Page 14 of 26
SU29.4-5 | Hydronephrosis and Renal Calculi — SDL Guide (Part 2)
Principles of Surgical Management
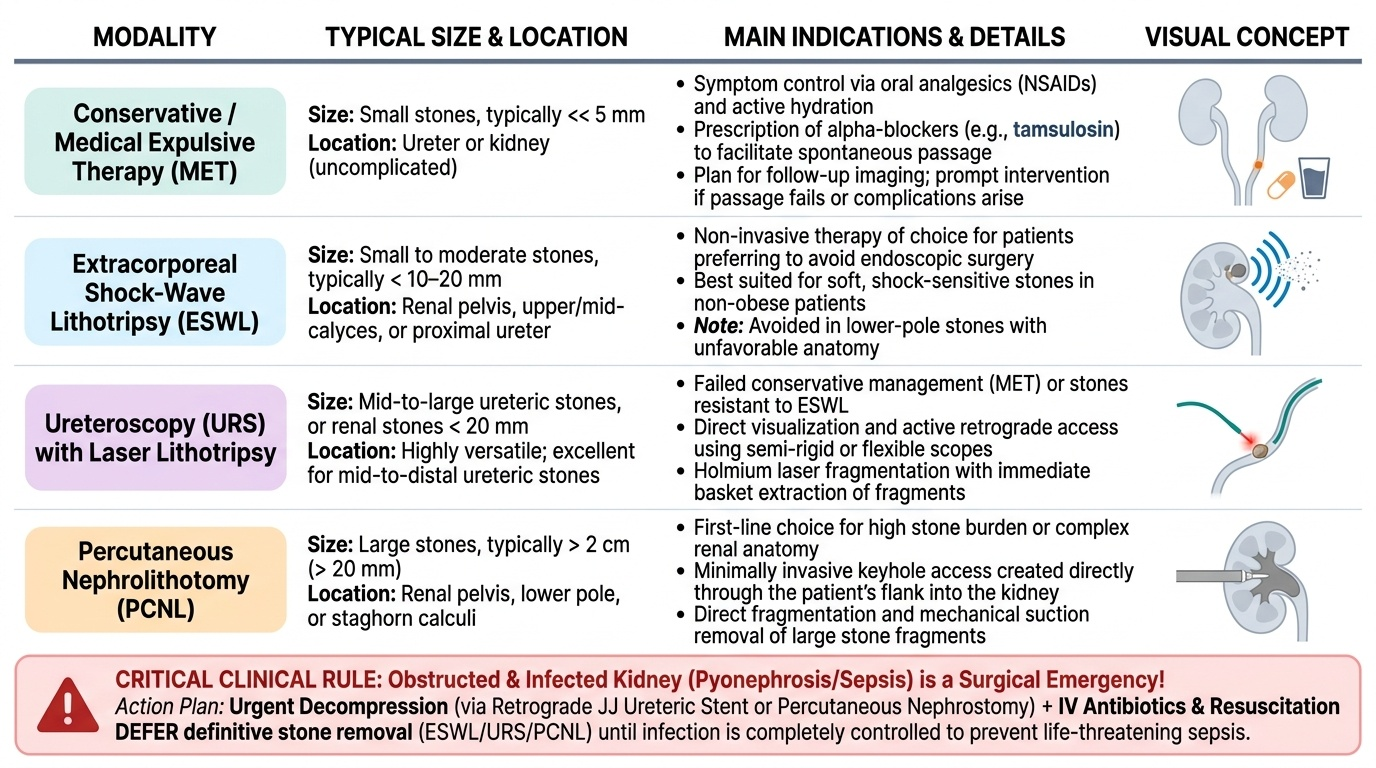
Management of both conditions rests on three principles applied in order: relieve the obstruction, treat the underlying cause, and preserve renal function — with one overriding rule of urgency. An obstructed, infected kidney (pyonephrosis or an obstructing stone with sepsis) is a surgical emergency: the priority is urgent decompression of the system by percutaneous nephrostomy or a retrograde JJ ureteric stent, together with intravenous antibiotics and resuscitation. Definitive removal of the stone is deferred until the infection is controlled — attempting primary stone surgery on an infected obstructed system can precipitate overwhelming sepsis. With that rule respected, the management of renal and ureteric calculi is largely size- and site-based. Small ureteric stones, typically less than 5 mm, usually pass spontaneously and are managed conservatively with analgesia (NSAIDs), hydration and medical expulsive therapy such as the alpha-blocker tamsulosin, with a plan to image and intervene if the stone fails to pass or the patient develops fever or uncontrolled pain. When intervention is needed, the modality is chosen by stone burden and location: extracorporeal shock-wave lithotripsy (ESWL) fragments suitable smaller stones non-invasively; ureteroscopy (URS) with laser lithotripsy is well suited to ureteric stones; and percutaneous nephrolithotomy (PCNL) is the procedure of choice for large or lower-pole stones and staghorn calculi (generally >2 cm). For hydronephrosis, treatment is directed at its cause: a pyeloplasty corrects PUJ obstruction; a stricture may be dilated, stented or reconstructed; bladder-outlet obstruction from BPH is relieved by catheterisation then definitive prostatic surgery; and an irreversibly damaged, non-functioning, infected kidney (confirmed on split function) may require nephrectomy. Throughout, renal function is protected by relieving obstruction promptly and treating infection, and prevention — high fluid intake, dietary modification and correction of any metabolic abnormality — reduces the high recurrence rate of stones. The whole plan is therefore a sequence: rule out the infected obstructed emergency first, then relieve and correct, then prevent.
