Page 13 of 26
SU29.4-5 | Hydronephrosis and Renal Calculi — SDL Guide
Learning Objectives
- Describe the clinical features, investigations and principles of management of hydronephrosis, including its classification by level of obstruction (SU29.4).
- Describe the clinical features, investigations and principles of management of renal calculi, including stone types and size-based treatment (SU29.5).
- Recognise the obstructed, infected upper urinary tract as a surgical emergency requiring urgent decompression.
INSTRUCTIONS
Obstruction to the flow of urine and the stones that so often cause it are among the commonest reasons a patient reaches a surgical clinic in loin pain. The two conditions in this module are inseparable: a calculus impacted in the ureter is one of the leading causes of hydronephrosis, and hydronephrosis is the kidney's response to any obstruction left unrelieved. The central task is to recognise an obstructed kidney, find and characterise the cause, judge how urgent relief is, and choose the right modality to relieve obstruction while preserving renal function. Get the urgency wrong — miss an obstructed, infected system — and a salvageable kidney is lost or the patient becomes septic; get the work-up wrong and a radiolucent stone is missed on a plain film. This module threads both conditions through one clinical arc, from presentation to safe surgical decision-making.
References
- Bailey & Love's Short Practice of Surgery, The Kidneys and Ureters / Urinary Calculi (textbook)
- SRB's Manual of Surgery, Urology — Hydronephrosis and Urolithiasis (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man arrives at the emergency department doubled over, unable to keep still on the trolley, gripping his right loin as a wave of pain radiates down towards his groin and testis. He is sweating and has vomited twice; his urine, when he finally passes some, is pink. In a quieter corner of the clinic the same morning sits a 60-year-old man whose only complaint is a dull, dragging ache in the left loin that has crept up over months, and who on examination has a vague fullness you can ballotte between your hands. Two patients, the same anatomical region, two completely different tempos — one an acute ureteric colic from a stone on the move, the other a slowly obstructed, dilated kidney. Your job is to tell them apart, find out why each kidney is obstructed, and decide how urgently the obstruction must be relieved.
WHY THIS MATTERS
Urinary stones are extremely common and frequently recurrent, and obstruction is the thread that links a benign-sounding stone to permanent renal damage. The clinical stakes are concentrated in a few decisions. First, an obstructed kidney that also becomes infected — a pyonephrosis — is a true surgical emergency: pus under pressure destroys renal tissue within days and seeds life-threatening sepsis, so the system must be drained urgently rather than waiting to remove the stone. Second, an obstruction that is silent (the slowly dilating hydronephrosis) can quietly abolish a kidney's function before the patient ever complains, which is why imaging and a test of true obstruction matter. Third, choosing the wrong stone treatment — for instance hunting a radiolucent uric-acid stone on a plain X-ray, or attempting to fragment a large staghorn calculus with shockwaves — wastes time and harms the patient. For a final-year student, ureteric colic, the loin mass and the obstructed infected kidney are recurring examination and on-call scenarios where a clear, safe plan is expected.
RECALL
Recall some foundations before we build on them. From anatomy: urine drains from the renal papillae into the minor and major calyces, into the renal pelvis, and down the ureter, which has three physiological narrowings where stones characteristically lodge — the pelviureteric junction (PUJ), the pelvic brim where the ureter crosses the iliac vessels, and the vesicoureteric junction (VUJ) as it enters the bladder. The ureter then drains into the bladder, which empties through the urethra; in men the prostate surrounds the urethral outlet. From physiology: the kidney filters plasma at the glomerulus to form urine, and continued filtration against an obstructed outflow is what raises pressure back up the system, distends the pelvis and calyces, and — if unrelieved — compresses and thins the renal parenchyma. Hold on to two ideas in particular: obstruction is defined by the level at which urine flow is blocked, and the kidney's functional reserve is finite, so time-to-relief is what determines whether function recovers.
