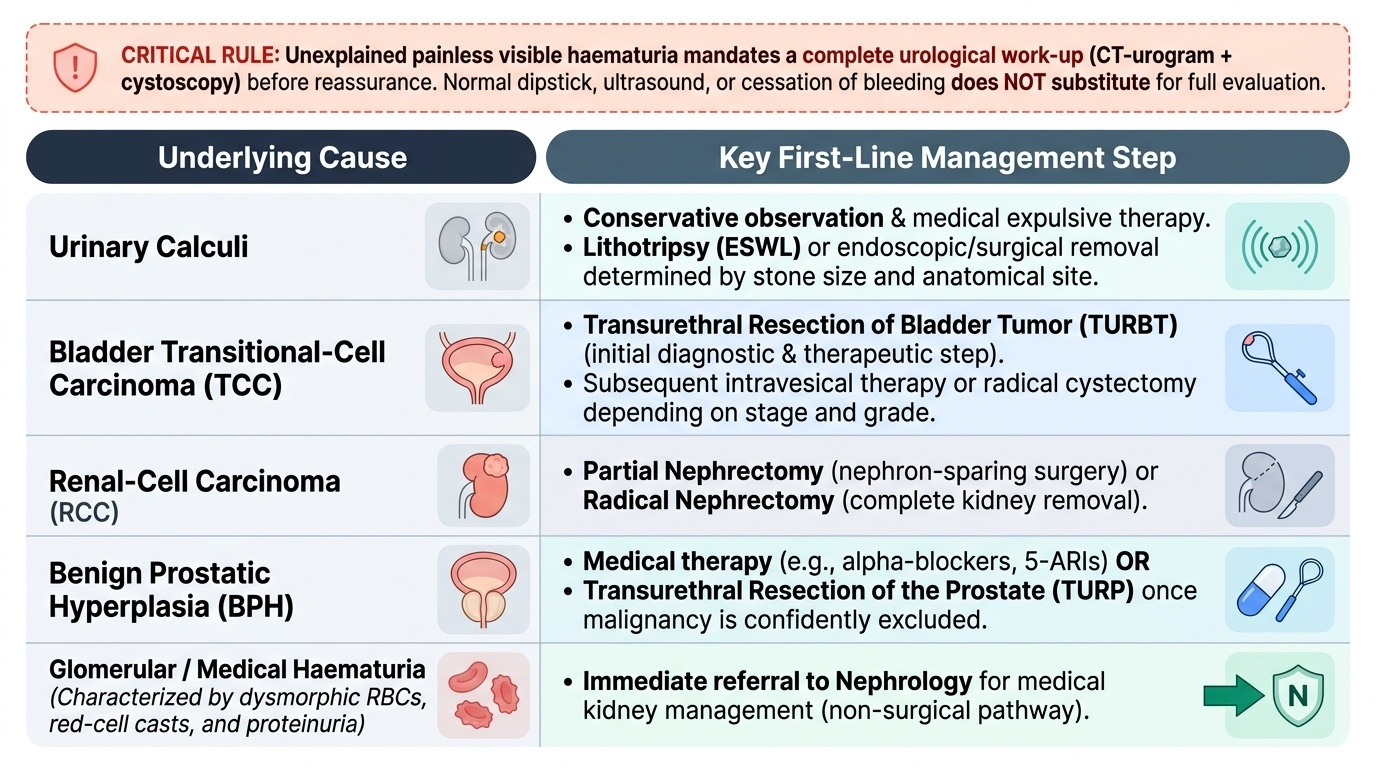
The governing principle of management is straightforward: treat the underlying cause, but only after the cause has been properly established, and the single non-negotiable rule is that unexplained painless visible haematuria mandates a complete urological work-up before any reassurance is given — a normal dipstick, a normal ultrasound or spontaneous cessation of bleeding never substitute for the full CT-urogram-plus-cystoscopy evaluation. Acute management addresses the bleeding itself: a patient in clot retention needs catheterisation and bladder washout/irrigation, and significant blood loss needs resuscitation, correction of anaemia and review of any anticoagulation. Definitive management then follows the diagnosis. Bladder transitional-cell carcinoma is diagnosed and initially treated by transurethral resection of bladder tumour (TURBT), with intravesical therapy or radical cystectomy according to stage and grade. Renal-cell carcinoma is managed by partial or radical nephrectomy. Urinary calculi are treated according to size and site by conservative measures, lithotripsy or endoscopic/surgical removal. Benign prostatic hyperplasia causing haematuria is managed medically or by transurethral resection of the prostate once malignancy is excluded, and prostate carcinoma by its own stage-directed pathway. When the work-up instead shows medical/glomerular haematuria — dysmorphic red cells, red-cell casts and proteinuria — the patient is referred to nephrology rather than managed surgically. The thread running through all of these is that management is only as safe as the work-up that preceded it: localise the bleeding, exclude malignancy completely, and then treat the specific cause.