Provided image
- EMERGENCY: obstructed + infected (pyonephrosis) → urgent decompression (nephrostomy or JJ stent) + antibiotics; defer definitive stone surgery.
- <5 mm ureteric stone → conservative + analgesia + medical expulsive therapy (tamsulosin).
- ESWL → suitable smaller stones (non-invasive).
- URS + laser → ureteric stones.
- PCNL → large / lower-pole / staghorn stones (>2 cm).
- Hydronephrosis: treat the cause — pyeloplasty (PUJ obstruction), relieve outlet obstruction, nephrectomy for a non-functioning infected kidney.
- Prevent: hydration, diet, correct metabolic cause.
CLINICAL PEARL
An obstructed kidney that becomes infected will not wait for definitive stone surgery. Faced with a febrile, septic patient and an obstructing ureteric stone with hydronephrosis, the correct first move is to DRAIN the system — a percutaneous nephrostomy or a JJ stent — and give antibiotics, NOT to take the patient straight to ureteroscopy or PCNL to remove the stone. Operating on pus under pressure can convert a salvageable kidney and a stable patient into urosepsis. Decompress and treat the infection first; remove the stone electively once the patient has recovered.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The restless 35-year-old with sudden colicky loin-to-groin pain, vomiting and pink urine has ureteric colic from a calculus: confirm with urinalysis and an NCCT KUB (the gold standard, which will find even a radiolucent uric-acid stone), and if the stone is small (under 5 mm) and the patient is afebrile, manage conservatively with analgesia and medical expulsive therapy — but escalate at once to decompression if he becomes febrile, because an obstructed infected stone is an emergency. The 60-year-old with a months-long dull ache and a ballottable loin mass has a chronic hydronephrosis: ultrasound will show the dilated pelvicalyceal system, and because the obstruction may be at the bladder outlet you must examine the prostate and bladder; a diuretic MAG3 renogram will confirm true obstruction and tell you whether the kidney is still worth saving. Use these to self-test the two competencies this module covers. First (SU29.4), can you define hydronephrosis, classify its causes by level (unilateral/ureteric versus bilateral/outlet, with pregnancy as physiological), name its investigations (USG first-line, MAG3 for true obstruction and split function) and state the principles of management (relieve obstruction, treat the cause, preserve function)? Second (SU29.5), can you classify renal calculi by composition (calcium oxalate commonest; struvite = infection/staghorn; uric acid = radiolucent; cystine inherited), give the clinical features of ureteric colic, name NCCT KUB as the gold-standard investigation, and outline size-based management (<5 mm conservative/MET, ESWL, URS+laser, PCNL for >2 cm/staghorn) including the obstructed-infected emergency? The questions that follow check exactly these links.
SELF-CHECK
A patient with an obstructing ureteric stone develops fever, rigors and tachycardia, with hydronephrosis on ultrasound. What is the most appropriate immediate management?
A. Immediate percutaneous nephrolithotomy to remove the stone
B. Urgent decompression with a nephrostomy or JJ stent plus intravenous antibiotics
C. Oral tamsulosin and discharge with analgesia
D. Extracorporeal shock-wave lithotripsy on the same admission
Reveal Answer
Answer: B. Urgent decompression with a nephrostomy or JJ stent plus intravenous antibiotics
This is an obstructed, infected upper urinary tract (impending pyonephrosis) — a surgical emergency. The system must be decompressed urgently by percutaneous nephrostomy or a retrograde JJ stent, with intravenous antibiotics and resuscitation. Definitive stone removal (PCNL, ESWL or ureteroscopy) is deferred until the infection is controlled; medical expulsive therapy and discharge would be dangerous in a septic, obstructed patient.