The Patient with Loin Pain and an Obstructed Kidney
The two conditions in this module declare themselves through loin pain of very different character, and the history is what first separates a stone in transit from a chronically obstructed, dilated kidney. Renal (ureteric) colic — the classic presentation of a calculus moving down the ureter — is a sudden, severe, colicky loin-to-groin pain that comes in waves and makes the patient restless and unable to lie still (in contrast to peritonitis, where the patient lies rigidly still). It is typically accompanied by haematuria (often microscopic), nausea and vomiting, and may radiate to the groin, scrotum or labia and tip of the penis as the stone nears the vesicoureteric junction, where it can also cause urinary frequency and urgency. By contrast, hydronephrosis — dilatation of the renal pelvis and calyces from any obstruction to urine flow — is frequently far more insidious: it may cause a dull, dragging loin ache or a palpable loin mass, or it may be entirely silent and discovered only when the kidney's function has already declined or on imaging done for another reason. The history must therefore pin down the tempo, the site and radiation of pain, and any red flags for an obstructed infected system — fever, rigors, dysuria and being systemically unwell, which together suggest pyonephrosis and demand urgent action. Ask too about lower-urinary-tract symptoms (poor stream, hesitancy, nocturia) that point to bladder-outlet obstruction as the cause of bilateral hydronephrosis, about previous stones (urolithiasis is highly recurrent), and about anuria, which in a patient with a single functioning kidney or bilateral obstruction is an emergency. This structured history already separates the acute stone from the chronic obstruction and flags the patient who cannot wait.