Provided image
| Cause | Key first-line management step |
|---|---|
| Urinary calculi | Conservative/medical expulsive therapy, lithotripsy or endoscopic/surgical removal by size & site |
| Bladder TCC | Transurethral resection of bladder tumour (TURBT); then intravesical therapy or cystectomy by stage/grade |
| Renal-cell carcinoma | Partial or radical nephrectomy |
| Benign prostatic hyperplasia | Medical therapy or TURP — only after malignancy excluded |
| Glomerular/medical haematuria | Refer to nephrology (red-cell casts, dysmorphic RBCs, proteinuria) |
CLINICAL PEARL
Never let a single normal test or the patient's own wellness close the case in painless visible haematuria. The bleed from a bladder cancer is characteristically intermittent and painless, so it may have stopped by the time the patient reaches you and a snapshot urinalysis may even be clear. The full work-up — CT urogram for the upper tract AND flexible cystoscopy for the bladder — must be completed in every adult with painless visible haematuria, because cystoscopy sees tumours that imaging misses and imaging sees upper-tract lesions that cystoscopy cannot reach. Conversely, if microscopy shows red-cell casts and dysmorphic red cells with proteinuria, stop the surgical work-up and refer to nephrology — that is medical, not surgical, haematuria.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 28-year-old woman had painful visible haematuria during a culture-proven urinary infection that resolved with treatment and a clear urine afterwards — a pattern consistent with cystitis; she still warrants confirmation that the urine clears and follow-up, but she sits at the benign end. The 66-year-old smoker had a single episode of painless visible haematuria and feels completely well — and that combination is the textbook presentation of bladder cancer: his wellness and the bleeding having stopped are exactly the features that must NOT reassure you, and he requires urine cytology, CT urogram for the upper tract and flexible cystoscopy for the bladder regardless of any normal early test. Use these to self-test the competency this module covers. First, can you define visible versus non-visible haematuria and use initial/terminal/total timing to localise the source to urethra-prostate, bladder neck, or upper tract? Second, can you list the causes by tract level, name transitional-cell carcinoma as the commonest cause of painless visible haematuria, and separate surgical (isomorphic cells, clots, no casts) from medical (dysmorphic cells, red-cell casts, proteinuria) haematuria? Third, can you state the investigation order — urinalysis/microscopy, cytology, bloods, CT urogram (upper tract) and flexible cystoscopy (bladder gold standard) — and the management principle that painless visible haematuria mandates a full work-up before reassurance? The questions that follow check exactly these links.
SELF-CHECK
In a patient being worked up for visible haematuria, which finding on urine microscopy indicates a glomerular (medical) source that should be referred to nephrology rather than to the surgical/urological pathway?
A. Isomorphic (normal-shaped) red cells with clots
B. Red-cell casts and dysmorphic red cells with proteinuria
C. A positive dipstick for blood with no red cells on microscopy
D. Bacteria and white cells with normal red-cell morphology
Reveal Answer
Answer: B. Red-cell casts and dysmorphic red cells with proteinuria
Red-cell casts and dysmorphic (distorted) red cells, usually with proteinuria, indicate bleeding from the glomerulus — medical/glomerular haematuria — and the patient should be referred to nephrology. Isomorphic red cells with clots indicate surgical (urological) bleeding worked up by CT urogram and cystoscopy. A positive dipstick with NO red cells on microscopy is pseudohaematuria (e.g. haemoglobinuria/myoglobinuria), not true haematuria. Bacteria and white cells suggest infection (cystitis).