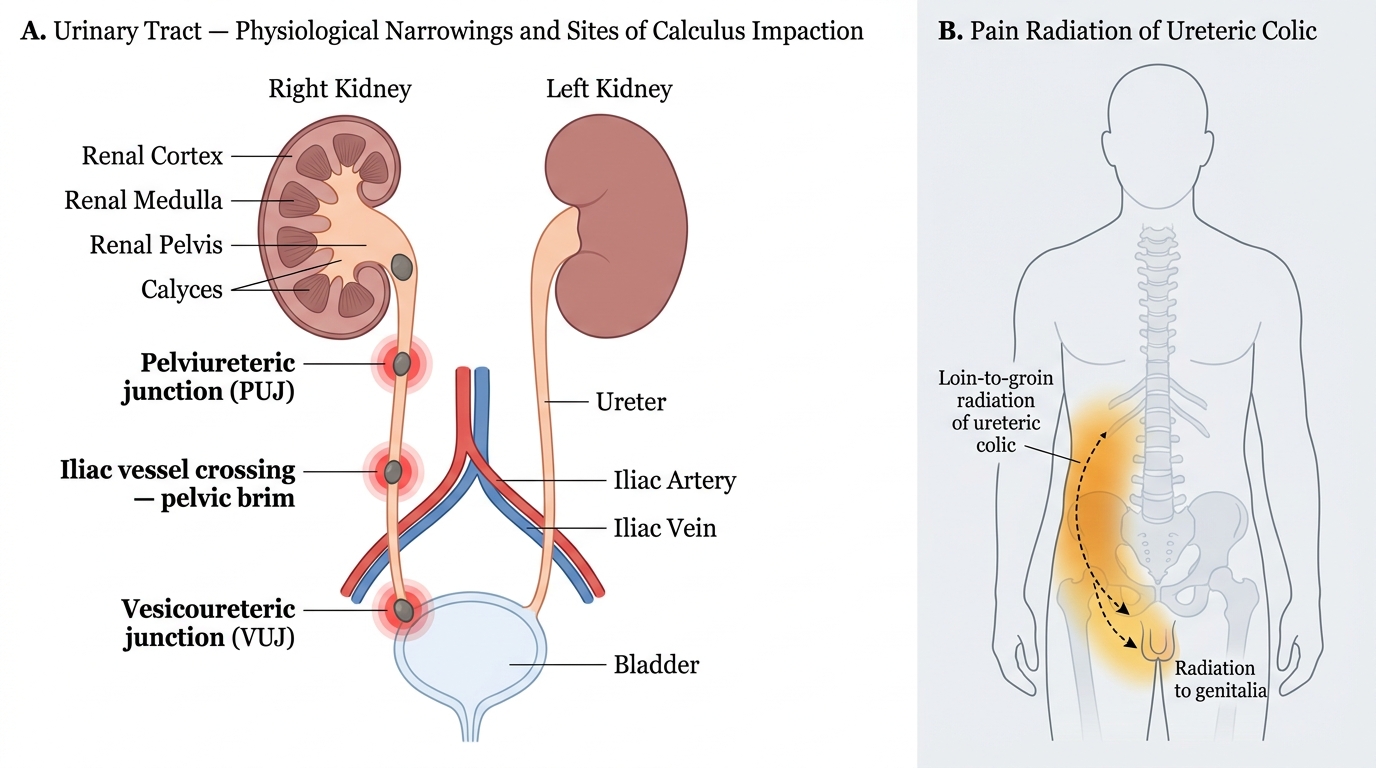
Physiological Narrowings of the Ureter and Pain Radiation of Ureteric Colic
Pathology of Obstruction, Hydronephrosis and Stone Formation
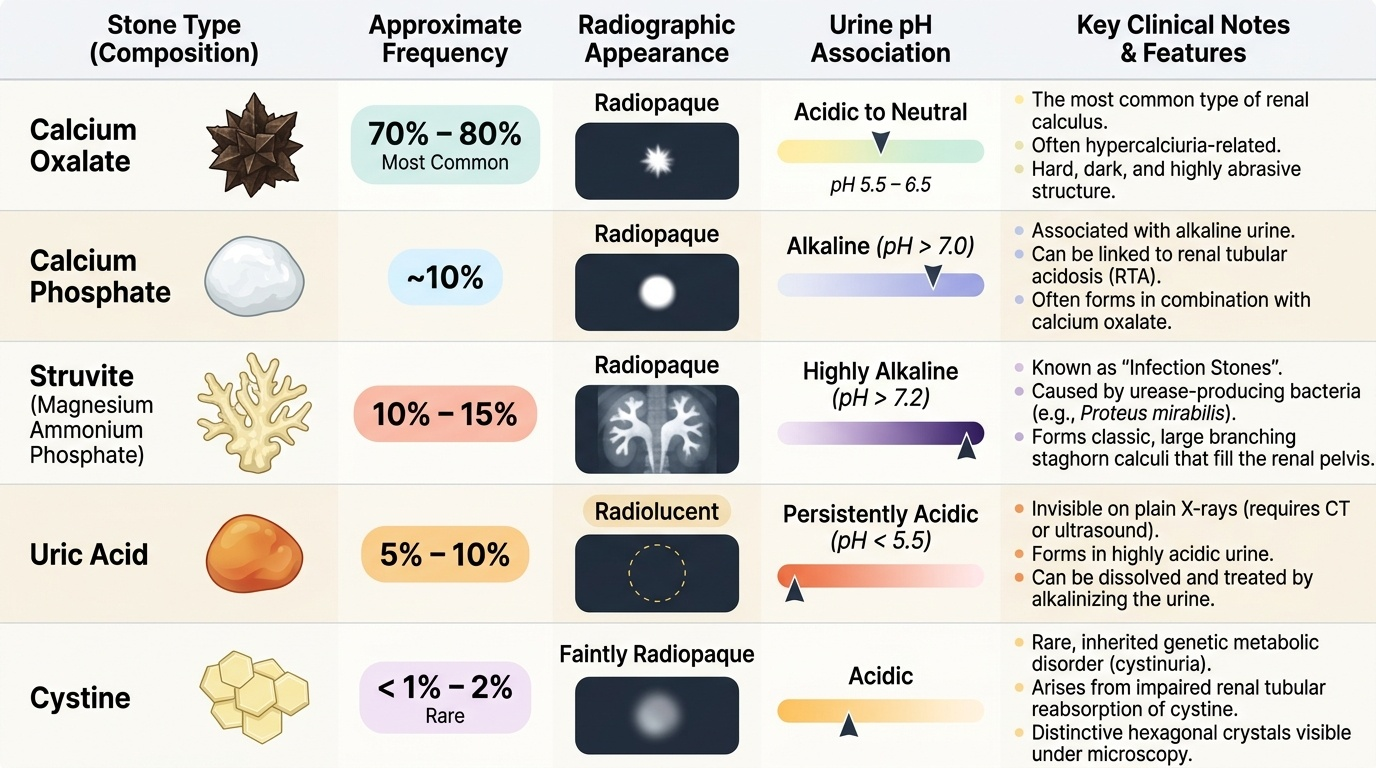
Understanding management begins with the mechanism. Hydronephrosis is the dilatation of the renal pelvis and calyces produced by obstruction to the outflow of urine; continued glomerular filtration against the block raises intrapelvic pressure, balloons the calyces, and — if the obstruction persists — progressively compresses and thins the renal cortex until function is lost, while stasis behind the obstruction predisposes to infection (pyelonephritis and, when pus collects under pressure, pyonephrosis). The single most useful way to classify hydronephrosis is by the level of obstruction, because the level predicts whether one or both kidneys are affected and points to the cause. Unilateral hydronephrosis results from obstruction at or above one ureter — pelviureteric junction (PUJ) obstruction (the commonest congenital cause), an impacted calculus, a ureteric stricture, a tumour of the renal pelvis or ureter, or extrinsic compression such as retroperitoneal fibrosis. Bilateral hydronephrosis points to obstruction at or below the bladder outlet affecting both kidneys — benign prostatic hyperplasia, a urethral stricture, posterior urethral valves in a male infant, or a neurogenic bladder. Pregnancy causes a physiological hydronephrosis (usually right-sided, from progesterone and mechanical compression) that needs no treatment. The other half of this module is the stone itself. Renal calculi are classified by their composition, and the type matters because it predicts radiographic appearance and treatment. Calcium oxalate is the commonest stone (~70-80%) and is radiopaque; calcium phosphate stones are also radiopaque and associated with alkaline urine. Struvite (magnesium ammonium phosphate) stones are infection stones that form in the presence of urease-producing organisms such as Proteus which alkalinise the urine; they are the classic cause of large branching staghorn calculi that fill the pelvicalyceal system. Uric acid stones are radiolucent — invisible on a plain X-ray — and form in persistently acidic urine, which is why they can be dissolved by alkalinising the urine. Cystine stones are rare and inherited (cystinuria). A stone impacted at one of the ureteric narrowings is itself a leading cause of obstruction, closing the loop between the two competencies.
Provided image
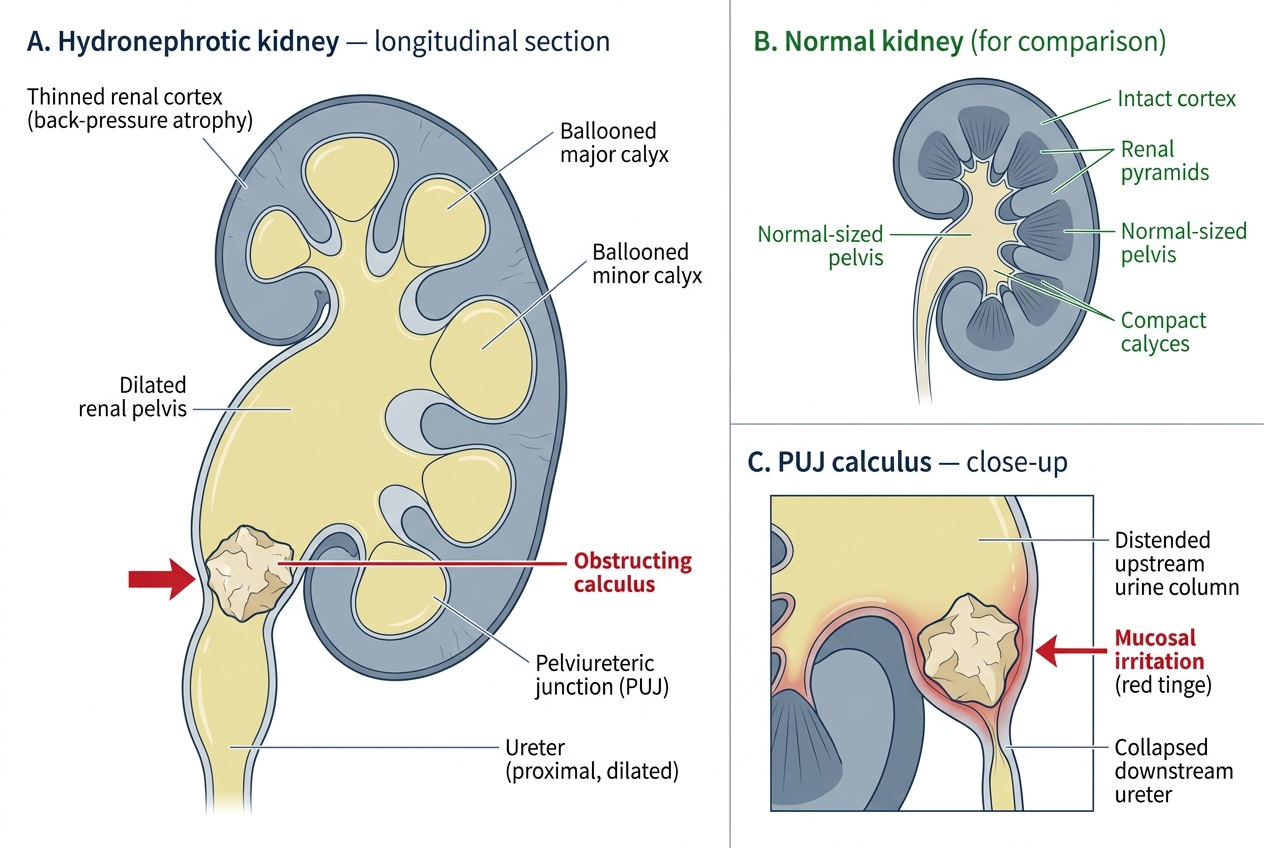
Hydronephrotic Kidney — Longitudinal Section with PUJ Calculus Obstruction
- Hydronephrosis by level: unilateral (ureteric level) — PUJ obstruction, calculus, stricture, tumour, retroperitoneal fibrosis; bilateral (outlet level) — BPH, urethral stricture, posterior urethral valves, neurogenic bladder; pregnancy = physiological.
- Calcium oxalate (~70-80%, commonest, radiopaque); calcium phosphate (radiopaque, alkaline urine).
- Struvite = infection/staghorn stone (urease-producing Proteus, alkaline urine).
- Uric acid = radiolucent, acidic urine, dissolvable by alkalinisation.
- Cystine = rare, inherited (cystinuria).
SELF-CHECK
Which renal stone type is radiolucent on a plain abdominal X-ray and may be dissolved by alkalinisation of the urine?
A. Calcium oxalate
B. Struvite (magnesium ammonium phosphate)
C. Uric acid
D. Calcium phosphate
Reveal Answer
Answer: C. Uric acid
Uric acid stones are radiolucent (not seen on a plain KUB film) and form in acidic urine, so they can be dissolved by urinary alkalinisation. Calcium oxalate (the commonest), calcium phosphate and struvite stones are all radiopaque; struvite is the infection/staghorn stone associated with urease-producing organisms such as Proteus.
Examination and the Imaging Work-up
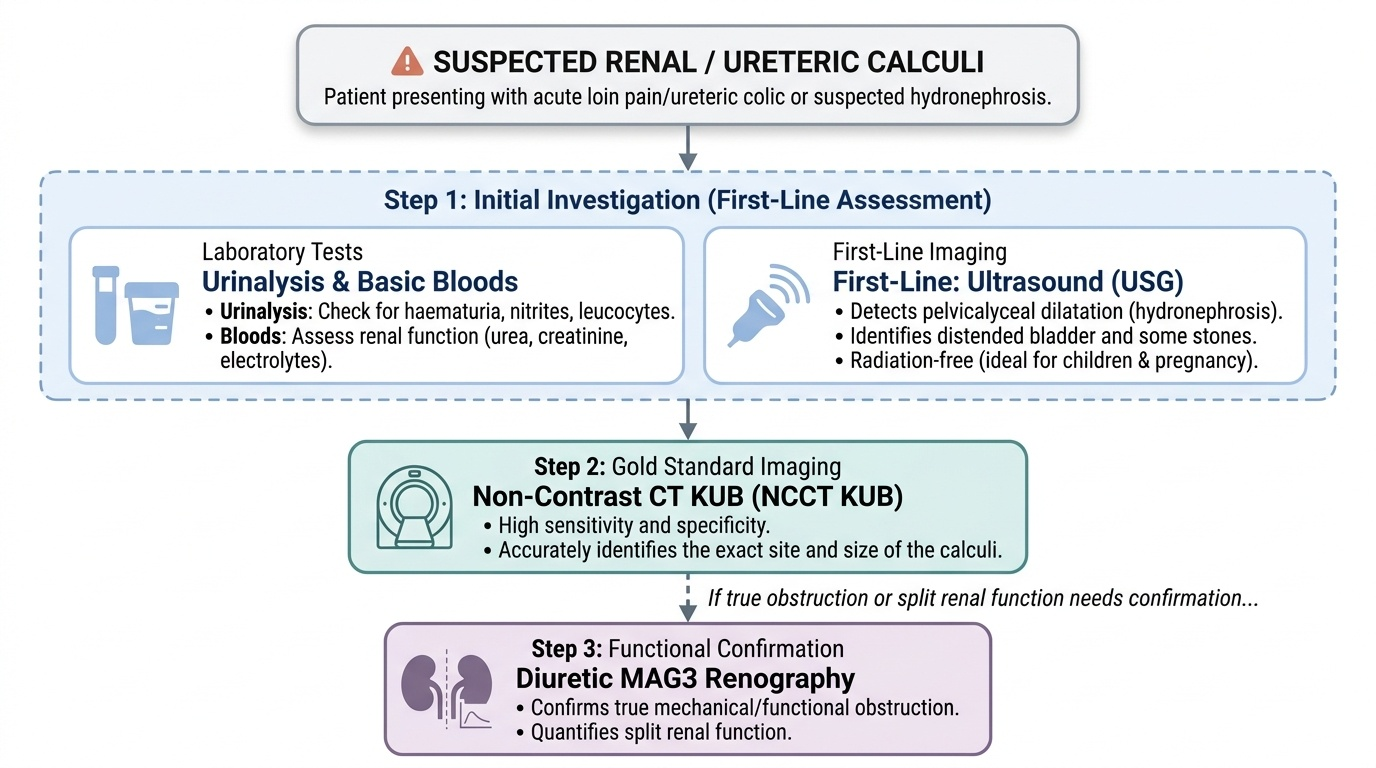
Examination in obstructive uropathy is focused and quickly narrows the problem, but it is the imaging that confirms the diagnosis, locates the obstruction and characterises the stone. On examination, the patient in ureteric colic is restless with marked loin (renal angle) tenderness and no peritonism; in chronic hydronephrosis you may feel a smooth, ballottable loin mass that moves with respiration. Always look for signs of an obstructed infected system (fever, tachycardia, a tender loin and a toxic patient), palpate for a distended bladder and, in a man with bilateral hydronephrosis, perform a digital rectal examination to assess the prostate, because the cause may lie at the outlet rather than in the ureter. Investigation then proceeds in a deliberate order. Start with urinalysis (haematuria supports a stone; nitrites and leucocytes suggest infection) and basic bloods including renal function (urea, creatinine, electrolytes). Ultrasound (USG) is the first-line imaging test: it reliably shows pelvicalyceal dilatation (the hallmark of hydronephrosis), is radiation-free, and can detect many stones and a distended bladder, making it ideal in children and pregnancy. For stones specifically, non-contrast CT of the kidneys, ureters and bladder (NCCT KUB) is the gold-standard investigation — it has high sensitivity, identifies the size and exact site of a calculus, and crucially detects radiolucent uric-acid stones that a plain X-ray misses. A plain KUB X-ray still has a role for following up known radiopaque stones, but it cannot exclude a radiolucent one. Where it is necessary to prove that a dilated system is truly obstructed (rather than merely capacious) and to measure each kidney's contribution, diuretic renography with MAG3 is the key functional test: it confirms genuine obstruction and gives the split renal function that decides whether a poorly functioning kidney is worth salvaging. Finally, recurrent or multiple stone formers warrant a metabolic work-up (serum calcium, urate, and 24-hour urine studies) to find a treatable cause. This ordered pathway separates a dilated-but-unobstructed system from a true obstruction, and a radiopaque from a radiolucent stone, before any decision about surgery.
Provided image
- Urinalysis (haematuria, infection) + renal function.
- USG = first-line: shows pelvicalyceal dilatation, radiation-free (children/pregnancy).
- NCCT KUB = gold standard for stones: size, site, detects radiolucent uric-acid stones.
- Diuretic MAG3 renography: confirms TRUE obstruction + split renal function.
- Metabolic work-up for recurrent stone formers.